If you’re researching an old medical bill, deciphering a past diagnosis, or simply trying to understand a historical medical record, you’ve likely encountered the term “ICD-9 code for joint pain.” While this coding system is no longer in active use, it remains a crucial piece of the healthcare puzzle for millions of records. This guide is designed to be your clear, comprehensive resource. We’ll demystify what these codes mean, explain why they matter even today, and help you translate them into the modern medical coding language.
ICD-9 Codes for Joint Pain
A Brief History: Why ICD-9 Codes Still Matter
Before we dive into the specifics of joint pain, it’s essential to understand the context. The International Classification of Diseases, 9th Revision (ICD-9) was the standard system used by healthcare providers and insurers in the United States to code all diagnoses, symptoms, and procedures from 1979 until October 1, 2015.
On that date, the U.S. healthcare system officially transitioned to ICD-10, a much more detailed and modern system. However, any medical encounter you had before October 2015 will be documented using ICD-9 codes. This is why you might still be searching for them when:
-
Reviewing old medical bills or insurance statements.
-
Requesting your historical medical records.
-
Understanding the timeline of a chronic condition like arthritis.
-
Applying for long-term disability benefits based on past diagnoses.
Note: Healthcare providers and insurance companies cannot use ICD-9 codes for services rendered on or after October 1, 2015. Using an old ICD-9 code on a current bill is a red flag and likely an error.
The Primary ICD-9 Code for Joint Pain: 719.4x
In the ICD-9 system, joint pain is classified under a broader category for “Arthropathies and related disorders.” The primary code family is:
719.4 – Pain in joint
This is not a standalone, complete code. The fifth digit is required to specify the site of the joint pain. This is where the “x” comes in—you must replace it with a number that corresponds to a specific part of the body.
Breaking Down the Fifth Digit: Site Specification
Here is a table showing the complete ICD-9 codes for pain in specific joints:
| ICD-9 Code | Official Description |
|---|---|
| 719.40 | Pain in joint, site unspecified |
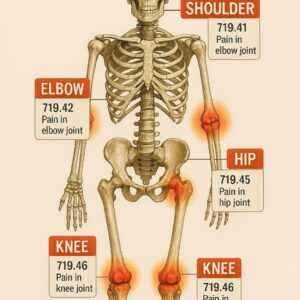
| 719.41 | Pain in joint, shoulder region |
| 719.42 | Pain in joint, upper arm |
| 719.43 | Pain in joint, forearm |
| 719.44 | Pain in joint, hand |
| 719.45 | Pain in joint, pelvic region and thigh |
| 719.46 | Pain in joint, lower leg |
| 719.47 | Pain in joint, ankle and foot |
| 719.48 | Pain in joint, other specified sites |
| 719.49 | Pain in joint, multiple sites |
As you can see, the most commonly searched code, “icd 9 code for joint pain” generally points to 719.40 (unspecified site) or a more specific code like 719.46 for knee pain.
What These Codes Did (and Did Not) Tell You
The 719.4x codes were used to indicate the symptom of pain. Crucially, they did not specify a cause. A code of 719.44 (pain in joint, hand) could apply equally to:
-
A patient with osteoarthritis.
-
A patient with rheumatoid arthritis.
-
A patient with gout.
-
A patient with a recent strain or injury.
-
A patient with unexplained arthralgia.
For the underlying disease, a separate ICD-9 code would be used. For example:
-
715.9x: Osteoarthritis, unspecified (e.g., 715.96 for osteoarthritis of the lower leg, knee).
-
714.0: Rheumatoid arthritis.
-
274.9: Gout, unspecified.
Key Distinctions and Related ICD-9 Codes
To avoid confusion, it’s helpful to understand codes for related but distinct conditions.
Arthralgia vs. Arthritis
-
Arthralgia (719.4x): This is the medical term for joint pain without obvious inflammation. The 719.4x codes were essentially codes for arthralgia.
-
Arthritis: This refers to joint pain with inflammation and structural change. It has its own set of codes (like the 715.xx, 714.xx series mentioned above). A patient could have both codes listed.
Polyarthralgia (Pain in Multiple Joints)
For pain in multiple joints, the correct ICD-9 code was 719.49 – Pain in joint, multiple sites.
The “Unspecified” Code: 719.40
This was often used as a default when the documentation wasn’t clear on the exact site, or for generalized joint pain. In modern ICD-10, there is much greater pressure to specify the site to avoid using unspecified codes whenever possible.
