Navigating the world of medical billing for durable medical equipment (DME) can often feel like trying to solve a complex puzzle. If you are a healthcare provider, a medical biller, or even a patient trying to understand why a specific brace costs what it does, you have likely run into the confusing question: What is the correct code for an ankle brace?
First, let’s clear up a common misconception. When we talk about billing for a physical item like a brace, we aren’t actually looking at “CPT” (Current Procedural Terminology) codes in the traditional sense. CPT codes usually describe a service or a procedure performed by a clinician—like an evaluation or a surgery. For the brace itself, we use HCPCS Level II codes (Healthcare Common Procedure Coding System).
These are the alpha-numeric codes that insurance companies require to identify the specific type of device being provided.
In this guide, we will strip away the jargon and walk you through everything you need to know about coding for ankle brace support. Whether you are dealing with a simple elastic sleeve or a rigid, custom-fabricated orthotic, we will cover the right codes, the documentation requirements, and how to avoid the dreaded denial letter.
CPT Codes for Ankle Brace Support
Table of Contents
ToggleUnderstanding HCPCS vs. CPT for Orthotics
Before we dive into the specific codes, it is vital to understand the difference. Many people search for “CPT code for ankle brace support” expecting a single five-digit number, but the reality is a bit different.
CPT codes are reserved for the action of fitting the brace. For example, if a doctor spends time measuring, fitting, and educating a patient on how to use a custom brace, you might bill a CPT code like 97760 (Orthotic(s) management and training). However, the brace itself—the physical product—is billed using HCPCS codes.
HCPCS Level II codes are managed by the Centers for Medicare & Medicaid Services (CMS). These codes define the specific class of brace:
-
L-Codes: These are the most common for orthotics. They cover everything from pre-fabricated (off-the-shelf) braces to custom-fabricated devices.
-
A-Codes: Sometimes used for supplies, but rarely for the primary ankle brace structure.
When billing insurance, you will almost always be pairing a HCPCS code (the brace) with a CPT code (the fitting service, if applicable), along with a diagnosis code (ICD-10) that proves medical necessity.
The Main HCPCS Codes for Ankle Braces
There is no single “one size fits all” code. The correct code depends entirely on the rigidity of the brace, the material, and whether it was custom-made for the patient or purchased straight off the shelf.
Let’s break these down into three main categories: Soft Supports, Rigid Braces, and Custom Devices.
L-Codes for Soft Ankle Supports (Elastic/Neoprene)
Soft braces are typically used for mild sprains, proprioception, or chronic instability. They are usually “off-the-shelf” (OTS) items that require minimal fitting.
| HCPCS Code | Description | Typical Use Case |
|---|---|---|
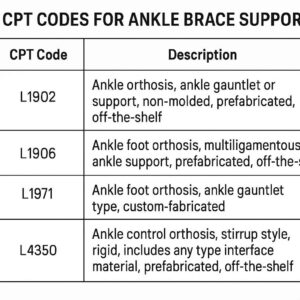
| L1902 | Ankle orthosis, ankle gauntlet (prefabricated) | A lace-up or wrap-around brace that covers the ankle and midfoot. Used for mild instability or tendinitis. |
| L1904 | Ankle orthosis, ankle gauntlet (custom fabricated) | A custom-molded version of a soft support, usually made from thermoplastics for a specific patient shape. Rarely used for purely soft supports. |
| L1906 | Ankle foot orthosis (AFO), prefabricated, with joint(s) | A rigid or semi-rigid plastic brace that extends from the calf to the foot. This is a step up from a gauntlet, often used for drop foot or significant instability. |
| L1907 | Ankle foot orthosis (AFO), prefabricated, without joint(s) | A solid-shell AFO that prevents all ankle motion. |
Important Note: For simple elastic sleeves or “ACE bandage” type supports, there is often no HCPCS code that allows for separate reimbursement. These are frequently considered “non-covered” or supplies that are bundled into the office visit cost.
