When a patient transitions from curative treatment to comfort-focused care, the language we use in medical records must shift as well. For healthcare providers, medical coders, and administrators, this shift is documented through specific codes. Finding the correct ICD-10 code for end of life care is not just a bureaucratic task; it is a crucial step in ensuring that a patient’s journey is respected, that the facility is reimbursed correctly, and that the data reflects the true nature of the care provided.
If you have ever stared at a screen wondering whether to use a Z code, a symptom code, or a diagnosis code for a hospice patient, you are not alone. This guide is designed to walk you through the nuances, offering clarity in a field that often feels gray.
Let’s break down the codes, the rules, and the realities of coding for the final chapter of life.
ICD-10 Code for End of Life Care
What Is End of Life Care in Medical Terms?
Before we dive into the alphanumeric world of ICD-10, it is vital to understand what we are actually coding for. In a medical context, “end of life care” is not a disease. It is a phase of treatment.
End-of-life care refers to the support and medical care given during the time surrounding death. This can be in the final weeks or months, and it includes:
-
Palliative care: Symptom management (pain, shortness of breath, anxiety).
-
Hospice care: A specific form of palliative care for those with a terminal diagnosis, typically when life expectancy is six months or less.
-
Comfort measures: Stopping aggressive treatments and focusing solely on quality of life.
Because this phase involves managing symptoms rather than curing a disease, the coding logic changes. You cannot simply code “dying” as a primary condition.
The Difference Between Hospice and Palliative Care
This is a critical distinction for coding. While the terms are often used interchangeably in conversation, they represent different billing scenarios.
-
Palliative Care: Can be provided at any stage of a serious illness, alongside curative treatment. The goal is to improve quality of life.
-
Hospice Care: Is specifically for the end of life. The patient has elected to forego curative treatment and focuses entirely on comfort.
This distinction matters because the ICD-10 code for end of life care you choose will depend on whether the patient is in a general palliative care plan or a formal hospice benefit period.
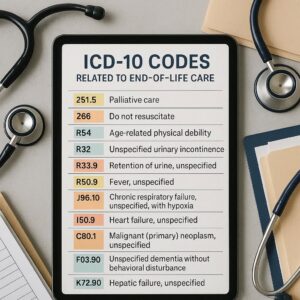
The Primary Code: Z51.5
If there is one code you need to remember for this topic, it is Z51.5.
-
Code: Z51.5
-
Description: Encounter for palliative care
This is the dedicated code used to indicate that the primary reason for an encounter (a hospital stay, a home visit, a nursing home admission) is to receive palliative care. It tells the story that the patient is no longer seeking diagnostic testing or curative therapies; they are there for symptom control and comfort.
When to Use Z51.5
You should use Z51.5 when the documentation clearly states that the patient is receiving palliative care. This is often the “primary diagnosis” or “first-listed diagnosis” on a claim for hospice or palliative care services.
For example:
-
A patient with terminal lung cancer is admitted to a hospice facility for pain management. The admission diagnosis is Z51.5.
-
A home health nurse visits a patient with advanced heart failure to adjust their comfort medications. The primary reason for the visit is Z51.5.
Rules for Using Z51.5
However, there is a golden rule in coding: You never code just Z51.5 alone.
In the world of ICD-10, Z codes (factors influencing health status) are almost always secondary to a diagnosis code that describes the underlying condition. You must link the palliative care encounter to the condition that necessitates it.
Therefore, the correct coding structure looks like this:
-
Primary Code: Z51.5 (Encounter for palliative care)
-
Secondary Code: The underlying terminal condition (e.g., C34.90 for Lung cancer, or I50.9 for Heart failure).
This combination tells the full clinical story: “This patient has heart failure, and they are here to receive palliative care for it.”
Alternative and Supporting Codes
While Z51.5 is the star of the show, it is rarely the only code on a claim. End-of-life care involves managing multiple, complex symptoms. These symptoms must also be coded to justify the intensity of the care provided.
