If you are reading this, you probably have a patient with a large kidney stone. You know that percutaneous nephrolithotomy (PCNL) is the right procedure. But now you need the correct CPT code. And not just any code. You need the code that reflects exactly what you did, avoids denials, and ensures fair reimbursement.
Let us be honest. Urology coding can feel like walking through a maze. One small miss can cost your practice thousands of dollars. But do not worry. This guide walks you through every important detail about the CPT code for percutaneous nephrolithotomy. We will keep things simple, clear, and practical.
By the end of this article, you will know exactly which code to use, when to add modifiers, and how to document like a pro.
CPT Code for Percutaneous Nephrolithotomy
What Is Percutaneous Nephrolithotomy (PCNL)?
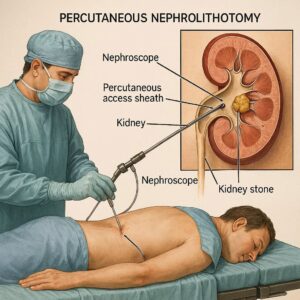
Before we talk about codes, let us quickly define the procedure. Percutaneous nephrolithotomy is a surgical technique to remove large or complex kidney stones. The surgeon makes a small incision in the patient’s back. Then, they pass a scope directly into the kidney through this tract. Once inside, they break up the stone and remove the fragments.
This is not a routine procedure. Doctors usually recommend PCNL for stones larger than 2 cm, staghorn calculi, or stones that did not respond to shock wave lithotripsy or ureteroscopy.
Note for coders: Understanding the procedure’s complexity helps you choose the right code. PCNL is more invasive than ureteroscopy but less invasive than open surgery.
The Primary CPT Code for Percutaneous Nephrolithotomy
Let us get straight to the answer.
The main CPT code for percutaneous nephrolithotomy is 50080.
But wait. There is more. The code changed in recent years. You need to pay attention to the current version.
CPT 50080 – Percutaneous nephrolithotomy, including pre-operative tract dilation and post-operative nephrostomy tube placement
This code covers:
-
Access into the kidney through the skin
-
Dilation of the tract
-
Introduction of a nephroscope
-
Stone fragmentation (laser, ultrasound, or pneumatic)
-
Stone extraction
-
Placement of a nephrostomy tube at the end
Sounds complete, right? In many cases, yes. However, there is a second code you should know.
CPT 50081 – Percutaneous nephrolithotomy, complex
Complex cases require extra work. These include:
-
Stones in a calyceal diverticulum
-
Stones in a horseshoe kidney
-
Multiple tracts
-
Stones requiring additional endoscopy or ancillary procedures
-
Patients with abnormal anatomy
When should you use 50081? Use it when the procedure takes significantly more time, skill, and effort than a standard PCNL.
Let us compare them side by side.
| Feature | CPT 50080 (Standard) | CPT 50081 (Complex) |
|---|---|---|
| Stone size | Usually >2 cm | Any size with complexity |
| Anatomy | Normal | Abnormal or surgically altered |
| Tracts | Single tract | Multiple tracts possible |
| Additional procedures | No | Yes (e.g., ESWL, ureteroscopy) |
| Reimbursement | Lower | Higher |
| Documentation required | Standard | Extensive |
What Is Not Included in These Codes?
Many coders assume the PCNL code covers everything. That is a mistake. Both 50080 and 50081 do not include:
-
Diagnostic nephrostography or antegrade pyelogram (if done separately before the procedure)
-
Ureteral stent placement (unless explicitly documented as part of PCNL)
-
Second or separate access site (may require modifier or separate code)
-
Treatment of contralateral kidney (separate code and modifier)
-
Open surgical conversion (different code set)
Always read the full CPT descriptor. Do not guess.
When to Use Modifiers with PCNL Codes
Modifiers are not optional. They tell the payer that something changed. Here are the most common modifiers for percutaneous nephrolithotomy coding.
Modifier 22 – Increased Procedural Services
Use modifier 22 when the work is substantially greater than typical. For example:
-
Extremely large staghorn calculus
-
Severe adhesions or scarring
-
Unusually difficult anatomy
Important: You must attach a clear operative note. Describe why this case was harder. Payers deny modifier 22 without strong documentation.
