If you have recently glanced at a medical report, a bill, or a referral letter and seen the alphanumeric string “M51.26” staring back at you, you might have felt a moment of confusion. It looks like a secret code—and in a way, it is. In the vast world of healthcare, we use these specific codes to communicate complex diagnoses quickly and accurately.
The good news? These codes are actually designed to bring clarity, not confusion. Understanding your ICD-10 code can help you take control of your health journey, understand your medical records, and have more informed conversations with your doctors.
In this guide, we are going to unpack everything you need to know about the ICD-10 code for M51.26. We will break down the medical jargon, explain what this diagnosis means for your body, and guide you through the next steps.
By the time you finish reading, you will be an expert on what M51.26 stands for and why it matters for your health.
ICD-10 Code for M51.26
What Exactly is an ICD-10 Code?
Before we dive into the specifics of M51.26, let’s take a step back. Think of ICD-10 codes as the universal language of medicine.
ICD stands for the International Classification of Diseases. It is a system used by doctors, hospitals, insurance companies, and public health officials around the world to classify every disease, symptom, injury, and health condition. The “10” stands for the 10th revision of this system, which is the current standard used in the United States and many other countries.
Why Do These Codes Matter to You?
You might think these codes are just for insurance billing, and while that is a huge part of it, they serve several important purposes:
-
For Insurance: They are the primary reason your claims get paid (or denied). The code tells your insurance company exactly what condition your doctor treated.
-
For Your Medical History: They create a clear, concise record of your health over time. This is incredibly helpful when you switch doctors or need to reference past issues.
-
For Public Health: Researchers and governments use this data to track disease outbreaks, study health trends, and allocate funding for research.
-
For Clarity: They remove ambiguity. “Lower back pain” can mean a hundred different things. An ICD-10 code pinpoints the specific issue.
Breaking Down the ICD-10 Code for M51.26
Now, let’s focus on our main subject. The code M51.26 looks complex, but it is actually a very logical description of a specific spinal condition. We can break it down piece by piece, almost like reading a sentence.
-
The “M” Chapter: In the ICD-10 system, the letter “M” covers a broad range of conditions. It stands for “Diseases of the musculoskeletal system and connective tissue.” So, right away, we know we are dealing with bones, muscles, or the tissues that support them.
-
The “51” Category: The numbers “51” narrow it down significantly. This category is officially titled: “Thoracic, thoracolumbar, and lumbosacral intervertebral disc disorders.” This tells us the problem lies in the cushioning discs between the bones of your spine (vertebrae), specifically in the lower and middle back regions.
-
The “.26” Specifics: The suffix after the decimal point is where we get the precise details. In this case, the “26” tells us two critical things:
-
The Type of Disorder: This code falls under “Other intervertebral disc disorders.” Specifically, it is often used for displacements or problems that haven’t been classified elsewhere.
-
The Location: The “2” in “26” indicates the thoracolumbar region. The “6” further specifies the side or level. In this context, M51.26 is often interpreted as a problem at the junction where the thoracic spine (mid-back) meets the lumbar spine (lower back), affecting multiple sites or an unspecified level within that region.
-
The Simple English Translation
So, if we put it all together, here is what M51.26 means in plain language:
“A disorder of the spinal disc located in the area where your mid-back meets your lower back (the thoracolumbar region).”
This usually refers to a problem like a herniated disc, a bulging disc, or disc displacement in that specific part of the spine.
The Anatomy Behind the Code: The Thoracolumbar Spine
To truly understand the ICD-10 code for M51.26, it helps to have a simple picture in your mind of what the thoracolumbar spine actually is.
The Spinal Regions: A Quick Tour
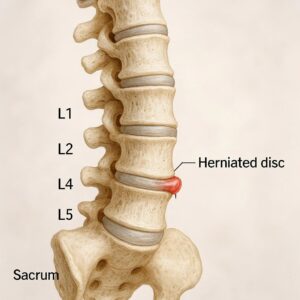
Imagine your spine as a column of building blocks (vertebrae) with soft, squishy pillows (discs) in between them. This column is divided into sections:
-
Cervical Spine (Neck): The top 7 vertebrae (C1-C7). Supports your head and allows you to nod and turn.
-
Thoracic Spine (Upper & Mid-Back): The next 12 vertebrae (T1-T12). These are attached to your ribs, forming a protective cage for your heart and lungs. This area is naturally less flexible.
