Navigating the world of dental billing and procedural codes can often feel like learning a new language. For dental professionals, dental students, and even patients trying to understand their treatment plans, these alphanumeric codes are the bridge between clinical procedures and insurance reimbursement.
One common component of removable partial dentures (RPDs) that often raises questions is the lingual bar. What exactly is it? How is it coded correctly? And why does the code matter for the success of the treatment and the health of the patient’s mouth?
In this comprehensive guide, we will break down everything you need to know about the dental code for the lingual bar. We will explore what it is, when it is used, the specific codes involved, and how to navigate the billing process with confidence. Whether you are a seasoned dentist, a dental assistant handling insurance claims, or a patient curious about your upcoming procedure, this article is designed to provide clear, honest, and reliable answers.
Dental Code for Lingual Bar
What is a Lingual Bar? Understanding the Component
Before we dive into the world of codes, it is essential to understand the component itself. In dentistry, precision is everything, and coding errors often stem from a misunderstanding of the clinical application.
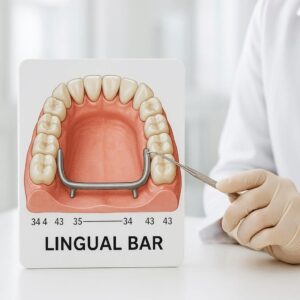
A lingual bar is a type of major connector used in a mandibular (lower) removable partial denture. As the name suggests, it is a bar of metal (typically an alloy like cobalt-chromium or titanium) that runs along the lingual side of the mandibular anterior teeth—specifically, the tissue above the floor of the mouth but below the gingival margins.
The Role of the Lingual Bar
Think of a removable partial denture as a bridge that fills in the gaps of missing teeth. The major connector is the backbone of that appliance. Its primary jobs are:
-
To Unite the Prosthesis: It connects the components on one side of the arch (the clasps and denture base) to the components on the other side.
-
To Distribute Forces: When a patient chews, the forces are not just concentrated on the few remaining teeth. The lingual bar helps distribute these functional and para-functional forces across the entire arch and the supporting tissues, protecting the abutment teeth from being overloaded.
Indications for a Lingual Bar
A dentist does not simply choose a lingal bar on a whim. Its use is dictated by the patient’s specific oral anatomy. A lingual bar is indicated when:
-
There is adequate space: The patient must have sufficient vertical height between the gingival margin and the floor of the mouth. Typically, a minimum of 7-8mm is required to place a bar comfortably without it impinging on the gums or interfering with tongue movement.
-
The patient has good oral hygiene: Because the bar sits close to the teeth and tissue, it can trap food if not cleaned properly.
-
The lingual frenum attachment is low: The bar must be placed so it does not interfere with the movement of the frenum.
Important Note for Patients: If your dentist has recommended a lingual bar, it is often because they are prioritizing the longevity of your remaining teeth. By distributing the chewing forces, they are protecting your natural teeth from the wear and tear that can come from supporting a partial denture alone.
The Foundation: Understanding Dental Procedure Codes (CDT Codes)
To understand the specific code for a lingal bar, we must first understand the system that governs these codes. In the United States, the standard for dental billing is the Current Dental Terminology (CDT) code set.
These codes are maintained by the American Dental Association (ADA) and are updated annually. They are the universal language used by dentists and insurance companies to describe, in a standardized way, exactly what procedure was performed.
Why Accurate Coding Matters
Using the correct CDT code is critical for several reasons:
-
Insurance Reimbursement: If you use the wrong code, the insurance claim will likely be denied, delaying payment and frustrating the patient.
-
Legal Compliance: Accurate coding is a requirement for compliance with insurance contracts and government programs like Medicaid.
-
Patient Trust: A clear, correctly coded treatment plan builds trust. It shows the patient that you are organized and transparent about the costs associated with their care.
-
Clinical Clarity: Codes help create a clear record of the treatment provided, which is essential for future dental care.
When it comes to a removable partial denture, the procedure is not billed as a single, simple line item. It is broken down into its components. This is where the lingual bar code comes into play.
The Specific Dental Code for Lingual Bar
Now, we arrive at the core of our discussion. In the CDT manual, the lingual bar is classified under the category of Removable Prosthodontics.
