If you work in urology medical coding, you know that the transurethral resection of the prostate (TURP) is one of the most common, yet surprisingly complex, procedures to bill. It’s not just one code. Depending on the technique, the patient’s history, and what the surgeon finds inside the operating room, the correct CPT code can shift dramatically.
Using the wrong code can mean the difference between a clean claim and a denial, or worse, a compliance audit.
In this guide, we’re going to strip away the confusion. We’ll look at the specific CPT codes associated with TURP, explore the nuances that determine which code to use, and discuss how to handle the modifiers and bundling rules that often trip up even seasoned billers.
CPT Codes for Transurethral Resection of the Prostate
Understanding the Basics: What is a TURP?
Before we dive into the numbers, let’s establish a baseline understanding of the procedure itself.
The prostate is a walnut-sized gland located just below the bladder in men. As men age, the prostate can enlarge—a condition known as benign prostatic hyperplasia (BPH). When this enlargement begins to squeeze the urethra, it causes urinary symptoms that range from annoying to debilitating.
A transurethral resection of the prostate is the surgical “gold standard” for treating moderate to severe BPH. The surgeon inserts a resectoscope through the urethra (hence “transurethral”) to reach the prostate. Using a wire loop, they shave away excess prostate tissue that is blocking the flow of urine.
Because this is a resection, meaning tissue is removed, the coding is significantly different from procedures that simply destroy tissue (like laser vaporization) or alter the anatomy.
The Primary CPT Code: 52601
When most medical professionals ask for the cpt code for transurethral resection of prostate, they are usually referring to the standard, most common procedure.
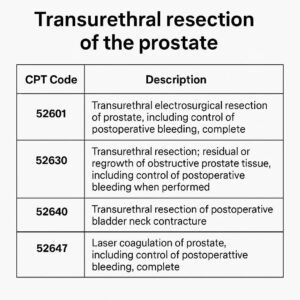
CPT 52601: Transurethral electrosurgical resection of prostate, including control of postoperative bleeding, complete (vasectomy, meatotomy, cystourethroscopy, urethral calibration and/or dilation, and internal urethrotomy are included)
What Does 52601 Include?
This code is incredibly comprehensive. When you bill 52601, you are telling the payer that the surgeon performed a complete resection of the prostate using an electrosurgical loop.
It is crucial to understand that this code has a list of included services. You cannot bill separately for these components just because they are documented in the operative report.
-
Cystourethroscopy: The visualization of the urethra and bladder is inherent to the procedure. Do not add a separate cystoscopy code (like 52000).
-
Urethral Calibration and/or Dilation: If the surgeon needs to dilate the urethra to pass the scope, this is bundled.
-
Internal Urethrotomy: Cutting of a stricture is included.
-
Meatotomy: Incision of the urinary meatus is included.
-
Vasectomy: If performed during the same session, it is considered incidental and bundled.
-
Control of Postoperative Bleeding: The “including control of postoperative bleeding” clause is important. This means the primary surgery covers the work of achieving hemostasis at the time of surgery. However, if the patient returns to the OR days later specifically for bleeding, that is a separate scenario (which we will discuss later).
When Is 52601 the Wrong Choice?
You cannot use 52601 if the surgeon only performed a partial resection. The descriptor says “complete.” If the documentation states “a limited resection” or “a small chip” was taken for pathology, you are likely looking at a different code or a biopsy code.
Alternative TURP Codes and Laser Procedures
Modern urology offers many ways to treat BPH. The rise of laser therapies has created a separate family of CPT codes that are often confused with the traditional TURP.
Here is a breakdown of the most common alternatives.
CPT 52648: Laser Vaporization
This is one of the most common competitors to the traditional TURP.
CPT 52648: Laser vaporization of prostate, including control of postoperative bleeding, complete (vasectomy, meatotomy, cystourethroscopy, urethral calibration and/or dilation, and internal urethrotomy are included)
If the surgeon uses a laser (such as GreenLight, Holmium, or Thulium) to vaporize the tissue rather than physically resecting it with a wire loop, this is the code to use.
Key Difference: 52648 is for vaporization. No tissue is sent to pathology (or if it is, it is minimal). 52601 is for resection, where physical chips of tissue are removed and sent to pathology for analysis.
CPT 52630: Secondary TURP
Patients sometimes need a second procedure years after the first if the prostate continues to grow or if symptoms return.
CPT 52630: Transurethral resection of prostate; secondary, for regrowth or residual tissue
This code is used exclusively for a repeat TURP. It is not for the initial surgery. It acknowledges that the procedure is being done in a previously operated field, which carries different surgical complexity.
Important Note: Do not use this if the patient had a previous laser vaporization and is now having a resection. The “secondary” typically refers to a subsequent resection after a previous resection.