-
Lumbar Spine (Lower Back): The next 5 vertebrae (L1-L5). These are the largest and strongest bones because they carry most of your body’s weight. This area is designed for bending and twisting.
-
Sacrum and Coccyx (Tailbone): The fused bones at the very bottom of the spine.
The Thoracolumbar Junction: The Crossroads
The thoracolumbar region isn’t a separate set of bones, but rather the “crossroads” where the thoracic spine meets the lumbar spine. This generally includes the last two thoracic vertebrae (T11 and T12) and the first two lumbar vertebrae (L1 and L2).
Why is this area so important and sometimes prone to issues?
-
A Transition Zone: This is where the relatively stiff, rib-supported thoracic spine meets the more flexible, weight-bearing lumbar spine.
-
A Biomechanical Focal Point: Because it connects a rigid area to a mobile one, the thoracolumbar junction experiences unique mechanical stress during bending, lifting, and twisting.
-
Nerve Root Pathways: Nerves that control muscles in the lower back, abdomen, and legs pass through this area.
When a disc disorder like M51.26 occurs here, it means the cushioning disc at this critical junction is damaged—it may be bulging, torn, or out of place.
What Does a Diagnosis of M51.26 Feel Like?
If you have been diagnosed with M51.26, you are likely experiencing some symptoms. It is important to remember that the disc problem itself is the anatomical issue, but the pain and other sensations are caused by the disc irritating nearby nerves.
Because the thoracolumbar junction is a complex area, the symptoms can sometimes be different from a typical “lower back injury.”
Common Symptoms of Thoracolumbar Disc Disorders
-
Localized Pain: You might feel a deep, aching pain right at the spot of the problem, usually in the very low part of the mid-back or the top of the lower back.
-
Radiating Pain (Referred Pain): This is a key symptom. Instead of just staying in your back, the pain may travel.
-
It can radiate into one or both of your hips.
-
It might wrap around to your lower abdomen or groin area. This is a classic sign of a thoracolumbar issue, as the nerves here serve those areas.
-
-
Stiffness: You may find it difficult to twist your torso or bend sideways. Simple actions like getting out of a car or turning to look behind you can be painful.
-
Muscle Spasms: The muscles in your lower back might tighten up uncontrollably as a protective response to the injury.
Symptoms of Nerve Compression (Radiculopathy)
If the displaced disc is pressing on a nerve root, you might experience more intense symptoms:
-
Numbness or Tingling: A “pins and needles” sensation in the legs, feet, or even the groin area.
-
Weakness: You might feel a lack of strength in one or both legs. You could find it hard to lift your foot (foot drop) or feel like your leg is going to give out when you stand up.
A Very Important Note:
If you experience sudden numbness in the groin or inner thighs along with a loss of bladder or bowel control, this is a medical emergency known as Cauda Equina Syndrome. You must seek emergency medical attention immediately.
How is M51.26 Diagnosed?
Getting to the code M51.26 isn’t something a doctor decides in five seconds. It is the result of a careful process to rule out other issues and confirm the specific problem.
1. The Patient History
Your doctor will start by asking detailed questions. They want to know:
-
When did the pain start?
-
What were you doing when it started? (e.g., lifting something, a fall, or no specific event?)
-
What does the pain feel like? (Ache, sharp, burning?)
-
Where exactly is the pain, and does it travel anywhere?
-
What makes it better or worse? (Sitting, standing, walking?)
2. The Physical Examination
Next, the doctor will examine you. They will:
-
Look at your posture and how you move.
-
Feel (palpate) your spine to find tender spots.
-
Test your range of motion (can you bend forward, backward, and side to side?).
-
Perform specific neurological tests, like checking your reflexes (knee jerks, ankle jerks), muscle strength in your legs, and sensation to light touch or pinprick.
3. Imaging Confirmation
While your history and physical exam might strongly suggest a disc disorder, imaging is needed to confirm the ICD-10 code for M51.26.
-
X-rays: These are often done first to look for fractures, alignment issues, or arthritis. They do not show discs.
-
MRI (Magnetic Resonance Imaging): This is the gold standard for diagnosing disc problems. An MRI provides detailed images of the soft tissues, including the discs, nerves, and spinal cord. It can clearly show if a disc is herniated, bulging, or pressing on a nerve. This scan is what definitively leads to the M51.26 diagnosis.