Coding Symptoms in End-of-Life Care
During the final stages of life, specific symptoms become the focus of treatment. These are often coded as additional diagnoses to provide a complete picture.
Here are the most common symptoms and their corresponding codes:
| Symptom | Common ICD-10 Code | Description |
|---|---|---|
| Severe Pain | G89.3 | Neoplasm related pain (Acute, chronic) |
| R52 | Pain, unspecified | |
| Shortness of Breath | R06.02 | Shortness of breath |
| Difficulty Breathing | R06.09 | Other forms of dyspnea |
| Nausea | R11.2 | Nausea with vomiting, unspecified |
| Fatigue | R53.83 | Other fatigue (often cancer-related) |
| Anxiety | F41.9 | Anxiety disorder, unspecified |
| Cachexia | R64 | Wasting syndrome |
| Constipation | K59.00 | Constipation, unspecified |
| Difficulty Swallowing | R13.10 | Dysphagia, unspecified |
Important Note: If the patient has a known history of cancer, pain should be coded as G89.3 (Neoplasm related pain) rather than a general R52 code, as it is more specific and paints a more accurate clinical picture.
Coding the Underlying Terminal Condition
As mentioned, you cannot use Z51.5 without linking it to the condition that is causing the decline. This is the “chronic” or “terminal” diagnosis.
-
Malignant Neoplasm (Cancer): Codes range from C00 to C96. You need to be as specific as possible regarding the site (e.g., C34.90 for lung cancer).
-
Heart Failure: I50.9 (Unspecified) or I50.32 (Chronic diastolic) etc.
-
Chronic Obstructive Pulmonary Disease (COPD): J44.9
-
Alzheimer’s Disease: G30.9 (often paired with F02.80 for dementia)
-
End-Stage Renal Disease (ESRD): N18.6 (often requiring dialysis, Z99.2)
Common Coding Scenarios and Examples
To make this practical, let’s look at how these codes come together in real-world documentation.
Scenario 1: The Cancer Patient in Hospice
-
The Story: A 78-year-old with metastatic breast cancer is admitted to an inpatient hospice unit. The main issues are uncontrolled bone pain and anxiety about the process.
-
The Codes:
-
Z51.5 (Encounter for palliative care)
-
C50.91 (Malignant neoplasm of unspecified site of female breast)
-
G89.3 (Neoplasm related pain)
-
F41.9 (Anxiety disorder, unspecified)
-
Scenario 2: The Heart Failure Patient at Home
-
The Story: A home health agency starts palliative care services for an 82-year-old man with end-stage heart failure. The primary goal is to manage his severe shortness of breath (dyspnea) so he can remain comfortable at home.
-
The Codes:
-
Z51.5 (Encounter for palliative care)
-
I50.9 (Heart failure, unspecified)
-
R06.02 (Shortness of breath)
-
Scenario 3: The Dementia Patient in a Facility
-
The Story: A patient in a long-term care facility with advanced Alzheimer’s disease has stopped eating and is experiencing significant pain, though they cannot verbally communicate it (evidenced by facial grimacing).
-
The Codes:
-
Z51.5 (Encounter for palliative care)
-
G30.9 (Alzheimer’s disease, unspecified)
-
F02.80 (Dementia in Alzheimer’s disease)
-
R52 (Pain, unspecified) or G89.3 if cancer is present.
-
Coding Pitfalls to Avoid
Accuracy in coding for end-of-life care is essential for compliance and reimbursement. Here are the most common traps and how to avoid them.
1. The “Impending Death” Trap
There is no code for “impending death” or “dying.” You must always code the symptoms and the underlying condition. Using vague codes like R99 (Ill-defined and unknown cause of mortality) is only for very specific circumstances (like a found body) and is inappropriate for a living patient receiving care.
2. Listing Symptoms Without a Diagnosis
Payers (like Medicare) need to see the “why.” If you submit a claim with only R06.02 (shortness of breath) and R53.83 (fatigue), it looks like a general illness. If you pair those with Z51.5 and I50.9 (heart failure), it tells the story of a heart failure patient at the end of life requiring comfort care.
