Navigating the world of medical billing and coding can feel like learning a new language. If you’re searching for the ICD 9 code for jaundice, you’ve likely encountered a crucial piece of historical healthcare documentation. While the ICD-9-CM (International Classification of Diseases, 9th Revision, Clinical Modification) was officially replaced by ICD-10 in 2015, understanding its codes remains essential for dealing with older medical records, certain insurance claims, and historical data analysis.
This guide will provide a comprehensive, clear breakdown of how jaundice was classified under ICD-9. We’ll explore the specific codes, their meanings, and the critical importance of context in choosing the right one. Our goal is to make this technical topic accessible and give you the knowledge to understand these codes confidently.
ICD-9 Code for Jaundice
Understanding Jaundice and Its Historical Coding
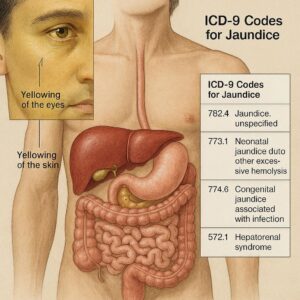
Before we dive into the numbers, let’s briefly recall what jaundice represents. Jaundice itself is not a disease but a clinical sign characterized by a yellowing of the skin, sclerae (whites of the eyes), and mucous membranes. This yellow hue is caused by an excess of bilirubin, a yellow pigment formed during the normal breakdown of red blood cells. The underlying cause can be pre-hepatic (like hemolytic anemia), hepatic (involving the liver itself, such as hepatitis), or post-hepatic (obstructive, like a gallstone blocking the bile duct).
In ICD-9, this need to distinguish the cause or context of the jaundice was paramount. There wasn’t just one universal code. Instead, medical coders had to select from several codes across different chapters of the coding manual, depending on the physician’s documented diagnosis.
The Primary ICD-9 Codes for Jaundice
Here are the main ICD-9 codes you would encounter for jaundice, each telling a different story about the patient’s condition.
1. ICD-9 Code 782.4: Jaundice, Unspecified, Not of Newborn
This was often the default code when a patient presented with jaundice, but the underlying cause was not yet determined or specified in the documentation.
-
Category: Symptoms, signs, and ill-defined conditions (Chapter 16).
-
Usage: This code was used for jaundice as a presenting symptom. It was a temporary placeholder when the cause was unknown or when a more specific code couldn’t be applied. For billing, using this code often triggered requests for more information from payers.
2. ICD-9 Code 277.4: Disorders of Bilirubin Metabolism
This code family was used for specific, diagnosed disorders that directly affect bilirubin processing.
-
Subcategories:
-
277.40: Disorder of bilirubin metabolism, unspecified
-
277.41: Constitutional hepatic dysfunction (Gilbert’s syndrome)
-
277.49: Other disorders of bilirubin metabolism (e.g., Crigler-Najjar syndrome, Dubin-Johnson syndrome)
-
-
Usage: This code was assigned for chronic, often inherited, conditions that cause jaundice without significant liver cell damage.
3. ICD-9 Code 774.xx: Perinatal Jaundice
This entire series was reserved exclusively for jaundice in newborns.
-
Key Examples:
-
774.0: Perinatal jaundice from hereditary hemolysis (e.g., due to ABO or Rh incompatibility).
-
774.1: Perinatal jaundice from other excessive hemolysis.
-
774.2: Neonatal jaundice associated with preterm delivery.
-
774.30: Neonatal jaundice due to delayed conjugation from other causes.
-
774.39: Other perinatal jaundice.
-
774.6: Unspecified fetal and neonatal jaundice.
-
-
Usage: Crucial for pediatric and obstetric coding, this category allowed for precise differentiation of the cause of newborn jaundice, which is extremely common and often managed differently than in adults.