Treatment Pathways for M51.26
Receiving a diagnosis of a thoracolumbar disc disorder can be scary, but the vast majority of people improve with non-surgical treatment. The goal of treatment is to reduce pain, allow the disc to heal, and return you to your normal activities.
Here is a look at the typical treatment ladder.
Phase 1: Conservative (Non-Surgical) Care
For most patients, this is the first and only line of treatment needed.
-
Relative Rest (with a twist): Gone are the days of complete bed rest. Doctors now recommend relative rest. This means avoiding the specific activities that cause pain (like heavy lifting or twisting), but staying otherwise active. Short, gentle walks can actually help reduce stiffness and promote healing.
-
Medications:
-
Over-the-Counter (OTC): Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil, Motrin) or naproxen (Aleve) can help reduce inflammation and relieve pain. Acetaminophen (Tylenol) can help with pain but doesn’t affect inflammation.
-
Prescription: For more severe pain, a doctor might prescribe stronger NSAIDs, muscle relaxants to stop muscle spasms, or nerve pain medications like gabapentin.
-
-
Physical Therapy (PT): This is the cornerstone of recovery. A physical therapist will not just give you a list of exercises; they will build a personalized program to:
-
Strengthen the core muscles that support your spine.
-
Stretch tight muscles in the back, hips, and legs.
-
Improve posture and body mechanics to protect your spine during daily activities.
-
Use modalities like heat, ice, or ultrasound to manage pain.
-
Phase 2: Interventional Treatments
If conservative care doesn’t provide enough relief after several weeks or months, your doctor might suggest interventional options.
-
Epidural Steroid Injections: Under X-ray guidance, a doctor injects a powerful anti-inflammatory medication (corticosteroid) into the space around the spinal nerve roots. This can significantly reduce inflammation and pain, providing a “window of opportunity” for physical therapy to be more effective. It is a treatment, not a cure.
-
Nerve Blocks: Similar to injections, these are used for both diagnosis and treatment, numbing specific nerves to confirm they are the source of the pain.
Phase 3: Surgical Options
Surgery is rarely the first option. It is usually considered only if:
-
There is a severe neurological deficit (like progressive leg weakness).
-
There are signs of Cauda Equina Syndrome.
-
The pain is disabling and has not improved after 6 to 12 weeks of comprehensive non-surgical treatment.
If surgery is needed, common procedures for this area include:
-
Microdiscectomy: The surgeon removes the small piece of disc material that is pressing on the nerve.
-
Laminectomy: The surgeon removes a small piece of bone (lamina) to create more space for the nerves.
| Treatment Phase | Common Options | Primary Goal |
|---|---|---|
| Conservative | Relative Rest, OTC/Prescription Meds, Physical Therapy | Reduce pain and inflammation, restore function through natural healing. |
| Interventional | Epidural Steroid Injections, Nerve Blocks | Decrease severe pain to allow for more effective participation in PT. |
| Surgical | Microdiscectomy, Laminectomy | Physically remove the pressure on the nerve when other methods fail. |
Living Your Life with a M51.26 Diagnosis
An ICD-10 code is just a label for a moment in time. Your life is what you do with it afterward. Here is some practical advice for living well with this condition.
Ergonomics and Daily Habits
-
Desk Setup: If you work at a desk, ensure your chair supports the natural curve of your spine. Your feet should be flat on the floor, and your computer screen should be at eye level. Get up and move around every 30-45 minutes.
-
Lifting Technique: Never bend at the waist to pick something up. Instead, squat down by bending your knees, keep the object close to your body, and use your leg muscles to stand up. Think “lift with your legs, not with your back.”
-
Sleeping Positions: Sleeping on your side with a pillow between your knees can help keep your spine aligned. If you sleep on your back, place a pillow under your knees to reduce pressure on your lower spine.
The Role of Movement
It might seem counterintuitive to move when your back hurts, but gentle movement is often the best medicine.
-
Walking: It is low-impact, promotes blood flow, and helps keep your muscles from tightening up.
-
Swimming or Water Therapy: The buoyancy of water takes the weight off your spine, allowing you to move and exercise more freely and with less pain.
-
Mind-Body Practices: Gentle yoga, Pilates, and tai chi, when done with a qualified instructor who knows about your condition, can be excellent for building core strength, improving flexibility, and reducing stress.
An Encouraging Note:
Remember, your diagnosis is a roadmap, not a life sentence. Thousands of people are diagnosed with disc disorders like M51.26 every day, and the overwhelming majority return to full, active, and pain-free lives. Be patient with your body and consistent with your care.