CPT 52647 and 52649: Laser Coagulation
These codes are less common today but still appear in payer policies.
-
52647: Laser coagulation of prostate (e.g., TULIP).
-
52649: Laser enucleation of the prostate (e.g., HoLEP) with morcellation.
HoLEP (Holmium Laser Enucleation of the Prostate) is an important distinction. While 52648 is for vaporization, HoLEP (often coded with 52649) involves enucleating (shelling out) the adenoma and then morcellating (chopping) it up for removal. This is a more complex procedure and is reimbursed differently than standard vaporization.
The Critical Role of Modifiers
Choosing the right CPT code is only half the battle. In urology, modifiers often determine whether you get paid or not, especially when dealing with bilateral structures or multiple procedures.
Modifier -50: Bilateral Procedure
Technically, the prostate is a single midline structure. However, some payers require modifier -50 if the procedure addresses both lobes in a way that qualifies as bilateral. Typically, for TURP, you do not append modifier -50. However, if you are coding a CPT code for transurethral resection of prostate along with a bilateral vasectomy or other urological procedure, modifiers become essential.
Modifier -51: Multiple Procedures
This is the most common modifier used with TURP codes. If the surgeon performs a TURP and a separate, distinct procedure that is not bundled, you append modifier -51 to the secondary procedures.
Example: A patient undergoes a TURP (52601) and a cystolitholapaxy (52317) to remove a bladder stone. The stone removal is a separate, significant procedure. You would bill 52601 as the primary procedure and 52317-51 as the secondary.
Modifier -22: Increased Procedural Services
If the TURP is unusually complex due to factors like an extremely large prostate (over 100 grams), significant scarring from prior surgery, or unusual anatomical anomalies, you may append modifier -22.
This modifier tells the payer: This was more work than a standard case. You must include a detailed operative report and a cover letter explaining why the complexity was exceptional. Without supporting documentation, this modifier will likely result in a denial.
Bundling Issues: What Not to Bill
One of the biggest pitfalls in urology coding is unbundling. The American Medical Association (AMA) and the National Correct Coding Initiative (NCCI) have strict rules about what services are considered integral to a TURP.
Do Not Bill These Separately
When you submit a claim for 52601 or 52648, you cannot bill for these separately:
| Procedure | Rationale |
|---|---|
| Cystourethroscopy (52000) | It is a component part of the TURP. You cannot see the prostate without a scope. |
| Urethral Dilation (53600-53665) | This is explicitly listed in the code descriptor as included. |
| Biopsy of Prostate (55700) | The resection removes tissue. If the surgeon is doing a resection, a separate biopsy is not warranted. |
| Control of Bleeding | This is included unless the patient returns to the OR days later. |
| Simple Cystoscopy | Again, integral. |
When You Can Bill Separately
There are scenarios where additional codes are appropriate, provided they are clearly documented.
-
Complex Urodynamics (CPT 51784, 51785): If performed as a separate, billable service prior to the surgery on a different date.
-
Ultrasound Guidance (CPT 76942, 76998): If the surgeon uses ultrasound guidance for the resection (often done for large prostates or suspected cancer), this may be billable. However, check payer policies. Medicare often considers it bundled.
-
Transurethral Ultrasound (CPT 76872): This is a diagnostic procedure. If performed immediately before the TURP for diagnostic planning, it is typically bundled. If performed on a separate day, it is billable.
Coding for Post-Operative Complications
A TURP is a safe procedure, but complications do happen. How you code these complications depends entirely on the timing and the “global surgical package.”
Most TURPs come with a 90-day global period. This means that for 90 days after the surgery, any related care is considered part of the original reimbursement.
Bleeding
If a patient returns to the operating room within the global period for control of bleeding, you cannot bill a new TURP code.
Instead, you use:
CPT 52620: Transurethral resection; of postoperative bladder neck contracture
Wait, isn’t that for contracture?
Actually, for bleeding, the standard approach is to use CPT 52620 if the procedure involves resection of the clot or fulguration of bleeding vessels, or CPT 52450 (Transurethral incision of prostate) depending on the payer and the method used to stop the bleeding. Many coders rely on CPT 52001 (Cystourethroscopy with irrigation and evacuation of clot) for managing clot retention in the global period.
Important: You must use modifier -78 (Unplanned return to the operating/procedure room by the same physician following initial procedure for a related procedure during the postoperative period). This modifier ensures the payer understands this is a complication, not a new, unrelated surgery.
Bladder Neck Contracture (BNC)
Months or years after a TURP, a patient may develop scar tissue at the bladder neck.
For this, you use:
CPT 52620: Transurethral resection; of postoperative bladder neck contracture
This code is specifically for the resection of scar tissue that formed after a prior prostate surgery. It is a distinct procedure from the initial TURP.
