In the vast and intricate world of healthcare, few disciplines intertwine as consequentially as clinical cardiology and medical coding. Coronary Artery Disease (CAD), the leading cause of morbidity and mortality worldwide, is not just a pathophysiological process; it is a complex narrative documented in patient charts and translated into a precise alphanumeric language: the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). For the medical coder, mastering CAD coding is an exercise in clinical understanding, meticulous attention to detail, and rigorous adherence to guidelines. An incorrectly assigned code is not merely a clerical error; it can distort epidemiological data, impede clinical research, trigger claim denials, and expose a healthcare organization to significant compliance risks. This article delves beyond the basic code lookup, offering a deep, exhaustive exploration of ICD-10-CM coding for CAD. We will dissect the hierarchy, unravel the nuances of clinical documentation, and equip you with the knowledge to navigate this complex category with confidence, ensuring that every code you assign accurately reflects the patient’s condition and supports the integrity of the healthcare system.
ICD-10-CM Coding for Coronary Artery Disease
2. The Anatomy of a Code: Understanding the ICD-10-CM Structure for CAD
ICD-10-CM codes for CAD reside primarily within chapter I00-I99, “Diseases of the Circulatory System.” The specific category is I25, Chronic ischemic heart disease. This parent code encompasses a range of chronic conditions resulting from reduced blood supply to the heart muscle. Understanding the structure is key to accurate selection.
-
I25 – Chronic ischemic heart disease
-
I25.1 – Atherosclerotic heart disease of native coronary artery
-
I25.10 – … without angina pectoris
-
I25.11 – … with angina pectoris
-
I25.110 – … with unstable angina
-
I25.111 – … with vasospastic angina
-
I25.118 – … with other forms of angina pectoris
-
I25.119 – … with unspecified angina pectoris
-
-
-
I25.2 – Old myocardial infarction
-
I25.5 – Ischemic cardiomyopathy
-
I25.7 – Atherosclerosis of coronary artery bypass graft(s) and coronary artery of transplanted heart with angina pectoris
-
I25.71 – Atherosclerosis of coronary artery bypass graft(s) with angina pectoris
-
(Further 5th and 6th character specificity for type of angina)
-
-
I25.72 – Atherosclerosis of coronary artery of transplanted heart with angina pectoris
-
-
I25.81 – Atherosclerosis of coronary artery bypass graft(s) without angina pectoris
-
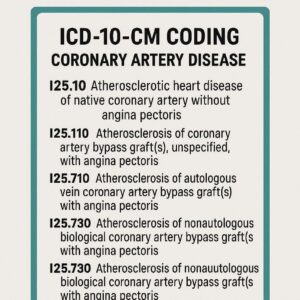
I25.810 – … of autologous vein bypass graft
-
I25.811 – … of autologous artery bypass graft
-
I25.812 – … of nonautologous biological bypass graft
-
I25.818 – … of other coronary artery bypass graft
-
I25.819 – … of unspecified coronary artery bypass graft
-
-
I25.82 – Chronic total occlusion of coronary artery
-
I25.83 – Coronary atherosclerosis due to lipid rich plaque
-
I25.84 – Coronary atherosclerosis due to calcified coronary lesion
-
I25.89 – Other forms of chronic ischemic heart disease
-
I25.9 – Chronic ischemic heart disease, unspecified
-
This hierarchical structure demands specificity. The coder must navigate from the general (chronic ischemia) to the precise (e.g., atherosclerosis of a native artery with vasospastic angina). The following sections will break down each critical subcategory.
3. I25.10 – The Foundation: Atherosclerotic Heart Disease of Native Coronary Artery Without Angina
I25.10 is a frequently used code, but its application must be precise. It represents a confirmed diagnosis of atherosclerosis (plaque buildup) in the patient’s own (native) coronary arteries, but the patient is not currently experiencing angina pectoris. This is a crucial distinction.
Clinical Context: This code is appropriate for patients with:
-
A history of a positive diagnostic test (e.g., coronary CT angiography showing >70% stenosis, abnormal cardiac stress test) confirming CAD.
-
Status post percutaneous coronary intervention (PCI) or stent placement for a past event, who are now asymptomatic. (Note: A code from Z98.61-Z98.62 should be added as an additional code to show the status of a coronary angioplasty or stent).
-
Documentation of “CAD,” “coronary atherosclerosis,” or “ischemic heart disease” without any mention of chest pain or anginal equivalent symptoms during the current encounter.