The Billing and Coding Side of M51.26
For healthcare administrators, billers, and coders, understanding the nuances of M51.26 is crucial for accurate reimbursement and compliance.
Specificity is Key in ICD-10
One of the main principles of ICD-10 is specificity. The code M51.26 sits within a larger family of codes. Choosing the right one depends entirely on the documentation in the patient’s chart.
-
M51.25 would be used for the same type of disc disorder, but located specifically in the thoracic region (mid-back).
-
M51.26 is used for the thoracolumbar region (the junction).
-
M51.27 is used for the lumbosacral region (the junction of the lower back and the sacrum, which is the most common area for disc issues).
A coder must never guess. If the physician’s notes clearly state the problem is at the thoracolumbar junction, M51.26 is the correct code. If the notes only say “lower back,” the coder may need to query the physician for more details.
Common Coding and Billing Pitfalls
-
Inadequate Documentation: The most common mistake is a lack of specificity in the medical record. A report that just says “back pain” does not support a specific code like M51.26.
-
Coding from the Report Alone: Coders should ideally code from the physician’s final diagnosis, not just from an imaging report. An MRI might show a bulging disc, but if the physician determines it is not the source of the patient’s symptoms, it shouldn’t be coded as the primary diagnosis.
-
Ignoring Laterality: While M51.26 is often for unspecified or multiple sites in that region, if the physician notes the problem is on the left or right side, a more specific code should be used if available.
Important Note for Billers
Always ensure the ICD-10 code for M51.26 is linked to the appropriate CPT (Current Procedural Terminology) codes for the services provided. For example, linking M51.26 to a CPT code for physical therapy or an epidural injection justifies the medical necessity of that procedure.
Frequently Asked Questions (FAQ)
Here are answers to some common questions about M51.26.
Q1: Is M51.26 a serious condition?
A: For most people, no, it is not a “serious” condition in the sense of being life-threatening. It is a common spinal issue. However, it can be a source of significant pain and discomfort. With proper treatment, the prognosis is usually very good. The only time it becomes a medical emergency is in the very rare case of Cauda Equina Syndrome.
Q2: What is the difference between M51.26 and M51.27?
A: The difference is location. M51.26 refers to a disc disorder in the thoracolumbar region (where the mid-back meets the lower back). M51.27 refers to a disc disorder in the lumbosacral region (where the lower back meets the sacrum/tailbone). The lumbosacral area (often involving the L5-S1 disc) is the most common site for disc problems.
Q3: How long does it take to recover from this type of disc disorder?
A: Recovery times vary greatly from person to person. With conservative treatment like physical therapy, many people start to feel significant improvement within a few weeks. Full recovery, where you can return to all activities without pain, can take anywhere from a few months to over a year. Patience is key.
Q4: Can this condition heal on its own without surgery?
A: Yes, absolutely. The body has an incredible ability to heal. In many cases of disc herniation, the body will gradually reabsorb the protruding disc material over time. This is why conservative care and physical therapy are so effective—they support the body’s natural healing process.
Q5: Will I need surgery for M51.26?
A: Statistically, no. Only a small percentage of people with disc disorders ever require surgery. Surgery is typically reserved for cases where there is severe nerve compression causing muscle weakness, or when pain has not improved after trying multiple non-surgical treatments for an extended period.
Conclusion
Navigating a new diagnosis can feel overwhelming, but knowledge is a powerful tool. The ICD-10 code for M51.26 is simply a precise medical shorthand for a specific issue: a disc disorder at the thoracolumbar junction of your spine. It explains the “what” and the “where” of your condition.
Understanding this code helps you cut through the jargon. It empowers you to ask your doctor better questions, understand your treatment options, and actively participate in your own recovery. Whether you are a patient learning to manage your symptoms or a professional ensuring accurate records, knowing the story behind M51.26 turns a random string of characters into a clear path forward.
Additional Resources
For more reliable information on spinal health and disc disorders, we highly recommend visiting the official website of the American Academy of Orthopaedic Surgeons (AAOS) . They provide excellent, patient-friendly resources on a wide variety of musculoskeletal conditions.
-
Resource Link: OrthoInfo – Low Back Pain (While this covers low back pain broadly, it provides excellent context for understanding related disc issues.)
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional for diagnosis and treatment of any medical condition.
Author: [Your Name/Site Name]
Date: FEBRUARY 13, 2026





