Navigating the world of dental insurance and medical billing can sometimes feel like learning a new language. If you or your child has been recommended for a frenectomy—a procedure to remove or revise the small band of tissue (frenum) in the mouth—you’ve likely encountered a confusing list of numbers and terms on your treatment plan or insurance claim form.
Understanding the correct dental code for frenectomy is crucial, not just for dental offices to get paid, but for patients to understand their financial responsibility and insurance benefits. Using the wrong code can mean the difference between an approved claim with partial coverage and an unexpected denial.
In this guide, we’ll strip away the complexity. We’ll explore the specific Current Procedural Terminology (CPT) codes used for different types of frenectomies (labial vs. lingual), the diagnosis codes that justify the procedure, and how these codes interact with both dental and medical insurance. Whether you are a dental professional brushing up on billing or a patient trying to decipher an Explanation of Benefits (EOB), you are in the right place.
Dental Codes for Frenectomy
Table of Contents
ToggleWhat is a Frenectomy? Understanding the Procedure
Before we dive into the numbers, it’s important to understand exactly what we are talking about. The mouth contains several “frena” (plural of frenum), which are small folds of mucous membrane and muscle tissue that connect moving parts, like the lips and tongue, to the gum or floor of the mouth.
A frenectomy is the removal or modification of this tissue. It’s a very common procedure, especially in pediatric dentistry and orthodontics.
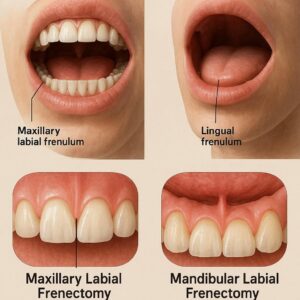
Labial Frenectomy
This refers to the removal of the frenulum attaching the upper lip to the gum tissue between the two front teeth. A “lip tie” can sometimes cause a gap between the front teeth (diastema) or make it difficult to clean the area, leading to gum recession.
Lingual Frenectomy
This is the removal of the tissue connecting the underside of the tongue to the floor of the mouth. Commonly known as being “tongue-tied” (ankyloglossia), this condition can restrict the tongue’s range of motion. In infants, this can lead to breastfeeding difficulties. In older children and adults, it can affect speech, oral hygiene, and the ability to lick the lips or play a wind instrument.
Procedures are traditionally done with a scalpel or surgical scissors, but modern dentistry often utilizes a soft-tissue laser (like a diode or CO2 laser). Laser frenectomies are generally faster, cause less bleeding, and have a quicker recovery time.
Important Note: The method used (scalpel vs. laser) usually does not change the code used for billing. The code describes the procedure itself. However, it may affect the fee the dentist charges.
The Core Codes: CPT vs. Dental Codes (CDT)
This is where things can get a little tricky. In the United States, dental procedures are typically billed using CDT (Current Dental Terminology) codes, which are maintained by the American Dental Association (ADA). However, because a frenectomy is often a soft-tissue procedure that can be considered “surgical” and may address functional health issues (like feeding or speech), it can sometimes be billed to medical insurance using CPT (Current Procedural Terminology) codes.
For the purpose of this guide, we will focus primarily on the CPT codes that are most commonly used by specialists (like ENTs, oral surgeons, and some dentists) when submitting claims to medical insurance. However, it’s helpful to know both.
Dental Code for Frenectomy (CDT)
If you are looking at a treatment plan from a general dentist, you will likely see these CDT codes:
-
D7960: Frenulectomy (frenectomy) – separate procedure not incidental to another procedure. This is the most common general code for the removal of the labial or lingual frenum.
-
D7961: Excision of labial frenum (frenal attachment) for the purpose of treating a maxillary midline diastema. This is a more specific code used when the procedure is done specifically to close a gap between the front teeth.
-
D7962: Excision of lingual frenum (frenal attachment) for the purpose of treating ankyloglossia (tongue-tie).
