In the modern healthcare landscape, the management of overweight and obesity has transcended mere aesthetic concern to become a central pillar of preventive and therapeutic medicine. Obesity is a complex, multifactorial, chronic disease associated with a staggering array of co-morbidities, from type 2 diabetes and cardiovascular disease to certain cancers and debilitating musculoskeletal disorders. As the clinical focus on weight management intensifies, so too does the administrative and financial infrastructure that supports it. At the heart of this infrastructure lies the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM)—a system that is far more than a simple catalog of codes. For providers specializing in weight management, endocrinology, bariatric surgery, and primary care, mastery of ICD-10 coding is not an optional clerical task; it is a critical competency that directly impacts patient care, practice viability, and the advancement of the field.
Accurate ICD-10 coding serves three paramount functions. First, it establishes medical necessity, providing the justified reason for a patient encounter, diagnostic test, or therapeutic procedure. Without the precise code that aligns with the documented clinical picture, claims for services like intensive behavioral therapy, pharmacotherapy management, or bariatric surgery are routinely denied. Second, it enables robust data analytics. Accurate coding allows for the tracking of disease prevalence, the evaluation of treatment outcomes, and the identification of population health trends. This data is invaluable for research, public health initiatives, and demonstrating the efficacy of weight management programs. Third, it facilitates effective care coordination. When a patient’s problem list accurately reflects their weight status and related conditions through standardized codes, all members of the care team—from the PCP to the cardiologist to the registered dietitian—share a clear, unified understanding of the patient’s health profile.
This comprehensive guide is designed to be an authoritative resource for healthcare providers, coders, and practice administrators. We will embark on a detailed journey through the ICD-10-CM coding system as it pertains to weight management, moving beyond basic definitions to explore the nuanced application of codes in real-world clinical scenarios. We will dissect the core categories for obesity, elucidate the mandatory use of Body Mass Index (BMI) codes, unravel the complexities of coding for co-morbidities, and demonstrate how to correctly use Z-codes for counseling and health status. Through detailed vignettes, we will illuminate common pitfalls and provide a roadmap for compliance. Our goal is to equip you with the knowledge to transform clinical documentation into precise, defensible, and reimbursable code assignments, thereby ensuring that your practice can sustainably deliver the high-quality care that patients struggling with weight-related issues need and deserve.
![A medical professional reviewing a patient’s chart, with a laptop showing an EHR system and a notepad with ICD-10 codes like E66.01 and Z68.41. This symbolizes the integration of clinical care and administrative coding.]
*(Image Caption: The integration of clinical documentation and precise ICD-10 coding is essential for effective weight management programs, impacting everything from treatment plans to insurance reimbursement.)*
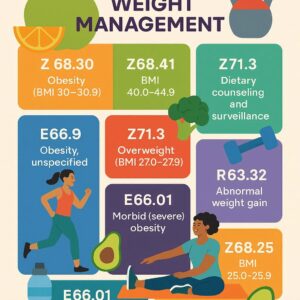
ICD-10 code for weight management
Chapter 1: Deconstructing the Foundation – The E66 Category for Obesity
The E66 category is the epicenter of ICD-10 coding for overweight and obesity. Unlike its predecessor in ICD-9, which offered limited specificity, ICD-10’s E66 category provides a more refined structure that demands detailed clinical documentation. It is crucial to understand that these codes describe the diagnosis of obesity itself, not just the circumstance of being overweight.
E66.0: Obesity due to Excess Calories
This is the most frequently used code for “simple” or “nutritional” obesity, where the primary etiology is a long-term imbalance between caloric intake and energy expenditure. The specificity required within this subcategory is a hallmark of ICD-10’s design.
-
E66.01: Morbid (Severe) Obesity due to Excess Calories: This code is a workhorse in bariatric medicine and advanced weight management clinics. The term “morbid obesity” is a specific clinical classification, typically defined as:
-
A Body Mass Index (BMI) of 40 kg/m² or greater, or
-
A BMI of 35 kg/m² or greater in the presence of at least one serious obesity-related co-morbidity (e.g., type 2 diabetes, severe sleep apnea, hypertension).