The Modern Equivalent: Transitioning from ICD-9 to ICD-10
Understanding the ICD-10 equivalents is vital because it helps bridge your historical records with current medical language. The ICD-10 system is exponentially more detailed.
The core ICD-10 code family for joint pain is M25.5- (Pain in joint).
Here’s a comparative table to illustrate the transition:
| Condition | ICD-9 Code | ICD-10 Code | Key Difference |
|---|---|---|---|
| Knee Pain, Unspecified | 719.46 | M25.561 (Pain in right knee) / M25.562 (Pain in left knee) | ICD-10 requires laterality (right/left). |
| Multiple Joint Pain | 719.49 | M25.50 (Pain in unspecified joint) or multiple specific codes. | ICD-10 discourages unspecified site codes. |
| Hand Joint Pain | 719.44 | M25.54- (Pain in joints of hand). Further digits specify which hand. | Far greater specificity in location. |
| Polyarthralgia | 719.49 | M25.50 | Often coded more precisely in ICD-10. |
As you can see, the simple act of coding “knee pain” now requires knowing which knee. This level of detail improves patient care and epidemiological tracking but represents a significant change from the older system.
Practical Guide: How to Use This Information
For Patients and Individuals
-
Decoding Old Documents: If you see “719.46” on an old bill, you now know it meant pain in the knee joint at that time.
-
Medical History: You can better understand the chronology of your health. A progression from 719.46 (knee pain) to 715.96 (osteoarthritis of knee) in your records tells a story.
-
Appeals and Research: Having the correct terminology empowers you when discussing historical care with new doctors or clarifying billing issues.
Important Considerations for Accuracy
-
Coding is Complex: A single medical encounter often involves multiple codes—one for the symptom (pain), one for the underlying diagnosis (e.g., osteoarthritis), and codes for any procedures performed.
-
Context is King: The code 719.4x only tells you that joint pain was documented. It does not reveal severity, cause, or treatment.
-
Consult a Professional: For definitive interpretation of your medical records or complex billing questions, always consult your healthcare provider’s office or a medical billing specialist.
FAQs on ICD-9 Codes for Joint Pain
Q: I have an old bill with code 719.40. What does that mean?
A: Code 719.40 meant “pain in joint, site unspecified.” Your provider documented that you had joint pain, but the specific location wasn’t coded or wasn’t clear from the documentation at the time.
Q: What is the ICD-9 code for arthritis?
A: There isn’t just one. Arthritis is a category. Common ones include 715.9x for osteoarthritis (e.g., 715.96 for knee) and 714.0 for rheumatoid arthritis. These are different from pain codes (719.4x).
Q: Can a doctor use ICD-9 codes today?
A: No. For any service dated October 1, 2015, or later, the use of ICD-9 codes is prohibited for billing and reporting in the U.S. They must use ICD-10-CM codes.
Q: Why is the ICD-10 system better?
A: ICD-10 offers greater specificity (e.g., right vs. left, initial encounter vs. follow-up), which leads to more precise patient records, improved tracking of public health trends, and more accurate billing.
Q: How do I find out the exact diagnosis behind an old joint pain code?
A: You need to request the full medical records from that encounter from your healthcare provider. The diagnosis will be in the doctor’s notes, not just on the billing statement.
Conclusion
Navigating the world of medical codes, especially outdated ones like the ICD-9 code for joint pain, can feel like decoding a secret language. Remember that the core code 719.4x represented the symptom of joint pain, with the fifth digit pointing to its location. While this system has been replaced by the more precise ICD-10, understanding these historical codes remains key to unlocking your personal medical history, resolving old billing queries, and appreciating the evolution of modern healthcare documentation. Always use this knowledge as a starting point for informed conversations with healthcare professionals.
Additional Resource
For the official, current code set, visit the CDC’s ICD-10-CM page: Centers for Disease Control and Prevention – ICD-10. This is the authoritative source for today’s diagnostic codes.
Disclaimer: This article is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment, nor is it a guide for medical coding. Always seek the advice of your physician or a qualified health provider with any questions you may have regarding a medical condition or billing. For official coding, healthcare providers must use current, licensed code books and resources.
Author: The Professional Healthcare Writing Team
Date: FEBRUARY 04, 2026