Documentation Requirements: The provider must explicitly state the diagnosis. Terms like “known CAD,” “history of CAD,” or “coronary artery disease” are generally sufficient to assign I25.10, provided there is no associated angina. Coders cannot infer atherosclerosis from risk factors like hypertension or hyperlipidemia alone.
4. The Spectrum of Angina: Decoding I25.11x and I25.7xx
Angina pectoris—cardiac chest pain due to ischemia—adds a critical layer of specificity. The ICD-10-CM system meticulously classifies angina types.
I25.11x: Atherosclerotic heart disease of native coronary artery WITH angina pectoris.
This category requires a 5th character to specify the angina type.
-
I25.110 – Unstable Angina (UA): Also known as “crescendo angina” or pre-infarction angina. It is characterized by pain that occurs at rest, is new in onset, or is increasing in frequency, duration, or intensity. It is part of the Acute Coronary Syndrome (ACS) spectrum. Crucial Note: If the provider documents “unstable angina” or “ACS,” I25.110 is correct. If they document a more specific ACS diagnosis like NSTEMI, codes from I21.0-I21.4 take precedence.
-
I25.111 – Vasospastic Angina (Prinzmetal’s Angina): Caused by a transient spasm of a coronary artery, often occurring at rest and not necessarily linked to atherosclerosis severity.
-
I25.118 – Other forms of angina pectoris: This includes stable angina (angina that is predictable and occurs with exertion or stress), microvascular angina, and other specified types.
-
I25.119 – Unspecified angina pectoris: Used only when the provider documents “angina” without specifying the type.
I25.7xx: Atherosclerosis of Bypass Grafts and Transplanted Hearts WITH Angina.
This category is for patients who have undergone surgical revascularization (CABG) or heart transplantation and have developed atherosclerosis in those grafts/arteries, and present with angina.
-
I25.71x: For CABG grafts (requires 6th character for angina type: 0,1,8,9).
-
I25.72x: For the coronary arteries of a transplanted heart (requires 6th character for angina type).
ICD-10-CM Code Selection Guide for Common CAD Presentations
| Clinical Scenario & Provider Documentation | Primary ICD-10-CM Code | Rationale & Key Considerations |
|---|---|---|
| Asymptomatic CAD: “Patient with known CAD, s/p stent to LAD 2 years ago, here for routine follow-up. No chest pain.” | I25.10 | Atherosclerosis of native coronary artery is present, but no angina is reported during this encounter. Add: Z98.61 (Intracoronary stent status). |
| Stable Angina: “Patient with CAD presents with typical exertional chest pressure, relieved with rest and nitroglycerin. Symptoms unchanged from prior.” | I25.118 | Atherosclerotic heart disease is documented with specified angina (stable). |
| Unstable Angina / ACS: “Patient admitted with sudden onset of rest chest pain, EKG shows ST-depression, troponin negative. Diagnosis: Unstable Angina.” | I25.110 | Unstable angina is explicitly diagnosed as part of ACS. If troponin were elevated, an I21.- code would be primary. |
| Post-MI, Asymptomatic: “History of inferior wall MI in 2020. Now presents for HTN management. No cardiac symptoms.” | I25.2 | The old/healed MI is the relevant chronic ischemic heart condition. I25.10 would be incorrect as the cause (MI sequelae) is known. |
| CAD with Heart Failure: “Patient with ischemic cardiomyopathy presents with acute decompensated heart failure, ejection fraction 30%.” | I25.5 (Primary) I50.9 or I50.2x (Secondary) | Ischemic cardiomyopathy is the cause of the heart failure and is sequenced first per coding guidelines. |
| S/P CABG with Graft Atherosclerosis & Angina: “Patient with prior CABG presents with recurrent stable angina. Cath shows significant atherosclerosis in the saphenous vein graft.” | I25.710 (if unstable: I25.711, etc.) | Atherosclerosis is specifically in the bypass graft, accompanied by angina. Specifies graft type if known. |
| Chronic Total Occlusion (CTO): “Cardiac cath reveals a 100% chronic total occlusion of the RCA, collateralized. Patient is asymptomatic.” | I25.82 | This is a specific anatomical finding of chronic ischemia, coded independently. May be used with I25.10. |
5. The Sequela of Infarction: Navigating Old and Healed Myocardial Infarctions (I25.2)
Code I25.2, Old myocardial infarction, is used for a history of MI that occurred in the past and is now considered healed or old. The acute phase has passed (typically > 4 weeks), but the sequela remains.