3. Using Outdated Codes
Medical coding changes every year. Codes are added, deleted, or revised every October 1st. Always ensure your software and coding manuals are updated to the latest version to avoid rejections.
Z51.5 vs. Other Related Z Codes
It is easy to confuse Z51.5 with other “encounter” codes. Here is how they differ:
| Code | Description | When to Use |
|---|---|---|
| Z51.5 | Encounter for palliative care | The patient is receiving symptom management and comfort care, often (but not exclusively) at the end of life. |
| Z51.1 | Encounter for antineoplastic chemotherapy | The patient is receiving chemotherapy to treat cancer (curative or maintenance). |
| Z51.0 | Encounter for antineoplastic radiation therapy | The patient is receiving radiation. |
| Z51.89 | Encounter for other specified aftercare | General aftercare not classified elsewhere. |
| Z76.89 | Persons encountering health services in other specified circumstances | A very vague code; avoid using this for palliative care if Z51.5 is more appropriate. |
Key Insight: A patient receiving chemotherapy (Z51.1) is generally not in the hospice phase, but they could be receiving concurrent palliative care (Z51.5) for pain management. In that case, both codes could be used, but the primary reason for the visit dictates the order.
The Future of End-of-Life Coding
As the population ages, the focus on palliative and end-of-life care is growing. The ICD-10 system is constantly evolving to capture this data better.
Currently, there is a push for more specificity regarding the type of palliative care (inpatient, outpatient, hospice) within the coding structure, but as of now, Z51.5 remains the primary workhorse. We are also seeing a greater emphasis on coding social determinants of health (Z55-Z65), such as the lack of a caregiver (Z74.2) or problems living alone (Z60.2), which heavily influence end-of-life planning and care.
Conclusion
Finding the right ICD-10 code for end of life care is about more than just billing. It is about documenting a deeply human experience with accuracy and respect. The cornerstone of this process is Z51.5 (Encounter for palliative care) , always paired with the underlying terminal diagnosis and the specific symptoms being managed.
By moving away from the idea of coding “death” and focusing on coding the care provided—the pain management, the relief of dyspnea, the comfort measures—we ensure that the medical record reflects the true, compassionate work being done for patients and their families during their most vulnerable time.
Frequently Asked Questions (FAQ)
1. Is Z51.5 the same as a hospice code?
Not exactly. Z51.5 is the code for palliative care encounters. While hospice care is a form of palliative care (specifically for the end of life), Z51.5 can also be used for palliative care provided outside of the formal hospice benefit period. For billing the hospice benefit itself, you use specific revenue codes, but Z51.5 remains the primary diagnosis code on the claim.
2. Can I use Z51.5 if the patient is still receiving treatment?
Yes. Palliative care (Z51.5) can be provided alongside curative treatment. This is common in modern medicine. However, if the patient is under the hospice benefit, they have waived curative treatment.
3. What is the ICD-10 code for “failure to thrive” at the end of life?
“Failure to thrive” in adults is coded as R54. However, for end-of-life patients, it is often better to code the specific debility or the underlying disease process causing the decline. R54 is a symptom code and should be used with a primary diagnosis.
4. What if the patient has multiple terminal conditions?
List them all. If a patient has both COPD and Heart failure, code both. The documentation should support which one is the primary driver of the current decline, but all relevant chronic conditions should be reported.
5. Do I need a different code for a “Do Not Resuscitate” (DNR) order?
No. DNR status is a physician’s order, not a diagnosis. It is not coded in ICD-10. It is documented elsewhere in the medical record.
Additional Resource
For the most up-to-date coding guidelines and annual updates, the definitive resource is the Centers for Medicare & Medicaid Services (CMS) and the American Hospital Association (AHA) Coding Clinic.
Disclaimer: This article is for informational purposes only and does not constitute legal or professional medical coding advice. Medical coding regulations, especially those involving Medicare and hospice, are complex and subject to change. Always consult with a certified professional coder or your facility’s compliance department to ensure accuracy and adherence to current guidelines.