Modifier 50 – Bilateral Procedure
If you perform PCNL on both kidneys during the same session, append modifier 50 to the primary code. Do not report two units of 50080 or 50081. Use one line with modifier 50.
Modifier 58 – Staged or Related Procedure
Sometimes, you plan a second PCNL session. For example, you remove most of the stone but leave a small fragment for later. If the second session is planned within the postoperative period, use modifier 58.
Modifier 78 – Unplanned Return to the OR
If the patient returns to the operating room for a complication (bleeding, retained stone fragment), use modifier 78. This is not the same as a planned second look.
Modifier 79 – Unrelated Procedure
Rare in PCNL, but possible. If the patient needs an unrelated surgery during the postoperative period, modifier 79 applies.
Documentation Requirements for PCNL Coding
You cannot code what you cannot prove. Documentation must be precise. Here is what payers expect.
Operative Report Must Include:
-
Indication for PCNL (stone size, location, composition if known)
-
Description of access method (ultrasound vs. fluoroscopy)
-
Number of tracts created
-
Type of energy used for fragmentation (laser, ultrasound, etc.)
-
Method of stone removal (basketing, forceps, suction)
-
Confirmation of stone clearance (nephroscopy, fluoroscopy)
-
Placement of nephrostomy tube or stent
-
Any complications or unexpected findings
Sample Documentation Snippet:
“After obtaining percutaneous access to the lower pole calyx under fluoroscopic guidance, a guidewire was advanced. The tract was dilated to 30 French. A nephroscope was introduced. A 2.5 cm staghorn calculus was fragmented using a holmium laser. Fragments were removed with grasping forceps. Final nephroscopy revealed no residual fragments. A 22 French nephrostomy tube was placed.”
That is clear. That is billable.
Common Billing Mistakes with PCNL Codes
Even experienced billers slip up. Avoid these frequent errors.
Mistake #1: Using 50080 for a Complex Case
If you undercode, you lose money. If you overcode, you risk an audit. Know the difference. When in doubt, document complexity and use 50081.
Mistake #2: Billing for the Nephrostomy Tube Separately
Do not separately bill for placement of a nephrostomy tube. It is included in 50080 and 50081.
Mistake #3: Adding Unnecessary Modifiers
Modifier 59 (distinct procedural service) is rarely needed for PCNL. Do not add it unless truly separate and unrelated.
Mistake #4: Ignoring Global Period Rules
Both 50080 and 50081 have a 90-day global period. All related postoperative care is included. You cannot bill separately for follow-up visits, stone analysis, or routine nephrostomy tube changes during that time.
How Do PCNL Codes Compare to Other Stone Procedures?
Understanding the differences helps you choose correctly.
| Procedure | CPT Code(s) | Best for | Invasive level |
|---|---|---|---|
| Shock wave lithotripsy (ESWL) | 50590 | Stones <2 cm, non-lower pole | Non-invasive |
| Ureteroscopy with laser | 52356 | Stones <2 cm, any location | Minimally invasive |
| Percutaneous nephrolithotomy | 50080, 50081 | Stones >2 cm, staghorn, complex | Minimally invasive but more than URS |
| Open nephrolithotomy | 50060-50075 | Failed PCNL, very large or complex stones | Open surgery |
Reader tip: Do not confuse PCNL with percutaneous nephrostomy (CPT 50395). The latter is only for drainage, not stone removal.
Real-World Scenarios: Which Code Should You Pick?
Let us walk through a few patient cases.
Scenario 1 – Standard PCNL
A 55-year-old male has a 2.3 cm renal pelvic stone. Normal anatomy. Single percutaneous tract. Holmium laser used. Stone completely cleared. Nephrostomy tube placed.
Code: 50080
Scenario 2 – Complex PCNL
A 62-year-old female has a 3.5 cm staghorn calculus in a horseshoe kidney. The surgeon creates two separate tracts. Uses both laser and ultrasonic fragmentation. Takes 3.5 hours.