Comparative Table: ICD-9 Codes for Jaundice at a Glance
| ICD-9 Code | Code Description | Primary Context | Typical Use Case |
|---|---|---|---|
| 782.4 | Jaundice, unspecified, not of newborn | Symptom | Adult patient presents with yellow skin; cause is unknown or pending investigation. |
| 277.41 | Constitutional hepatic dysfunction (Gilbert’s syndrome) | Chronic Disorder | Patient with mild, intermittent jaundice, especially during illness or fasting, with normal liver function tests. |
| 277.49 | Other disorders of bilirubin metabolism | Chronic Disorder | Diagnoses like Crigler-Najjar or Dubin-Johnson syndrome. |
| 774.0 | Perinatal jaundice from hemolysis | Newborn | Jaundiced newborn with laboratory confirmation of ABO incompatibility. |
| 774.2 | Neonatal jaundice with preterm delivery | Newborn | Jaundice in a baby born at 34 weeks gestation. |
| 774.6 | Unspecified fetal and neonatal jaundice | Newborn | Jaundice in a newborn where a more specific cause is not documented. |
The Critical Importance of Specificity in ICD-9 Coding
A core principle in medical coding—both in ICD-9 and its successor—is specificity. The code must reflect the physician’s documentation as accurately as possible. Coding jaundice as a symptom (782.4) when the diagnosed cause is viral hepatitis (which had its own code series, like 070.1 for hepatitis A with hepatic coma) would be incorrect and could lead to claim denials or inaccurate data.
Expert Insight: “In the ICD-9 era, the difference between coding 782.4 and a more specific code like 570 (acute and subacute necrosis of the liver) wasn’t just bureaucratic. It directly impacted reimbursement rates, quality of care statistics, and public health tracking. The coder’s role was to be a precise translator of clinical notes into data.” – Senior Medical Coding Auditor.
How Underlying Causes Were Coded
Jaundice frequently appears as a symptom of a larger problem. Here’s how some common underlying conditions were coded in ICD-9:
-
Viral Hepatitis: Codes under 070.x (e.g., 070.1 Viral hepatitis A with hepatic coma, 070.30 Hepatitis B without mention of hepatic coma).
-
Alcoholic Liver Disease: Codes under 571.x (e.g., 571.1 Acute alcoholic hepatitis, 571.2 Alcoholic cirrhosis of liver).
-
Cholelithiasis (Gallstones) with Obstruction: 574.xx series (e.g., 574.11 Calculus of gallbladder with acute cholecystitis with obstruction).
-
Malignant Neoplasm of Liver and Intrahepatic Bile Ducts: 155.xx
-
Hemolytic Anemias: Codes under 282-283.
In these cases, the code for the underlying disease would be listed as the primary diagnosis, and a code like 782.4 might sometimes be added as a secondary diagnosis to further specify the patient’s presentation, though this was not always necessary or beneficial for billing.
The Transition from ICD-9 to ICD-10: A World of Difference
The shift to ICD-10-CM on October 1, 2015, was monumental. For conditions like jaundice, it moved coding from a system of limited options to one of extensive detail.
Key Changes for Jaundice Coding:
-
Increased Specificity: ICD-10 offers vastly more codes to describe etiology, laterality, and acuity.
-
Consolidation and Reorganization: The “symptom” code for jaundice is now R17, “Unspecified jaundice.” However, it is strongly discouraged in favor of more specific codes.
-
Newborn Jaundice: Codes are now under P58.x and P59.x, allowing even more granularity about the cause of neonatal jaundice.
-
Example of Detail: In ICD-10, you can code for K83.1 (Obstruction of bile duct), and then add additional codes for the cause of the obstruction (like a gallstone, K80.xx) and the presence of jaundice.
A Helpful Comparison: ICD-9 vs. ICD-10 for a Common Scenario
| Scenario | ICD-9 Coding | ICD-10 Coding |
|---|---|---|
| A 45-year-old patient with jaundice caused by a gallstone obstructing the common bile duct. | Primary: 574.11 (Calculus of gallbladder with acute cholecystitis with obstruction) Possible Secondary: 782.4 |
Primary: K80.43 (Calculus of bile duct with acute cholecystitis with obstruction) Secondary: K83.1 (Obstruction of bile duct) Additional: R17 (Unspecified jaundice) – likely not needed as obstruction implies jaundice. |
Important Note for Readers: If you are coding for a current healthcare encounter in the United States after October 2015, you must use ICD-10-CM codes. Using ICD-9 for current services will result in claim rejection. This article’s primary value is for historical record review, understanding older documents, or academic purposes.