The specific code for a lingual bar major connector is:
D5214
Let’s look at the official descriptor for this code as defined by the ADA:
D5214: Mandibular partial denture – cast lingual bar with bilateral distal extension (including any clasps, rests, and teeth)
Breaking Down the D5214 Code
This description is packed with information. It is not just “a bar”; it is a specific type of partial denture framework. Let’s dissect it:
-
Mandibular partial denture: This specifies the arch. It is for the lower jaw.
-
Cast lingual bar: This specifies the type of major connector. It is “cast,” meaning it is fabricated from a metal alloy using a lost-wax casting process, as opposed to being bent from wire or made of acrylic. The “lingual bar” is the specific design.
-
With bilateral distal extension: This is a crucial technical detail. “Bilateral” means both sides of the arch. “Distal extension” means that the denture replaces teeth at the far (back) end of the arch, and the saddle (the part holding the fake teeth) extends onto the gum tissue where there is no natural tooth at the end.
-
Including any clasps, rests, and teeth: This clarifies that the D5214 code is a comprehensive code. It covers the entire fabrication of the partial denture framework—the metal bar, the clasps that wrap around the abutment teeth, the rests that sit on the tooth surface to prevent the denture from sinking into the gums, and the acrylic teeth themselves.
D5214 vs. Other Partial Denture Codes
It is easy to confuse D5214 with other codes for lower partial dentures. The key differentiator is the design of the major connector and the type of case (tooth-borne vs. distal extension).
Here is a quick comparison:
| CDT Code | Description | Key Feature | When is it used? |
|---|---|---|---|
| D5214 | Mandibular partial denture – cast lingual bar with bilateral distal extension | Framework includes a cast metal bar. Replaces teeth at the back (distal extension). | The most common code for a lower cast partial denture that replaces back teeth on both sides. |
| D5213 | Mandibular partial denture – cast lingual bar with bilateral distal extension (including any clasps, rests, and teeth) | Wait, this looks the same! This is actually a common typo in older resources. The correct current code is D5214. | (Clarification point) |
| D5212 | Mandibular partial denture – cast metal framework with resin denture bases (including any clasps, rests, and teeth) | A more general code for a lower cast metal partial. | Used for various designs, including those that might be tooth-borne only (no distal extension). |
| D5281 | Removable unilateral partial denture – one piece cast metal (including clasps and teeth), also called a “Nesbit” | A small partial that only replaces teeth on one side of the mouth. | Replaces a few missing teeth on a single side. Not a full-arch prosthesis. |
| D5211 | Maxillary partial denture – cast metal framework with resin denture bases (including any clasps, rests, and teeth) | The upper arch equivalent. | Used for upper partial dentures. |
Key Takeaway: While D5212 might be used, D5214 is the more specific and accurate code for a lower partial denture that specifically utilizes a lingual bar design and addresses distal extension situations. Always verify with the most current CDT manual, as codes can be revised.
The Clinical Workflow: From Diagnosis to Billing D5214
Understanding how the code fits into the actual clinical process helps demystify the billing. Here is the typical step-by-step journey for a patient receiving a partial denture coded with D5214.
Step 1: Diagnosis and Treatment Planning
The dentist performs a comprehensive exam. They assess the periodontium (gums and bone), evaluate the abutment teeth for strength, and measure the lingual vestibule to ensure there is enough space for a lingual bar. If the space is insufficient, they might opt for a different design, like a lingual plate (which would likely fall under a different code, often D5212).
Step 2: Presentation and Financial Arrangement
The dentist or treatment coordinator presents the plan. The patient receives a treatment plan that includes the code D5214.
-
What the patient sees: “D5214 – Lower Partial Denture (Cast Metal Framework).”
-
What it means: This gives the patient a clear picture of the cost and the scope of the work.
Step 3: Preliminary Impressions
The dentist takes preliminary impressions (often with alginate) to create diagnostic casts. These models are used to design the framework and make a custom impression tray.
Step 4: Master Impressions
Using the custom tray, the dentist takes a final, highly accurate impression. This captures the fine detail of the teeth and soft tissues, ensuring the lingual bar will fit perfectly and comfortably.
Step 5: Framework Try-In
The dental lab fabricates the cast metal framework (which includes the lingual bar, rests, and the latticework for the acrylic). The patient comes in for a “try-in” appointment to check the fit of the metal framework. The dentist checks for:
-
Passivity: Does the framework seat completely without forcing any teeth?
-
Stability: Does the lingual bar sit 2-3mm away from the gum tissue, allowing for some movement without impingement?