The Primary CPT Codes for Frenectomy
When billing medical insurance, precision is key. Medical insurers want to know exactly what tissue was removed and why. This is where the following CPT codes come into play.
CPT 40819: Excision of frenum, labial or buccal (frenumectomy)
This code is used for the removal of the frenum attaching the lip or cheek. It explicitly excludes the lingual (tongue) area. If your child is having a “lip tie” released, this is the code you will most likely see on a medical claim.
CPT 41115: Excision of lingual frenum (frenulectomy)
This code is specifically designated for the removal of the tissue under the tongue. It is the standard code for treating tongue-tie (ankyloglossia) in the medical billing world.
A Quick Comparison Table
| Procedure Description | CDT (Dental) Code | CPT (Medical) Code | Key Differentiator |
|---|---|---|---|
| Lip Tie Release | D7960 or D7961 | CPT 40819 | D7961 is for gap closure; 40819 is for medical necessity. |
| Tongue Tie Release | D7960 or D7962 | CPT 41115 | D7962 specifies ankyloglossia; 41115 is the standard medical code. |
Why the Right Code Matters: A Story of Two Insurances
Imagine a family, the Millers, whose newborn baby is struggling to breastfeed. A lactation consultant identifies a severe tongue-tie. The dentist performs a lingual frenectomy using a laser.
Scenario A (Billed to Dental Insurance):
The dentist’s office bills the procedure using CDT code D7962. The Millers have dental insurance, but many dental plans have a low annual maximum (often $1,000-$2,000) and may classify this as a minor surgical procedure subject to a separate deductible. The insurance might pay a portion, but the family could still face a significant out-of-pocket expense. If they have no dental insurance, the full cost is theirs to bear.
Scenario B (Billed to Medical Insurance):
The dentist’s office, recognizing the medical nature of the problem (inability to feed), bills the procedure to the baby’s medical insurance using CPT code 41115, along with the appropriate diagnosis code. The medical plan, which is designed to cover health issues, processes the claim. After the family meets their medical deductible, the insurance may cover a much larger percentage, or even the entire cost, of the procedure.
This scenario highlights the immense financial impact of using the correct code. A procedure that might cost several hundred dollars out-of-pocket could be covered as a medical necessity under the patient’s health plan.
Key Takeaway for Patients: If your frenectomy is being performed to resolve a functional health issue (like feeding problems, speech difficulties, or sleep apnea), ask your provider if they will submit a claim to your medical insurance. You will likely need to provide your medical insurance card, not just your dental card.
The Essential Role of ICD-10 Diagnosis Codes
A CPT code tells the insurance company what you did. An ICD-10 (International Classification of Diseases, 10th Revision) code tells them why you did it. The “why” is arguably the most important part of the claim, especially for medical insurance.
For a frenectomy claim to be paid by medical insurance, the diagnosis code must justify the medical necessity of the procedure. Here are the most common ICD-10 codes used:
For Lingual Frenectomy (CPT 41115)
-
Q38.1: Ankyloglossia (Tongue Tie). This is the congenital condition code. It is the most common and powerful code for justifying a lingual frenectomy in infants and children.
-
R47.82: Fluency disorder in conditions classified elsewhere. This can be used for speech difficulties related to tongue mobility.
-
R13.0: Aphagia and dysphagia. This refers to difficulty swallowing.
-
P92.5: Neonatal difficulty in feeding at breast. This is a crucial code for newborns who are failing to latch or transfer milk effectively due to a tongue tie.
For Labial Frenectomy (CPT 40819)
-
Q38.0: Congenital malformations of lips, not elsewhere classified. This can be used for a congenital “lip tie.”
-
K05.30: Chronic periodontitis, unspecified. Used if the frenum is pulling on the gums and causing recession or periodontal issues.
-
K08.1: Loss of teeth due to accident, extraction, or local periodontal disease. Sometimes used in cases where a high frenum impacts denture stability.