Comparative Analysis: TURP vs. Other BPH Procedures
To help visualize the differences, here is a comparative table of the most common BPH procedure codes.
| CPT Code | Procedure Name | Technique | Tissue Sample | Key Indicator |
|---|---|---|---|---|
| 52601 | TURP (Electrosurgical) | Wire loop resection | Yes (Chips) | Gold standard; tissue for pathology |
| 52648 | Laser Vaporization | Laser energy | No | Minimally invasive; for patients on blood thinners often |
| 52649 | Laser Enucleation (HoLEP) | Laser enucleation + morcellation | Yes (Morcellated) | Large prostates (>100g) |
| 52630 | Secondary TURP | Wire loop resection | Yes | Prior history of TURP |
| 52620 | Resection of BNC | Resection of scar tissue | Variable | Post-operative complication |
| 52441 | UroLift (each additional) | Implant | No | Outpatient; preserves ejaculation |
Documentation Requirements for Coders
As a medical coder, you are only as good as the documentation you receive. To accurately assign a cpt code for transurethral resection of prostate, the operative report must contain specific elements.
The “Must-Haves” in the Operative Report
-
Approach: The report must clearly state “transurethral.”
-
Method: Does it say “resection with wire loop” (52601) or “laser vaporization” (52648)?
-
Specimen: If the path report shows “prostatic chips,” it supports 52601. If there is no specimen (or only vaporized debris), it supports 52648.
-
Completeness: The surgeon must state whether the resection was “complete” or “limited.” If they only took a biopsy, use biopsy codes (55700 series), not resection codes.
-
Size: While not always required for coding, documenting the prostate size (e.g., “estimated 40g”) supports medical necessity, especially for laser procedures where size limits may apply.
Reimbursement and Payer Policies
Reimbursement for TURP has changed over the years. Medicare and commercial payers have shifted toward value-based care, but the facility (hospital) and professional (surgeon) components are billed separately.
Professional Component (PC) vs. Facility
-
Professional Component (Modifier -26): This covers the surgeon’s work. In an outpatient setting (ASC or hospital outpatient), you will bill the TURP code with modifier -26.
-
Facility Component (Modifier -TC): This covers the operating room, equipment, and staff. This is billed by the facility.
-
Global: If performed in an office-based surgery suite (less common for TURP due to equipment costs), you may bill the code globally without a modifier.
Medicare’s Perspective
Medicare considers TURP a highly scrutinized procedure. Medical necessity is key. The documentation must show:
-
Failed conservative management (medication).
-
Objective evidence of obstruction (urinary flow rates, post-void residual).
-
Moderate to severe symptom score (AUA symptom score).
If the documentation for 52601 shows a prostate estimated at 20 grams (small), Medicare may deny the claim, arguing that a less invasive procedure (like TURP of the prostate with a different method) should have been attempted first.
Common Denials and How to Avoid Them
Even with perfect coding, denials happen. Here are the top reasons TURP claims are denied.
1. Unbundling
Error: Billing 52000 (cystoscopy) with 52601.
Solution: Educate your providers that the cystoscopy is inclusive. Audit your claims to ensure software edits are not automatically appending the cystoscopy code.
2. Missing Diagnosis Codes
The diagnosis must support the surgical code.
-
For 52601: Use N40.1 (Enlarged prostate with lower urinary tract symptoms) or N40.0 (Enlarged prostate without lower urinary tract symptoms) depending on the clinical picture.
-
Do not use R35.0 (Frequency of urination) alone. You need the structural diagnosis (N40.x).
3. Incorrect Modifier Usage
Error: Using modifier -51 on the primary procedure.
Solution: In most payer hierarchies (including Medicare), the highest-valued procedure is listed first without modifier -51. The subsequent procedures get -51.
4. Global Period Misunderstanding
Error: Billing an office visit (E/M code) with a modifier -25 during the global period for a post-op complication.
Solution: If the patient comes in 2 weeks post-TURP with a UTI, you can bill the E/M code with modifier -25 if the UTI is a separate, distinct issue from the surgery. If they come in for post-op bleeding, it is included.
Tips for Surgical Schedulers and Billers
To ensure a smooth revenue cycle, the conversation about coding needs to start before the patient ever enters the operating room.
-
Verify Benefits: Check if the patient has a high deductible. TURPs are costly. Ensure the pre-authorization is obtained with the correct CPT code. If the surgeon plans a 52601 but the authorization is for a 52648, you will face a denial.
-
Pre-Authorization: For commercial payers, you often need to provide clinical notes proving the prostate size and failed medical management. Submit the AUA symptom score sheet if possible.