-
Application: Use for documented “old MI,” “healed MI,” “prior MI,” “status post MI,” or “myocardial fibrosis due to old infarct.”
-
Excludes: Never use I25.2 for a current, acute MI (I21.-) or a subsequent MI (I22.-). The guidelines are clear that I25.2 is for conditions stated as history or old.
-
Clinical Significance: This code captures the lasting impact of an MI, such as scarred myocardium, which is vital for risk stratification and explaining conditions like ischemic cardiomyopathy (I25.5).
6. Specificity is King: Coding for Atherosclerosis of Coronary Artery Bypass Grafts and Other Forms
The ICD-10-CM system demands extreme specificity for post-surgical states.
-
I25.81x – Atherosclerosis of coronary artery bypass graft(s) WITHOUT angina pectoris: Parallels I25.10 but for grafts. The 5th and 6th characters specify the graft type (autologous vein, artery, etc.). This is critical for outcomes tracking.
-
I25.82 – Chronic total occlusion of coronary artery: A specific code for a completely blocked artery, a key finding in interventional cardiology. It can be used alongside other I25 codes.
-
I25.83 & I25.84: These codes (lipid-rich plaque, calcified lesion) offer unprecedented pathologic specificity, mainly used in research contexts or when detailed imaging or intravascular ultrasound (IVUS) provides such characterization.
7. Acute Coronary Syndromes (ACS): Where CAD Coding Meets Urgency
While chronic codes are under I25, acute events have their own categories. This is a major point of confusion.
-
I20.-, Angina pectoris: Includes unstable angina (I20.0), but note the direct conflict with I25.110. Coding Clinic guidance dictates that when CAD is documented with unstable angina, I25.110 is used. I20.0 is for unspecified or non-atherosclerotic unstable angina.
-
I21.-, Acute myocardial infarction: This is the primary code for a current acute MI (STEMI, NSTEMI). It replaces any chronic CAD code (I25.-) for that encounter’s principal diagnosis. The type of MI (inferior, anterior, etc.) is specified with 4th and 5th characters.
-
I22.-, Subsequent ST elevation (STEMI) and non-ST elevation myocardial infarction (NSTEMI): For a new acute MI occurring within 4 weeks of a previous one.
Hierarchy Rule: In an encounter for an acute MI, the acute MI code (I21.- or I22.-) is always principal. A code from I25.- (like I25.2 for the old MI or I25.10 for underlying CAD) may be assigned as an additional code to show the full history.
8. The Power of Combination: Using Additional Codes for Complete Clinical Picture
Accurate CAD coding rarely involves a single code. The ICD-10-CM system encourages a holistic picture.
-
Risk Factors: Always add codes for conditions like:
-
E11.9 – Type 2 diabetes mellitus
-
I10 – Essential (primary) hypertension
-
E78.5 – Hyperlipidemia
-
F17.2- – Tobacco dependence
-
-
Status Post Procedures: Z codes are essential.
-
Z95.5 – Presence of coronary angioplasty implant (stent) and graft
-
Z98.61 – Coronary angioplasty status (with or without stent)
-
Z95.1 – Presence of aortocoronary bypass graft
-
-
Associated Conditions:
-
I50.- – Heart failure (often linked with I25.5, Ischemic cardiomyopathy)
-
R07.9 – Chest pain, unspecified (if documented but not clearly anginal)
-
9. The Documentation Imperative: What Coders Need from Providers
The coder’s accuracy is bound by the clinician’s documentation. Clear documentation should specify:
-
The Etiology: “Atherosclerotic,” “ischemic.”
-
The Location/Vessel: “Native vessel,” “bypass graft,” “LAD,” “RCA.”
-
The Clinical Presentation: “Asymptomatic,” “with stable angina,” “with unstable angina,” “with heart failure.”
-
The Chronology: “Acute,” “chronic,” “history of,” “old,” “healed.”
-
Related Conditions: “Ischemic cardiomyopathy,” “chronic total occlusion.”
A query process is essential when documentation is unclear, contradictory, or uses non-specific terms like “CAD” without context.
10. Common Pitfalls, Audits, and Compliance Risks
-
Miscoding Stable vs. Unstable Angina: Assuming all angina is stable. This affects DRG assignment and reimbursement.
-
Using I25.2 for Recent MI: Applying the old MI code to an acute event is a serious error.