Code: 50081 with modifier 22 (if significantly more work than typical complex case)
Scenario 3 – Bilateral PCNL
Same patient, but stones in both kidneys. The surgeon performs PCNL on the right kidney, then the left kidney in the same operative session.
Code: 50080 with modifier 50 (or 50081-50 if complex bilaterally)
Scenario 4 – Second Look PCNL
The patient returns 2 weeks later for a planned second procedure to remove a residual fragment seen on postoperative imaging.
Code: 50080 with modifier 58
Reimbursement Tips for Percutaneous Nephrolithotomy
Getting paid correctly requires more than the right code.
Tip 1 – Know Your Payer
Medicare, Medicaid, and commercial insurers have different rules. Some require prior authorization for PCNL. Others deny 50081 without supporting documentation.
Tip 2 – Use the Correct Place of Service
PCNL is a hospital outpatient or inpatient procedure. Do not bill it as an office procedure.
Tip 3 – Check National and Local Coverage Determinations (NCD/LCD)
Medicare LCDs sometimes list specific indications for PCNL. If your patient does not meet these criteria, expect a denial.
Tip 4 – Appeal Denials Quickly
If a payer denies 50081 and asks for 50080, appeal with the operative note. Highlight the complex features.
Tip 5 – Track Your Days in the Global Period
During the 90-day global period, you can still bill for:
-
Unrelated procedures (modifier 79)
-
Significant complications requiring return to OR (modifier 78)
-
New problems unrelated to the stone (e.g., UTI from another cause)
But you cannot bill for:
-
Routine postoperative visits
-
Stone analysis (CPT 82365 – included)
-
Nephrostomy tube changes without complication
Important Notes for Readers
Note 1: CPT codes are updated annually. The codes discussed here (50080 and 50081) are current as of 2026. Always verify with the latest AMA CPT manual.
Note 2: This guide is for educational purposes. It does not replace legal, payer, or compliance advice. When in doubt, consult a certified professional coder.
Note 3: Never copy and paste another provider’s op note. Payers use software to detect cloned documentation.
Frequently Asked Questions (FAQ)
1. Is CPT 50080 the same as a nephrostomy tube placement?
No. A nephrostomy tube placement alone is CPT 50395. PCNL includes stone removal and tube placement.
2. Can I bill for ultrasound guidance during PCNL?
No. Ultrasound guidance for access is included in the PCNL code. Do not bill it separately.
3. What if the stone is removed but no nephrostomy tube is placed?
Some surgeons place a ureteral stent instead. The code (50080 or 50081) still applies. Tube placement is not mandatory for coding.
4. How do I code for PCNL with antegrade ureteroscopy?
If the surgeon passes the scope down the ureter to treat a stone, this is still part of PCNL if done through the same tract. No separate code. If a second access is needed, document and consider modifier 22.
5. What is the difference between 50080 and 50590?
50080 is PCNL (through the back into the kidney). 50590 is shock wave lithotripsy (non-invasive, no incision).
6. Can a non-urologist perform PCNL?
In rare cases, interventional radiologists perform percutaneous stone removal. They should use the same CPT codes if they perform the full procedure.
7. What happens if I use the wrong PCNL code?
You may receive a denial, a downcode, or a post-payment audit. Correct coding reduces risk.
Additional Resource
For official coding guidance, always refer to the American Urological Association (AUA) Coding and Reimbursement Resource Center.
👉 AUA Coding Resources – External Link
This is a trusted, non-commercial source for urology-specific coding updates, modifiers, and payer policy examples.
Conclusion
Choosing the correct CPT code for percutaneous nephrolithotomy comes down to understanding the procedure’s scope and complexity. Use CPT 50080 for standard PCNL with a single tract and normal anatomy. Use CPT 50081 for complex cases requiring extra work, multiple tracts, or abnormal anatomy. Always document thoroughly, apply modifiers only when needed, and respect the 90-day global period. With this guide, you can bill with confidence and reduce unnecessary denials.
Disclaimer: This article is for informational purposes only and does not constitute legal, medical, or billing advice. Coding rules vary by payer and region. Always consult a certified professional coder or your compliance department before submitting claims.
Author: Professional Medical Coding Writer – Urology Focus
Date: April 09, 2026