-
Post-Op Checklist: Create a checklist for your providers that highlights the key elements needed for coding: Approach, Method, Specimen, Size, and Complexity.
The Future of TURP Coding
The landscape of urology coding is dynamic. While the traditional TURP (52601) remains a stalwart in the CPT code set, we are seeing a shift.
Newer procedures like Aquablation (which uses a water jet to resect tissue) currently lack a unique CPT code. Currently, Aquablation is often coded with the unlisted code 53899 (Unlisted procedure, urinary system), which requires submitting a paper claim with the operative report and a cost comparison. This is a high-risk area for denials and requires meticulous documentation.
Similarly, the Rezūm system (water vapor therapy) is typically billed under 53899 as well. As these technologies mature, we may see dedicated CPT codes emerge, but for now, unlisted codes remain the norm for non-laser, non-resection technologies.
Quotation from a Coding Expert
“The biggest mistake I see in urology practices is assuming that because a scope went in and the prostate was treated, it automatically defaults to 52601. You have to read the operative note. Did they use a loop or a laser? Did they take tissue or vaporize it? If you miss that distinction, you’re not just losing revenue; you’re potentially committing fraud by upcoding a vaporization to a resection.”
— Janet R., CPC, COC, Senior Urology Coding Consultant
Important Notes for Readers
Note 1: Payer-Specific Variations
While this guide covers the standard CPT guidelines, every insurance carrier—including Medicare, Medicaid, and commercial plans like UnitedHealthcare or Cigna—has unique medical policies. Some carriers consider 52648 (laser vaporization) the preferred method and will deny 52601 unless a specific medical reason (like need for pathology) is documented. Always check the Local Coverage Determination (LCD) for your jurisdiction.
Note 2: The 2026 Updates
As of March 2026, there have been no major structural changes to the TURP family of codes compared to 2025. However, the Relative Value Units (RVUs) are updated annually. Always ensure your billing software is using the most current fee schedule to avoid reimbursement discrepancies.
Note 3: Assistant Surgeons
In rare cases involving massive prostates or high-risk patients, an assistant surgeon may be required. If an assistant is used, you would append modifier -80 (Assistant surgeon) to the primary CPT code. However, payers are increasingly strict about assistant-at-surgery claims for TURP, often denying them unless the medical necessity is clearly documented.
Note 4: Coding for Females
While a “prostate” is specific to male anatomy, if you are coding for a transgender patient (male-to-female) who has had a prostate and is undergoing a related procedure, the same CPT codes apply. However, you must ensure the ICD-10 diagnosis code reflects the patient’s anatomy and the medical necessity for the procedure.
Conclusion
Navigating the cpt code for transurethral resection of prostate requires more than just memorizing a number. It demands a thorough understanding of surgical techniques, documentation requirements, and payer-specific bundling rules. By distinguishing between resection (52601) and vaporization (52648), respecting the global surgical package, and using modifiers appropriately, you can ensure compliant billing and maximize reimbursement for your urology practice.
Frequently Asked Questions (FAQ)
Q1: What is the most common CPT code for a standard TURP?
The most common code is 52601 (Transurethral electrosurgical resection of prostate, complete). This is used when the surgeon uses a wire loop to physically cut and remove prostate tissue for pathology.
Q2: Can I bill a cystoscopy (52000) separately with a TURP?
No. Cystourethroscopy is considered an integral component of a TURP. The NCCI edits bundle 52000 into 52601, 52630, and 52648.
Q3: What is the difference between 52601 and 52648?
52601 is for electrosurgical resection using a wire loop, which yields tissue chips for pathology. 52648 is for laser vaporization, which destroys the tissue without a physical specimen for pathology.
Q4: How do I code a TURP for a patient who had a previous prostate surgery?
You should use CPT 52630 (Secondary TURP for regrowth or residual tissue). This acknowledges the increased complexity of operating in a previously resected field.
Q5: How do I code an emergency return to the OR for bleeding after a TURP?
You should code the procedure performed to stop the bleeding (e.g., 52001 for clot evacuation or 52620 for fulguration of bleeding) and append modifier -78 (Unplanned return to the OR for a related procedure).
Final Checklist for Coders
Before submitting your claim for a TURP, run through this quick checklist:
-
Did I verify the surgical method (Resection vs. Laser vs. Enucleation)?
-
Did I avoid unbundling cystoscopy or dilation?
-
Did I use the appropriate modifier (-78, -51) if applicable?
-
Is the diagnosis code specific (N40.1) and does it support medical necessity?
-
Did I check the payer’s LCD for frequency limitations or size requirements?
-
Is the patient still within the global period for a prior procedure?
By maintaining vigilance on these details, you ensure that your practice remains compliant, profitable, and focused on delivering excellent patient care.