L-Codes for Rigid and Hinged Braces
When a patient suffers from a moderate to severe sprain, ligament tears, or post-operative recovery, they require a brace that restricts motion to allow healing. These are often hinged or rigid designs.
| HCPCS Code | Description | Typical Use Case |
|---|---|---|
| L1970 | Ankle foot orthosis (AFO), prefabricated, with ankle joint, plastic or other material | This is one of the most common codes for a “walking boot” or a rigid, hinged plastic brace that allows some controlled motion while protecting the ankle. |
| L1980 | Ankle foot orthosis (AFO), prefabricated, with ankle joint, metal | A more heavy-duty metal upright brace, often used for chronic paralysis or severe weakness, less common for acute sprains. |
| L2275 | Addition to lower extremity orthosis, varus/valgus correction | Used when adding specialized pads or wedges to a brace to correct alignment issues. |
| L2820 | Addition to lower extremity orthosis, soft interface | Used for adding padding to a rigid brace to improve comfort. |
L-Codes for Custom Fabricated Braces
If a brace is “custom fabricated,” it means it is not simply adjusted from a shelf; it is built specifically for the patient’s anatomy based on a cast, scan, or detailed tracing. These require significantly more documentation and usually a higher reimbursement rate.
| HCPCS Code | Description | Typical Use Case |
|---|---|---|
| L2106 | Ankle foot orthosis, fracture orthosis, walking boot type, prefabricated | Wait—this says prefabricated. It is important to distinguish. True custom rigid braces fall under L2108, L2112, etc. |
| L2108 | Ankle foot orthosis, fracture orthosis, walking boot type, custom fabricated | A walking boot that is custom-molded to the patient’s leg and foot, typically used for complex fractures or non-healing wounds where a prefabricated boot would cause pressure issues. |
| L1907 (Custom modifier) | Ankle foot orthosis, custom fabricated, without joints | A solid custom-molded plastic AFO used for patients with fixed deformities or neurological conditions like stroke. |
How to Determine Medical Necessity
Insurance companies do not just ask “What brace did you give?” They ask, “Why did you give it?”
Medical necessity is the golden key to getting a claim paid. If the medical records do not support the level of brace you billed for, the claim will be denied. Here is how the severity usually aligns with the codes:
-
Mild Conditions: If the patient has a Grade 1 sprain or mild tendinitis, a soft gauntlet (L1902) is usually appropriate.
-
Moderate Conditions: For Grade 2 sprains, post-operative status after arthroscopy, or severe tendonitis, a hinged or rigid walking boot (L1970) is the standard.
-
Severe Conditions: For chronic neurological conditions (like stroke or cerebral palsy), Charcot foot, or non-healing fractures, a custom fabricated AFO (L1907 or L2108) is required.
The Role of ICD-10 Codes
You cannot bill an ankle brace without a matching diagnosis. Common diagnoses that support ankle brace necessity include:
-
S93.401A: Sprain of unspecified ligament of ankle (initial encounter).
-
M25.571: Pain in right ankle.
-
G72.81: Critical illness myopathy (for drop foot).
-
M21.271: Fixed deformity, right ankle.
-
Z96.6: Presence of orthopedic joint implant (post-surgical).
If you bill L1970 (rigid walking boot) for M25.571 (ankle pain) without mention of instability, weight-bearing restrictions, or a specific injury, you will likely face a denial.
The “KX” Modifier and Advance Beneficiary Notice (ABN)
One of the trickiest aspects of billing for ankle braces, particularly for Medicare beneficiaries, involves modifiers.
The KX Modifier
For certain high-cost orthotics (like custom fabricated braces), Medicare requires that specific documentation criteria are met. Adding the KX Modifier to the HCPCS code is your way of certifying, “Yes, I have the documentation on file proving this was medically necessary and the patient met the coverage criteria.”
-
If you don’t append KX when required? Denial.
-
If you append KX without the documentation? That is fraud.
The GA and GZ Modifiers
If you are providing a brace that you suspect Medicare will not cover (perhaps it is for comfort rather than function), you must have the patient sign an Advance Beneficiary Notice (ABN).
-
GA Modifier: You have a signed ABN on file. Medicare will likely deny it, but the patient is responsible for payment.
-
GZ Modifier: You did not get an ABN, and you suspect Medicare will deny it. The provider is liable for the cost, and you cannot bill the patient.
Documentation Requirements: The “Big 3”
To ensure your claim survives an audit, your medical records must contain three critical elements. I like to call these the “Big 3” of orthotic billing.
1. The Detailed Written Order (DWO)
A verbal order is not enough for DME. You must have a Detailed Written Order signed and dated by the treating practitioner before or on the date of delivery.
-
The DWO must specify the item (e.g., “L1970 – Rigid Hinged Walking Boot”).
-
It must specify the length of need (e.g., “6 weeks” or “indefinite”).
-
For custom braces, the DWO must explicitly state “custom fabricated.”
2. The Face-to-Face Encounter
For certain high-level orthotics (and especially for Medicare patients), a face-to-face encounter must have occurred within the 6 months prior to the order. The medical record must clearly document that the practitioner evaluated the patient and determined the orthotic was necessary.