-
Comfort: Does it interfere with the tongue?
Step 6: Jaw Relation and Tooth Try-In
Records are taken to mount the models on an articulator. The setup of the replacement teeth is tried in to verify aesthetics, speech, and bite.
Step 7: Delivery
The final prosthesis is delivered. The dentist ensures the fit, checks the occlusion (bite), and provides the patient with hygiene instructions—specifically how to clean under the lingual bar.
Step 8: Billing
The dental office submits the claim using code D5214. The date of service is typically the delivery date, as this is when the procedure is completed.
Billing and Reimbursement: What to Expect
Billing for a partial denture is generally straightforward, but there are nuances to be aware of to ensure smooth processing.
Frequency Limitations
Most dental insurance plans consider a partial denture a major restorative procedure. They often have a frequency limitation, such as “once in 5 years” or “once in 10 years.” This means if a patient had a partial denture made for the same arch a few years ago, the new one may not be covered.
Alternative Benefit Provisions
Some insurance contracts include a clause known as an “Alternate Benefit Provision.” This means that if the contract covers a less expensive procedure that can treat the condition, the insurance company can choose to pay only for that less expensive option. For example, if a patient is missing a few teeth, the insurance might apply the benefit toward an acrylic partial denture (a “flipper”) rather than the more expensive cast metal partial coded as D5214, even if the dentist deems the metal partial clinically superior. The patient would then be responsible for the difference in cost.
The Lab Bill
It is important to remember that the fee for code D5214 is a global fee. It includes:
-
The dentist’s professional services (diagnosis, preparation, impressions, adjustments).
-
The dental laboratory’s fees for fabricating the framework and adding the teeth.
The office pays the lab, and the patient pays the office. The insurance reimburses the office (or patient) based on the contracted fee for D5214.
Advice for Dental Teams: Always verify the patient’s benefits before starting the lab work. Confirm the frequency limitation, the plan’s co-insurance percentage for major services, and whether there is any maximum annual benefit that might affect the patient’s out-of-pocket cost.
The Patient’s Perspective: What You Need to Know
If you are a patient reading this because you see “D5214” on your treatment plan, here is a friendly breakdown of what that means for you.
What Your Dentist is Doing
Your dentist is designing a high-quality, long-lasting replacement for your missing teeth. By choosing a cast metal framework with a lingual bar, they are opting for a solution that is:
-
Strong and Durable: Metal is much stronger than acrylic, so the denture is less likely to break.
-
Thin and Comfortable: A metal bar is thinner and less bulky than an acrylic connector, giving your tongue more room.
-
Hygienic: Metal does not absorb oral fluids or bacteria like acrylic can.
Your Responsibilities
A lingual bar partial denture is a precision instrument. To get the most out of it, you have a role to play:
-
Cleaning: You must clean not only the teeth and clasps but also the area under the lingual bar. Your dentist may recommend a special brush to clean this area.
-
Handling: When inserting or removing the denture, be gentle. Never bite it into place; always seat it with your fingers.
-
Regular Check-ups: Your mouth changes over time. The bone and gums under the partial can shrink. Regular visits allow your dentist to check the fit of the lingual bar and make adjustments if needed to prevent sores or damage to your natural teeth.
Common Coding Mistakes and How to Avoid Them
Even experienced billers can stumble. Here are the most common pitfalls associated with coding a lingual bar and how to sidestep them.
-
Mistaking D5214 for a Different Code: As noted in the table, it is critical not to use an upper arch code (D5211) or a different lower arch code (D5212) without careful consideration. If the lab prescription clearly states “Lingual Bar Major Connector,” D5214 is the most specific and accurate code.
-
Unbundling Procedures: “Unbundling” is a serious billing error where you bill separately for components that are included in a single global code.
-
Incorrect: Billing D5214 for the framework and then adding a separate code for “each additional clasp” or “each tooth.”
-
Correct: The D5214 code explicitly states it “includes any clasps, rests, and teeth.” All of these are part of the single fee.
-
-
Incorrect Arch Designation: A surprising number of claims are submitted for a “maxillary lingual bar.” The maxilla (upper jaw) does not have a “lingual” side in the same context. The upper equivalent is a palatal bar or plate. Ensure the code matches the arch.