-
Ignoring Laterality/Specificity: Not using available 5th/6th characters for angina type or graft type.
-
Overlooking Additional Codes: Failing to code significant risk factors or status post procedures.
-
Code Conflict Errors: Using both I25.110 and I20.0 for the same diagnosis.
These pitfalls are prime targets for Recovery Audit Contractors (RACs) and other audit entities, leading to takebacks and penalties.
11. Case Studies: Applying Knowledge to Real-World Scenarios
Case 1: A 68-year-old male with a history of hypertension and tobacco use presents to the ED with 45 minutes of severe, crushing substernal chest pain at rest. EKG shows ST-elevation in leads V2-V4. Troponin is elevated. The cardiologist documents “Acute Anterior Wall STEMI.”
-
Coding: I21.09 (STEMI involving other coronary artery – anterior wall). Additional codes: I25.10 (underlying CAD), I10 (HTN), F17.210 (tobacco dependence).
Case 2: A 72-year-old female, s/p CABG (saphenous vein graft) 8 years ago, sees her cardiologist for worsening chest tightness when walking up one flight of stairs. Symptoms are relieved within 5 minutes of rest. A recent CT angiogram showed >70% stenosis in the vein graft.
-
Coding: I25.718 (Atherosclerosis of coronary artery bypass graft(s) with other forms of angina pectoris – stable angina). Additional code: Z95.1 (Presence of aortocoronary bypass graft).
12. Conclusion: The Coder’s Role in the CAD Care Continuum
Mastering ICD-10-CM coding for Coronary Artery Disease transcends mere code assignment; it is an integral part of patient care logistics, healthcare economics, and clinical data integrity. The coder, armed with deep knowledge of the code set’s structure, a clear understanding of cardiovascular pathophysiology, and an unwavering commitment to documentation specificity, acts as a vital translator between the clinical story and the data that drives modern medicine. By ensuring precision in every code—from the broad category of chronic ischemia to the granular detail of graft atherosclerosis with vasospastic angina—coders safeguard accurate reimbursement, support quality metrics, and contribute to the robust data essential for advancing the fight against heart disease.
13. Frequently Asked Questions (FAQs)
Q1: What is the difference between I25.10 and I25.119?
A: I25.10 is for patients with diagnosed atherosclerotic CAD who have no angina. I25.119 is for patients with diagnosed atherosclerotic CAD who DO have angina, but the provider has not specified the type (stable, unstable, etc.).
Q2: When do I use I25.5 (Ischemic cardiomyopathy)?
A: Use I25.5 when the provider explicitly links dilated or dysfunctional cardiomyopathy (often with reduced ejection fraction/heart failure) to underlying ischemic heart disease. It is sequenced first, followed by a heart failure code (I50.-).
Q3: Can I code both an acute MI (I21.-) and chronic CAD (I25.-) on the same claim?
A: Yes. The acute MI (I21.-) would be the principal diagnosis. A code from I25.- (such as I25.10 for the underlying CAD or I25.2 for an old, separate MI) can and should be added as a secondary code to complete the clinical picture.
Q4: The provider only documents “CAD” in the assessment. What code do I use?
A: The default code for unspecified chronic ischemic heart disease is I25.9. However, a query to the provider is highly recommended to clarify if the patient has angina and if the CAD is atherosclerotic, as this will allow for a more specific (and often more appropriate) code like I25.10 or I25.119.
Q5: How do I code a patient with a coronary stent who is having angina?
A: First, determine the location of the disease. Is the atherosclerosis in the native artery or in the stent itself (in-stent restenosis)? For native artery disease with angina, use I25.11x. For restenosis within the stent, it is still considered disease of the native artery, so I25.11x is still used. Always add Z98.61 to indicate the stent status.
14. Additional Resources and References
-
Official ICD-10-CM Guidelines: Centers for Disease Control and Prevention (CDC) / National Center for Health Statistics (NCHS) – The definitive source for coding rules.
-
AHA Coding Clinic for ICD-10-CM/PCS: American Hospital Association – Provides official advice and clarifications on complex coding scenarios, including cardiology.
Disclaimer: This article is for informational purposes only and is intended for healthcare professionals and medical coders. It does not constitute medical or coding advice. Code selection must always be based on provider documentation, official ICD-10-CM coding guidelines, and the most current code sets. Always consult the latest official resources for accurate coding.
Date: December 16, 2025
Author: Medical Coding & Cardiovascular Billing Specialists