3. The Medical Record Notes
The clinical notes must answer “Why?” They should document:
-
The patient’s functional limitation (e.g., “Patient is unable to bear weight without risk of fracture displacement”).
-
The specific diagnosis.
-
Why a lower-level brace (like a simple elastic wrap) is insufficient.
-
The expected duration of use.
Common Billing Scenarios and Coding Examples
Let’s look at a few realistic scenarios to see how these codes work in practice.
Scenario 1: The Acute Ankle Sprain
A 28-year-old athlete rolls their ankle during a basketball game. The physician diagnoses a Grade 2 lateral ligament sprain. The patient needs to protect the ankle but still walk. The provider dispenses a pneumatic walking boot (rigid with hinges) from their office stock.
-
HCPCS Code: L1970 (AFO, prefabricated, with ankle joint, plastic)
-
Modifier: RT (Right side) or LT (Left side). If it is the first brace of this type, use RA (Replacement) is not applicable here.
-
Diagnosis: S93.401A
-
CPT for Fitting: 97760 (if the provider spent time training the patient on how to use the pneumatic compression).
Scenario 2: The Post-Operative Recovery
A 65-year-old Medicare patient undergoes a bunionectomy (foot surgery). The surgeon requires the patient to remain non-weight-bearing for two weeks, followed by six weeks in a walking boot to protect the surgical site. The boot is provided by an external DME supplier.
-
HCPCS Code: L1970
-
Modifier: KX (The supplier must ensure the documentation proves the boot is necessary for post-surgical recovery; for Medicare, post-surgical boots usually require the KX modifier to confirm necessity).
-
Diagnosis: Z96.6 or the specific post-op diagnosis.
-
Important: The DME supplier needs the Detailed Written Order before dispensing.
Scenario 3: Chronic Instability & Custom Fitting
A 45-year-old with Charcot-Marie-Tooth disease experiences progressive foot drop and instability. Over-the-counter braces are causing skin breakdown due to the patient’s unique foot shape. A physiatrist creates a plaster cast of the leg, and a custom-fabricated carbon fiber AFO is created.
-
HCPCS Code: L1907 (AFO, custom fabricated, without joints) – depending on the design, it could also be L1970 with a custom modifier.
-
Modifier: KX (mandatory for Medicare custom orthotics) and RT/LT.
-
Diagnosis: G60.0 (Hereditary motor and sensory neuropathy).
-
CPT for Fitting: 97760 (Orthotic management and training, 15 minutes) – this is billable in addition to the brace itself, as custom fitting requires significant professional time.
Medicare Coverage Criteria for Ankle Braces
Medicare is often the strictest payer. If you meet their criteria, you usually meet the criteria for private insurers. Here are the specific coverage rules for ankle braces:
-
Off-the-Shelf (OTS) Orthotics: For codes like L1902 or L1970, Medicare considers these “off-the-shelf.” Beneficiaries usually pay a 20% coinsurance after the Part B deductible. No KX modifier is required for OTS unless there is a specific local coverage determination (LCD) stating otherwise.
-
Custom Fabricated Orthotics: For codes like L1907 or L2108, Medicare requires:
-
A detailed written order prior to fabrication.
-
A face-to-face encounter within 6 months.
-
The KX modifier appended to the claim.
-
Specific documentation stating why a prefabricated device cannot be used (e.g., “Patient has foot deformity that cannot be accommodated by any prefabricated device available on the market”).
-
Important Note: Many local Medicare Administrative Contractors (MACs) have specific Local Coverage Determinations (LCDs) for “Ankle-Foot Orthosis.” It is crucial to check the LCD for your specific state (e.g., Noridian, Novitas, Palmetto GBA) as they may have unique frequency limits (e.g., one brace per lifetime unless there is a change in condition).
Tips to Avoid Denials
Denials in DME billing are frustrating, but they are often preventable. Here is a checklist to keep your claims clean:
-
Verify the “DMEPOS” Status: Is the patient on a Medicare Advantage plan? Does their insurance require the use of a specific contracted DME supplier? If you are a physician office dispensing braces, ensure you are enrolled as a Medicare DME supplier; otherwise, you cannot bill for the brace itself—only the fitting service.
-
Match the Code to the Brace: Do not get creative. If you dispensed a lace-up gauntlet, do not bill L1970 just because the reimbursement is higher. Insurers audit physical inventory.
-
Timely Documentation: Ensure the Detailed Written Order is signed and dated before or on the date the patient takes the brace home. A backdated order or an order dated after delivery is a guaranteed denial.
-
Use the Right Modifiers: Forgetting the RT (right) or LT (left) modifier is a top reason for automated denials. If the brace is for bilateral use, use U1 or the specific policy indicator, though ankle braces are rarely bilateral.