-
Clinical Implication: The use of E66.01 is often a gateway code for establishing medical necessity for surgical interventions (bariatric surgery) and for advanced pharmacotherapies. Documentation must explicitly state “morbid obesity” or “severe obesity,” and the BMI must be recorded to support it.
-
-
E66.09: Other Obesity due to Excess Calories: This code is used for cases of obesity that do not meet the criteria for “morbid.” This includes Class I (BMI 30-34.9) and Class II (BMI 35-39.9) obesity, where the cause is attributed primarily to caloric excess. If the provider’s documentation simply states “obesity” without specifying “morbid,” and the etiology is presumed or stated to be caloric, E66.09 is the appropriate default code.
E66.1: Drug-Induced Obesity
This code is essential for capturing iatrogenic weight gain, a common and frustrating side effect of many medications. Accurate use of this code informs the entire care team of a potentially modifiable cause of the patient’s weight issue.
-
Coding Instruction: An additional code from the T36-T50 categories (with fifth or sixth character 5) must be used to identify the causative drug. For example:
-
E66.1 + T38.0x5A (Adverse effect of glucocorticoids, initial encounter) for weight gain from prednisone.
-
E66.1 + T43.205A (Adverse effect of unspecified antidepressants, initial encounter) for weight gain from an SSRI.
-
-
Clinical Implication: Identifying drug-induced obesity can lead to a clinical intervention such as dose reduction, medication switching, or proactive management, making this a powerful code for quality patient care.
E66.2: Morbid (Severe) Obesity with Alveolar Hypoventilation
This code describes a specific and serious condition known as Obesity Hypoventilation Syndrome (OHS). It is distinct from obstructive sleep apnea, though they often coexist. OHS is defined by the combination of obesity (typically BMI >30), awake chronic hypercapnia (PaCO₂ >45 mmHg), and sleep-disordered breathing, in the absence of other causes of hypoventilation.
-
Clinical Implication: This is a high-acuity diagnosis with significant implications for patient management, often requiring non-invasive ventilation. Documentation must clearly support the diagnosis of alveolar hypoventilation or OHS. Do not use this code for obesity with simple sleep apnea; use E66.01 or E66.09 with G47.33 instead.
E66.3: Overweight
This code is used for individuals who are overweight but not obese. This is formally defined as a Body Mass Index (BMI) between 25.0 and 29.9 kg/m². It is a crucial code for preventive care encounters, as it identifies patients at risk of progressing to obesity and its related diseases.
E66.8: Other Obesity
This is a residual category for specified forms of obesity that do not fit the descriptions above. This could include, hypothetically, types of obesity linked to specific monogenic syndromes that are not elsewhere classified. In most routine clinical practice, this code is rarely used.
E66.9: Obesity, Unspecified
This code should be used as a last resort. It is reserved for situations where a provider documents “obesity” but gives no information regarding its severity (morbid vs. other) or its etiology. With the emphasis on specificity in modern healthcare, reliance on E66.9 can be a red flag for auditors and may lead to claim denials, especially for higher-level services. It is always best practice to query the provider for more specific documentation.
Chapter 2: The Quintessential Qualifier – The Role of Body Mass Index (BMI) Codes (Z68.-)
If the E66 codes provide the diagnosis, the BMI codes from the Z68 category provide the essential, objective metric that quantifies it. The use of BMI codes is not optional in high-quality weight management coding; it is a mandatory component that provides the numerical justification for the diagnostic label.
Documentation and Specificity
The Z68 category is highly detailed, with codes for nearly every whole number BMI from under 18.5 to over 70. The most clinically relevant ranges for weight management are:
-
Z68.1 – Z68.29: BMI 19.9 through 29.9 (Normal, Overweight)
-
Z68.3 – Z68.35: BMI 30.0 – 34.9 (Class I Obesity)
-
Z68.36 – Z68.39: BMI 35.0 – 39.9 (Class II Obesity)
-
Z68.4 – Z68.45: BMI 40.0 – 70.0 and over (Class III Obesity, also known as Morbid or Severe Obesity)
The Legal and Reimbursement Imperative of BMI Coding
The linkage between a diagnosis of E66.01 (Morbid Obesity) and a BMI code of Z68.41 (BMI 40.0-44.9) is a classic example of coding integrity. The BMI code acts as the objective proof for the subjective diagnosis. For bariatric surgery centers, this is non-negotiable. Payers require the BMI to be documented and coded to confirm that the patient meets the NIH and payer-specific criteria for surgery. Furthermore, for Evaluation and Management (E/M) services, the BMI is often a factor in scoring the complexity of data reviewed, contributing to a higher level of service.