-
E66.9: Obesity, unspecified. This is an emerging area, as restrictive frena can sometimes be linked to breathing issues and sleep-disordered breathing (sleep apnea), but this is less common and requires extensive documentation.
The Importance of Linking:
On a claim form (like the CMS-1500 form for medical claims), the CPT code and the ICD-10 code are “linked.” The insurance company will ask: “Is a lingual frenectomy (CPT 41115) a reasonable and necessary treatment for a patient with ankyloglossia (ICD-10 Q38.1)?” The answer is almost always yes. This is how a claim gets paid.
When is a Frenectomy Considered “Medically Necessary”?
Insurance companies don’t pay for everything. They pay for things that are “medically necessary.” This is the biggest hurdle in getting a claim approved. Understanding how insurers view this will help you set realistic expectations.
Here is how medical necessity is typically defined for frenectomies:
For Infants (Lingual)
Medical necessity is usually proven through:
-
Diagnosis of Ankyloglossia: A qualified provider (pediatrician, ENT, or pediatric dentist) confirms a tongue-tie using a standardized assessment tool (like the Hazelbaker Assessment Tool for Lingual Frenulum Function).
-
Documented Feeding Difficulties: A lactation consultant’s or physician’s note detailing poor latch, maternal nipple pain, poor weight gain, or the baby’s inability to transfer milk effectively.
For Children/Adults (Lingual)
-
Speech Difficulties: An assessment by a speech-language pathologist (SLP) documenting that the restricted tongue movement is contributing to articulation problems.
-
Oral Hygiene Issues: Inability to clear food debris from the mouth, leading to decay or periodontal disease.
-
Mechanical/Social Issues: Difficulty licking lips, playing a wind instrument, or kissing comfortably.
For Labial Frenectomy
-
Diastema Closure: In orthodontic cases, if a large gap between the front teeth persists after braces, releasing the frenum can prevent the gap from reopening. This is often seen as necessary for the stability of orthodontic treatment.
-
Periodontal Health: If the frenum pulls on the gum margin, causing recession, food trapping, or inflammation, it is considered a threat to periodontal health.
-
Denture Stability: For denture-wearers, a high or restrictive frenum can prevent a denture from seating properly. Its removal is necessary for the function of the prosthetic.
A Word of Caution: “Cosmetic” reasons are rarely covered. If the goal is purely to improve the appearance of a smile without any functional impairment, it is highly unlikely that medical insurance will provide any coverage.
The Billing Process: What Patients Need to Know
If you are a patient preparing for a frenectomy, here is a step-by-step guide to navigating the insurance maze.
Step 1: Pre-Authorization (The Most Important Step)
Never assume coverage. Before the procedure, ask your provider’s billing department to perform a pre-authorization or predetermination of benefits. This involves sending the planned CPT codes (e.g., 41115) and the supporting ICD-10 codes (e.g., Q38.1, P92.5) to your medical insurance company. They will respond in writing with an estimate of what they will pay. This prevents nasty surprises after the fact.
Step 2: Verify Provider Network
Is your dentist or oral surgeon an “in-network” provider for your medical plan? Many dentists are not. If they are out-of-network, you may have higher out-of-pocket costs, or the claim might be processed differently. Ask this question upfront.
Step 3: Understand Your Benefits
Look at your medical insurance card and policy. You need to know:
-
Your deductible: How much you must pay before insurance kicks in.
-
Your co-insurance: The percentage you pay after the deductible (e.g., you pay 20%, insurance pays 80%).
-
Your out-of-pocket maximum: The most you will have to pay in a year.
Step 4: The Claim is Submitted
After the procedure, the provider’s office will submit a claim to your medical insurance company using the appropriate CPT and ICD-10 codes. They will send it to the address on your medical card.
Step 5: Receive an Explanation of Benefits (EOB)
The insurance company will send you and the provider an EOB. This document explains what was paid, what was denied, and what you owe. Compare this to any bill you receive from the provider.