The Patient’s Perspective: Out-of-Pocket Costs
As a writer, it is important to address the human side of this. When patients hear about “codes,” they usually just want to know: “How much is this going to cost me?”
Even with the correct HCPCS code, costs vary wildly based on the patient’s insurance plan.
-
For Soft Braces (L1902): These are often purchased outright at a pharmacy or online for $20–$50. Billing insurance for these is often not worth the administrative cost, as they may be considered “non-covered” or applied to a high deductible.
-
For Rigid Walking Boots (L1970): The allowable rate by insurance can range from $80 to $200. The patient is responsible for their copay or coinsurance, which could be 20% of the allowed amount.
-
For Custom AFOs (L1907): These can be expensive, often costing $500 to $2,000. These almost always go through insurance, and patients with high deductibles may face significant out-of-pocket costs.
Future Trends in Ankle Brace Coding
Coding is not static. As of 2026, we are seeing a continued emphasis on medical necessity documentation and a crackdown on “overutilization” of walking boots (L1970) for minor sprains.
Additionally, there is a growing trend toward telehealth for orthotic management. While you cannot usually bill a fitting code (97760) via telehealth unless it is synchronous audio-video with specific criteria, the evaluation for necessity often happens virtually. This means the documentation requirements for the Detailed Written Order become even more critical, as the physical “hands-on” fitting is absent.
Conclusion
Finding the correct HCPCS code for an ankle brace is less about memorizing a single number and more about understanding the clinical picture. The “CPT code for ankle brace support” is usually a combination of a HCPCS device code (like L1902 for a soft gauntlet or L1970 for a walking boot) paired with a CPT service code (like 97760 for training) and supported by a robust ICD-10 diagnosis.
By focusing on documentation—specifically the Detailed Written Order, the medical necessity justification, and the appropriate modifiers—you can significantly reduce denials and ensure patients get the support they need without administrative headaches.
Frequently Asked Questions (FAQ)
Q1: Can I bill an office visit (E/M code) and a brace fitting on the same day?
A: Yes, you can bill an Evaluation and Management (E/M) code (e.g., 99213) alongside a brace fitting code (97760), but you must append modifier -25 to the E/M code to indicate it was a separately identifiable service. You cannot bill the E/M code if the only purpose of the visit was to dispense the brace.
Q2: What is the difference between L1902 and L1970?
A: L1902 is a “gauntlet”—a soft, lace-up brace that covers the ankle and foot but does not extend up the calf. It provides mild support. L1970 is a rigid or hinged plastic orthosis (often a walking boot) that extends up the calf and restricts ankle motion significantly. L1970 is for more severe injuries or post-operative use.
Q3: Do I need a prescription for an ankle brace to bill insurance?
A: Yes. For insurance to pay for an ankle brace, you must have a Detailed Written Order (DWO) from a treating practitioner. A verbal order is not sufficient for DME (Durable Medical Equipment) billing.
Q4: Why was my claim denied with code CO-50?
A: CO-50 (Contractual Obligation) often means that the procedure code is not covered based on the medical necessity criteria. This usually happens if the diagnosis code does not match the brace code (e.g., using L1970 for a simple strain when the insurer expects L1902).
Q5: Can I bill Medicare for an ankle brace I bought at a pharmacy?
A: If you are a Medicare beneficiary and you purchase a brace from a pharmacy without a physician’s order, Medicare will not cover it. If the brace is prescribed and supplied by a Medicare-enrolled DME provider, Medicare Part B may cover it, subject to the deductible and coinsurance.
Q6: Is a walking boot considered an AFO?
A: Yes. In coding terms, a walking boot falls under the category of an Ankle Foot Orthosis (AFO) . The specific code depends on whether it is prefabricated (L1970) or custom fabricated (L2108).
Additional Resource
For the most up-to-date information on Local Coverage Determinations (LCDs) for Ankle-Foot Orthoses, it is essential to check the official Medicare Coverage Database.
-
Resource: Medicare Coverage Database – Ankle Foot Orthosis (AFO) LCDs
-
Navigate to this link and search for “Ankle Foot Orthosis” or the specific HCPCS code (e.g., L1970) to find the coverage policies specific to your state or region.
-
Final Note on Compliance
Medical coding is a high-stakes field. While this guide provides a comprehensive overview, it is your responsibility to ensure that you are billing in accordance with the latest CMS guidelines, payer-specific policies, and state regulations. When in doubt, consult with a certified professional coder (CPC) or a compliance officer.