Synergy Between Obesity Diagnosis Codes and BMI Codes
| Clinical Scenario | Provider Documentation | Primary Diagnosis Code | Mandatory Secondary Code | Rationale |
|---|---|---|---|---|
| Class III Obesity | “Morbid obesity due to excess calories. BMI calculated at 42.” | E66.01 (Morbid obesity due to excess calories) | Z68.41 (BMI 40.0-44.9) | The BMI code provides the quantitative evidence for the “morbid” designation. |
| Class I Obesity | “Obesity. Patient has a BMI of 32.” | E66.09 (Other obesity due to excess calories) | Z68.32 (BMI 32.0-32.9) | The diagnosis is obesity, but not specified as morbid. The BMI confirms Class I. |
| Overweight Status | “Patient is overweight, BMI 27. Here for dietary counseling.” | E66.3 (Overweight) | Z68.27 (BMI 27.0-27.9) | The BMI code is essential as the diagnosis is solely based on this metric. |
| Drug-Induced Weight Gain | “Significant weight gain, likely secondary to chronic olanzapine use. BMI is now 38.” | E66.1 (Drug-induced obesity) + T43.595A (Adv eff of antipsychotics) | Z68.38 (BMI 38.0-38.9) | The BMI code quantifies the severity of the drug-induced obesity. |
Chapter 3: Beyond the Scale – Coding for Co-morbidities and Related Conditions
Obesity is rarely an isolated problem. Its profound impact on multiple organ systems means that a comprehensive coding approach must encompass the entire clinical picture. Sequencing these codes correctly is vital for painting an accurate portrait of the patient’s health status and justifying comprehensive management plans.
Metabolic Syndrome (E88.81)
This code represents a cluster of conditions—including abdominal obesity, elevated blood pressure, insulin resistance, and dyslipidemia—that dramatically increase the risk of cardiovascular disease and diabetes. When a provider documents this diagnosis, it should be coded along with the individual components (e.g., I10, R73.09, E78.5). This code powerfully communicates the systemic nature of the patient’s risk.
Prediabetes (R73.03)
This is a critical code for preventive care. It identifies patients with impaired fasting glucose or impaired glucose tolerance who are at high risk for developing diabetes. In the context of a weight management visit, this code underscores the urgency of intervention.
Hypertension (I10)
Essential (primary) hypertension is one of the most common co-morbidities of obesity. While I10 is a simple code, its presence alongside an obesity code justifies more intensive monitoring, pharmacotherapy, and lifestyle counseling.
Dyslipidemia (E78.5)
This code for hyperlipidemia is essential for capturing the lipid abnormalities commonly seen in obesity. It supports the medical necessity for lipid panels and cholesterol-management medications.
Sleep Apnea (G47.33)
Obstructive Sleep Apnea (OSA) is intricately linked to obesity. Coding G47.33 alongside an obesity code is crucial, as treatment of OSA (e.g., with CPAP) is a vital part of the patient’s overall health management and can also be a prerequisite for bariatric surgery.
Fatty Liver Disease (K76.0)
This code is for non-alcoholic fatty liver disease (NAFLD), a condition where excess fat is stored in the liver. In its more severe form, it can progress to steatohepatitis (NASH) and cirrhosis. Its presence highlights a direct hepatic consequence of obesity.
Chapter 4: The Encounter’s Purpose – Distinguishing Between Z-Codes for Health Status and Counseling
Z-codes are used to classify factors influencing health status and contact with health services. They are not disease codes but are essential for explaining the reason for the encounter when no active disease is being treated.
Z68.-: Body Mass Index (BMI)
As discussed, this is a status code used to report the patient’s BMI. It is always secondary to a related diagnosis.
Z71.3: Dietary Counseling and Surveillance
This is a frequently used and often misunderstood code. It is used when the primary reason for the encounter is to receive dietary counseling. For example:
-
A patient with obesity sees a Registered Dietitian Nutritionist (RDN) for a dedicated appointment to create a meal plan.