Common Reasons for Claim Denials (and How to Fight Them)
Even with the best planning, claims can be denied. Here are the most common reasons and what you can do.
Denial Reason 1: “Not a Covered Benefit” / “Dental Procedure”
-
The Problem: The medical insurance company classifies the frenectomy as a dental procedure and therefore excludes it from coverage. This is the most common denial.
-
The Solution: This is where a letter of medical necessity (LMN) is crucial. Your provider must write a letter explaining that the procedure is not about “teeth” but about a functional health condition (feeding, speech, breathing). They need to frame the argument in medical, not dental, terms.
Denial Reason 2: “Lack of Medical Necessity”
-
The Problem: The submitted diagnosis codes (ICD-10) don’t convincingly support the need for the procedure in the eyes of the medical reviewer.
-
The Solution: Provide more documentation. This could be a letter from a lactation consultant, a speech therapy evaluation, or photos/videos showing the functional limitation. An appeal with stronger evidence often succeeds.
Denial Reason 3: “Provider is Out-of-Network”
-
The Problem: You went to a dentist who is not contracted with your medical plan.
-
The Solution: You can either appeal based on the lack of in-network providers in your area who perform the procedure (a “gap in network” appeal) or be prepared for the higher out-of-network costs. For future reference, look for a provider who is specifically “dual-credentialed” (in-network with dental and medical plans).
Laser Frenectomy vs. Traditional: Does it Change the Code?
A common question is whether using a laser commands a different, higher-paying code. The answer is generally no.
-
CPT codes describe the service (e.g., Excision of lingual frenum), not the method. Whether the doctor uses a scalpel, scissors, or a laser, the primary code is still CPT 41115.
-
Similarly, the dental codes (D7960, D7962) remain the same regardless of the instrument used.
However, a provider may charge a higher fee for a laser procedure due to the cost of the equipment, disposables, and the advanced training required. This is a matter of the provider’s practice fees, not the insurance code. This difference between the provider’s fee and what the insurance allows is often passed on to the patient.
Frequently Asked Questions (FAQ)
1. Does medical or dental insurance cover frenectomy?
It depends on the reason. If it’s for a functional health problem (feeding, speech), medical insurance is the better option. If it’s purely related to orthodontic tooth movement or gum health, it may be billed to dental insurance. Some patients with both types of insurance may see a coordination of benefits.
2. What is the typical cost of a frenectomy without insurance?
The cost varies widely by geographic location and provider. For a laser frenectomy, you might expect to pay anywhere from $400 to $1,200 or more. An initial consultation fee is often separate.
3. Is frenectomy covered by Medicare or Medicaid?
Coverage varies by state for Medicaid. Some states cover frenectomy for infants with documented feeding problems. Original Medicare (Part B) may cover it if it is deemed medically necessary for a health condition, though it is less common for adults.
4. At what age is it best to have a frenectomy?
For tongue-tie, many professionals recommend addressing it in infancy (0-12 months) if it’s causing feeding issues. This can prevent a host of problems down the road. However, frenectomies can be successfully performed on children, teens, and adults at any age.
5. How long does it take to recover from a frenectomy?
Recovery is typically quick. With laser procedures, healing often takes just a few days to a week. Infants usually bounce back within 24 hours. Stretches and exercises are often prescribed to prevent the tissue from reattaching as it heals.
Conclusion
In summary, navigating the dental code for frenectomy requires a clear understanding of the distinction between dental and medical billing. The key lies in using the correct CPT codes—40819 for labial and 41115 for lingual procedures—and supporting them with the appropriate ICD-10 diagnosis codes that prove medical necessity. For patients, the path to coverage starts with verifying benefits and seeking pre-authorization, ensuring that this vital procedure is accessible and affordable.
Disclaimer: This article is for informational purposes only and does not constitute legal or financial advice. Medical billing and coding are complex and subject to change based on payer policies, contracts, and individual patient plans. Always consult with your insurance provider and healthcare provider regarding coverage and financial responsibility.