Why Understanding ICD-9 Codes Still Matters
You might wonder why we’re discussing a retired coding system. The reasons are practical:
-
Medical Record Review: Patients’ histories span decades. Older records, consultation notes, and past surgical reports will reference ICD-9 codes.
-
Long-term Disability and Insurance Claims: Some ongoing claims or appeals may reference the original ICD-9 code from the time of diagnosis.
-
Research and Data Analysis: Epidemiological studies tracking disease trends over time must reconcile data from both the ICD-9 and ICD-10 eras.
-
Professional Knowledge: For medical coders, billers, and auditors, understanding the evolution of coding systems is a mark of comprehensive expertise.
A Step-by-Step Guide to Interpreting an Old ICD-9 Code for Jaundice
If you find an ICD-9 code on an old document, follow this logic:
-
Identify the Code: Note the exact numeric code (e.g., 774.0).
-
Check the Category:
-
77x: It’s related to a newborn. Consider birth history and timing.
-
782.4: It was documented as a symptom without a specified cause at that time.
-
277.4: It indicates a diagnosed, often chronic, disorder of bilirubin metabolism.
-
57x, 07x, etc.: The jaundice was a symptom of a specific liver or gallbladder disease listed as the primary diagnosis.
-
-
Seek Context: The code alone is a data point. The full medical record narrative provides the true story.
Conclusion
Finding the correct ICD 9 code for jaundice was never about a single number; it was a diagnostic puzzle requiring the coder to match the physician’s clinical findings to the most precise code available in the system. Whether it was the symptomatic code 782.4, the disorder-specific 277.4, or one of the many newborn codes in the 774 series, each served a distinct purpose in painting an accurate picture of the patient’s health for data, billing, and care continuity. While ICD-10 has brought necessary detail and clarity, the logic and principles of ICD-9 remain a foundational part of medical data history.
Frequently Asked Questions (FAQ)
Q: What is the most common ICD-9 code for jaundice in adults?
A: For unspecified jaundice where the cause wasn’t documented, code 782.4 (Jaundice, unspecified, not of newborn) was the most commonly used. However, if a cause was known, a more specific code for that condition (like for hepatitis or cirrhosis) would be used instead.
Q: Can I use ICD-9 codes for medical billing today?
A: No. As of October 1, 2015, all healthcare providers covered by the Health Insurance Portability and Accountability Act (HIPAA) in the U.S. are required to use ICD-10-CM for diagnosis coding. Using ICD-9 will result in claim denials.
Q: How do I code jaundice in a newborn in ICD-9?
A: You would use a code from the 774.xx series. The specific code depends on the cause (e.g., hemolysis, prematurity) as documented by the physician. 774.6 was used for unspecified neonatal jaundice.
Q: What is the ICD-10 equivalent of ICD-9 code 782.4?
A: The closest equivalent is R17, “Unspecified jaundice.” However, ICD-10 strongly encourages the use of more specific codes whenever possible (e.g., R17.0 for hyperbilirubinemia with other liver issues, or codes for the specific disease causing the jaundice).
Q: Why are there so many different codes for jaundice?
A: Because jaundice is a symptom, not a final diagnosis. The coding system aims to capture the underlying reason for the symptom to ensure accurate treatment, proper reimbursement for the complexity of care, and correct data for public health tracking.
Additional Resources
For the most current and official coding guidelines and tools, always refer to authoritative sources:
-
Centers for Disease Control and Prevention (CDC) ICD-10-CM Browser: https://www.cdc.gov/nchs/icd/icd10cm.htm (For current coding)
-
American Medical Association (AMA): Provides CPT and coding resources.
-
The American Health Information Management Association (AHIMA): A leading resource for health information and coding professionals.
Disclaimer: This article is for informational and educational purposes only. It is not a substitute for professional medical coding advice, official coding guidelines, or physician consultation. Medical coding is complex and regulated; always consult the most current official code sets and guidelines from the CDC and CMS for all billing and coding activities. The author and publisher are not responsible for any errors, omissions, or consequences resulting from the use of this information.
Author: The Medical Coding Guide Team
Date: FEBRUARY 05, 2026