-
A patient with prediabetes schedules a visit with their provider specifically for a “nutritional counseling session.”
-
Crucial Distinction: If a patient is seen for a problem (e.g., morbid obesity, hypertension) and dietary counseling is provided as an integral part of managing that problem, Z71.3 is not the primary code. The primary code should be the disease (E66.01, I10), and Z71.3 may be listed as a secondary code to indicate that counseling was provided, but it does not define the visit.
Z71.89: Other Specified Counseling
This is a catch-all for other types of counseling encounters. In weight management, this could be used for behavioral counseling sessions focused on physical activity, stress management, or sleep hygiene, where these are the sole focus of the visit.
Chapter 5: Clinical Vignettes – Applying ICD-10 Codes in Real-World Scenarios
Theory is best understood through practice. Let’s apply our knowledge to realistic patient encounters.
Vignette 1: Initial Consultation for Medical Weight Management
-
Scenario: A 45-year-old female presents to a weight management clinic for the first time. She has a history of progressive weight gain. Her BMI is 41. The physician documents: “Morbid obesity due to excess calories. Also has poorly controlled hypertension and is being evaluated for sleep apnea.”
-
Correct Coding:
-
E66.01 – Morbid (severe) obesity due to excess calories (The primary reason for the specialist consultation).
-
Z68.41 – Body mass index (BMI) 40.0-44.9 (Mandatory qualifier).
-
I10 – Essential (primary) hypertension (Active, relevant co-morbidity).
-
R06.81 – Apnea, not elsewhere classified (This is used for the “evaluation for” sleep apnea, as the diagnosis is not yet confirmed. Once a sleep study confirms OSA, this would be replaced with G47.33).
-
Vignette 2: Pre-operative Bariatric Surgery Consultation
-
Scenario: A 38-year-old male with a BMI of 44 is seen by a bariatric surgeon. He has a confirmed diagnosis of OSA on CPAP, type 2 diabetes, and hyperlipidemia. The visit is for surgical clearance and informed consent for a sleeve gastrectomy.
-
Correct Coding:
-
E66.01 – Morbid (severe) obesity due to excess calories (The underlying disease warranting surgery).
-
Z68.41 – Body mass index (BMI) 40.0-44.9 (Critical for proving surgical criteria).
-
E11.9 – Type 2 diabetes mellitus without complications (Major co-morbidity).
-
G47.33 – Obstructive sleep apnea (Confirmed and treated co-morbidity).
-
E78.5 – Hyperlipidemia (Additional co-morbidity).
-
Z01.811 – Encounter for pre-procedural respiratory examination (Explains the “clearance” aspect of the visit).
-
Z01.818 – Encounter for other pre-procedural examination (For the general surgical clearance).
-
Vignette 3: Routine Follow-up for Weight-Related Hypertension
-
Scenario: An established patient with obesity (BMI 36) and hypertension comes in for a blood pressure check. The note states: “Hypertension, stable on current meds. Obesity, discussed continued lifestyle modifications.”
-
Correct Coding:
-
I10 – Essential (primary) hypertension (This is the focus of the visit – the “blood pressure check”).
-
E66.09 – Other obesity due to excess calories (Not specified as morbid, but a chronic, active condition).
-
Z68.36 – Body mass index (BMI) 35.0-35.9 (Quantifies the obesity).
-
Chapter 6: Navigating the Pitfalls – Common Coding Errors and Compliance Risks
Avoiding these common errors can save a practice from costly denials and audits.
-
Error 1: Using an Outdated Obesity Code. ICD-10 has been mandatory since 2015. Using ICD-9 codes (e.g., 278.00 series) is a critical error.
-
Error 2: Omitting the BMI Code. Using E66.01 without a Z68.4- code is like diagnosing a fracture without an X-ray. It lacks the required objective support.
-
Error 3: Incorrect Code Sequencing. The primary diagnosis should always be the chief reason for the encounter. If a patient is seen for a hypertension follow-up, I10 should be first, even if obesity is a more significant overall problem. Sequencing E66.01 first in this case misrepresents the visit’s purpose.