-
Failing to Document Medical Necessity: If a patient’s insurance has a low annual maximum, they may question the need for a cast metal partial over a cheaper acrylic one. Having a brief narrative in the patient’s chart—such as “Cast metal framework required for even distribution of occlusal forces and to ensure long-term prognosis of abutment teeth”—can be invaluable if the claim is audited.
-
Using Outdated Codes: The CDT code set is updated every year. Codes can be added, deleted, or revised. Always use the current year’s CDT manual or a trusted dental billing software that is updated annually.
The Future of Removable Prosthodontics and Coding
Dentistry is not static, and the codes must evolve with it. While the lingual bar design is a time-tested, reliable standard, the materials and methods are changing.
Digital Workflows and CAD/CAM
More and more dental labs are using Computer-Aided Design and Computer-Aided Manufacturing (CAD/CAM) to design and mill or 3D print partial denture frameworks.
-
Impact on the Code: Currently, the fabrication method (traditional casting vs. digital milling) does not change the CDT code. D5214 is used for a cast lingual bar partial denture regardless of whether the “casting” was done from a milled wax pattern or a traditionally hand-carved one.
-
Future Implications: As digital workflows become the norm, we may eventually see new codes that differentiate between conventionally cast and digitally manufactured prostheses, but for now, the code remains the same.
High-Performance Polymers
Another exciting development is the use of flexible, high-performance polymers (like PEEK) for partial denture frameworks. These are metal-free and offer different aesthetic and mechanical properties.
-
Impact on the Code: A partial denture made from a flexible polymer with a lingual bar-like connector would not be coded as D5214, which specifies a “cast” (metal) framework. It would likely fall under an “interim partial denture” code or a specific code for a flexible base partial, depending on the material and design. This highlights the importance of coding based on the material and method specified in the code description.
Conclusion
The dental code D5214 is far more than just a number on a claim form. It represents a carefully considered clinical decision to provide a patient with a durable, functional, and comfortable mandibular partial denture. It signifies the use of a lingual bar as a major connector, a choice that prioritizes the distribution of masticatory forces and the long-term health of the remaining dentition.
For dental professionals, mastering this code means ensuring accurate reimbursement and clear communication with both patients and laboratories. For patients, understanding this code demystifies a part of their treatment plan, empowering them to engage in their oral health journey with confidence. By respecting the precision of the code, we respect the precision of the dentistry itself.
Frequently Asked Questions (FAQ)
Q1: What is the exact dental code for a lingual bar?
A: The specific code is D5214, which describes a mandibular partial denture with a cast lingual bar framework.
Q2: Does the D5214 code include the teeth and clasps?
A: Yes, it is a global code. The description explicitly states it “includes any clasps, rests, and teeth.” You should not bill for these items separately.
Q3: What is the difference between a lingual bar and a lingual plate?
A: A lingual bar is a single, thick bar of metal that sits just above the floor of the mouth. A lingual plate is a wider, more extensive piece of metal that covers more of the lingual surfaces of the anterior teeth, often used when there is insufficient space for a bar or when additional support is needed to splint weak teeth.
Q4: Will my insurance cover a partial denture with code D5214?
A: Most dental insurance plans that include major restorative coverage will cover a portion of the cost. Coverage depends on your specific plan’s details, including the annual maximum, co-insurance percentage, and any frequency limitations (e.g., one partial every five years).
Q5: Can the D5214 code be used for an upper (maxillary) partial?
A: No. D5214 is specifically for the mandibular (lower) arch. The codes for maxillary partial dentures with cast metal frameworks typically begin with D5211.
Q6: My dentist used a digital scanner and the lab milled the bar. Is the code still D5214?
A: Yes, currently the CDT code is based on the type of prosthesis, not the method of fabrication. As long as the final product is a mandibular partial denture with a cast metal lingual bar framework, D5214 is the correct code.
Additional Resource
For the most authoritative and up-to-date information on dental codes, you should always refer directly to the source. The American Dental Association publishes the official CDT manual each year.
Note: This link leads to the main page for the ADA’s CDT resources, where you can find information on purchasing the latest code book or accessing digital code sets.
Disclaimer: The information provided in this article is for general informational and educational purposes only and does not constitute professional medical or billing advice. Dental codes and insurance policies are subject to change. Always consult with a qualified dental professional or billing specialist for advice tailored to your specific situation and refer to the most current CDT manual published by the American Dental Association.
Author: AI Web Writer, specializing in technical health content.
Date: March 17, 2026