-
Error 4: Misusing Z71.3. Using Z71.3 as the primary code for a visit where a disease (like obesity or diabetes) is managed and counseled is incorrect and will lead to down-coding or denial.
Chapter 7: The Future of Coding – A Glimpse into ICD-11 and Beyond
The World Health Organization (WHO) has already released ICD-11, which offers even greater specificity for obesity. It introduces codes for etiological types, such as:
-
6B00: Obesity due to heterogeneous mechanisms
-
5B81: Obesity due to melanocortin 4 receptor deficiency
-
5B80.0: Drug-induced obesity
While the US has not yet set a timeline for transitioning to ICD-11, its structure signals a future where coding will be even more integrated with the underlying pathophysiology of obesity, moving further away from a one-size-fits-all approach.
Conclusion
Mastering ICD-10 coding for weight management is a fundamental skill that bridges clinical practice and administrative excellence. Precision in using E66.- codes for diagnosis, Z68.- codes for BMI quantification, and appropriate codes for co-morbidities ensures accurate communication, validates medical necessity, and secures appropriate reimbursement. A disciplined approach to documentation and code selection, avoiding common pitfalls, is essential for maintaining compliance and supporting the financial health of a practice dedicated to treating this complex chronic disease. As the field evolves towards ICD-11, the principles of specificity and accuracy will only become more critical.
Frequently Asked Questions (FAQs)
1. What is the difference between E66.01 and E66.09?
E66.01 is specifically for “Morbid (Severe) Obesity,” which is clinically defined as a BMI of 40 or greater, or 35 or greater with serious co-morbidities. E66.09 is for “Other Obesity,” which covers Class I and Class II obesity (BMI 30-39.9) where the cause is excess calories and it is not specified as “morbid.”
2. When should I use a Z71.3 (Dietary Counseling) code as the primary diagnosis?
Only when the sole or primary reason for the patient’s encounter is to receive dietary counseling, and no active disease is being evaluated or managed during that visit. An example is a healthy patient with a BMI of 26 who schedules an appointment with a dietitian specifically for advice on healthy eating.
3. My EHR automatically calculates BMI. Do I still need to add a Z68 code?
Yes, absolutely. The automatic calculation is a tool for the clinician, but for coding, billing, and data tracking purposes, the specific Z68 code must be selected and submitted on the claim. The calculated BMI in the note supports the code selection.
4. A patient has a BMI of 41 but the provider only documents “obesity,” not “morbid obesity.” What code do I use?
You must use E66.09 (Other obesity). The term “morbid” is a specific clinical classification. Without that specific term in the documentation, you cannot assign E66.01, even if the BMI supports it. The best practice is to query the provider for clarification.
5. How do I code for a patient who has had bariatric surgery in the past and is now being seen for weight management?
You would use Z98.84 (Bariatric surgery status) to indicate their surgical history. Then, code any active conditions, such as E66.09 if they still have obesity, or Z68.- for their current BMI. If they are being seen for a nutritional deficiency post-surgery, you would code the deficiency (e.g., D64.9 for anemia) and E89.2 (Postprocedural malabsorption).
Additional Resources
-
Centers for Medicare & Medicaid Services (CMS) ICD-10-CM Official Guidelines for Coding and Reporting: https://www.cms.gov/medicare/coding/icd10 (The definitive source for coding rules).
-
American Medical Association (AMA) CPT® Network: (For procedural coding related to weight management services).
-
The Obesity Society (TOS): https://www.obesity.org/ (For clinical practice guidelines and updates).
-
American Academy of Professional Coders (AAPC): https://www.aapc.com/ (For ongoing coder education and certification).
-
CDC – About Adult BMI: https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html (For public health information on BMI).
Disclaimer: This article is intended for informational and educational purposes only. It is not a substitute for professional medical advice, coding consultation, or the clinical judgment of a qualified healthcare provider. Medical coding is complex and constantly evolving. Always consult the most current, official ICD-10-CM coding manuals, payer-specific guidelines, and your organization’s compliance officer for accurate code assignment. The author and publisher disclaim any liability arising directly or indirectly from the use of this information.
Date: November 03, 2025
Author: Dr. Evelyn Reed, MD, CCS-P





