Arthritis is often colloquially dismissed as simple joint pain, an inevitable nuisance of aging. However, for over 58 million adults in the United States alone, it is a complex, multifaceted, and often debilitating group of diseases that represents the leading cause of disability in the country. For healthcare providers, researchers, insurers, and health policymakers, accurately classifying and understanding this burden is paramount. This is where the intricate language of medical classification comes into play: the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). This system transforms a patient’s painful reality into a precise alphanumeric code, a critical data point that drives diagnosis, treatment, reimbursement, and population health analysis. This article serves as an exhaustive guide to mastering ICD-10 codes for arthritis. We will move beyond basic definitions into the nuanced layers of specificity required for accurate coding, exploring the clinical nuances of each major arthritis type and their direct translation into the ICD-10-CM framework. Whether you are a medical coder, a healthcare provider, a student, or a patient seeking to understand your medical records, this deep dive will illuminate the critical link between clinical medicine and administrative data.
ICD-10 Codes for Arthritis
2. Understanding the Foundation: What is the ICD-10-CM?
The ICD-10-CM is the official system for assigning codes to diagnoses and procedures in the United States. It is a morbidity classification published by the World Health Organization (WHO) and modified for use in the U.S. by the Centers for Disease Control and Prevention (CDC) and the National Center for Health Statistics (NCHS). Its primary purposes are:
-
Standardization: It provides a common language for reporting and monitoring diseases.
-
Reimbursement: It is fundamental to the medical billing process. Diagnoses codes are required for claims submission to insurers like Medicare and Medicaid.
-
Epidemiology and Research: It allows for the tracking of incidence and prevalence of diseases, helping to identify public health trends and allocate resources.
-
Quality Measurement: Codes are used to measure the quality, efficacy, and safety of patient care.
The structure of an ICD-10-CM code is hierarchical:
-
Chapter: Codes are grouped into chapters based on etiology or body system. Arthritis codes are primarily found in Chapter 13: Diseases of the Musculoskeletal System and Connective Tissue (M00-M99).
-
Category: The first three characters of a code define the general category of the disease (e.g., M19 for Other osteoarthritis).
-
Subcategory and Extension: Characters four through seven provide increasing specificity regarding anatomy, etiology, manifestation, and laterality (e.g., M19.011 for Primary osteoarthritis, right shoulder).
This hierarchical structure is what demands the high level of detail we will discuss throughout this article.
3. The Many Faces of Arthritis: A Clinical Overview
Before one can code arthritis, one must understand its clinical nature. “Arthritis” is not a single disease but an umbrella term for over 100 conditions that affect the joints and surrounding tissues.
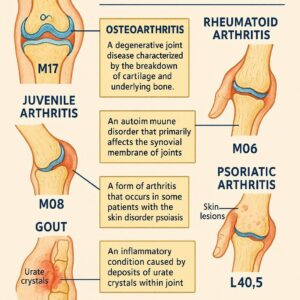
Osteoarthritis (OA): The “Wear-and-Tear” Arthritis
OA is the most common form, characterized by the breakdown of joint cartilage and the underlying bone. It is typically related to aging, injury, or obesity and most commonly affects weight-bearing joints like the hips and knees, as well as the hands and spine. Symptoms include pain, stiffness, and loss of flexibility. It is primarily a degenerative, non-systemic process.
Rheumatoid Arthritis (RA): The Systemic Assailant
RA is a chronic autoimmune disorder where the body’s immune system mistakenly attacks the synovium (the lining of the membranes that surround the joints). This causes painful inflammation, eventual joint deformity, and bone erosion. Unlike OA, RA is systemic, meaning it can affect other organ systems like the heart, lungs, eyes, and skin. It often presents symmetrically (e.g., in both wrists simultaneously).
Psoriatic Arthritis (PsA): Where Skin and Joints Collide
PsA is another autoimmune disease that occurs in some people with the skin condition psoriasis. It can affect any joint and is often characterized by “sausage-like” swelling of fingers and toes (dactylitis), nail changes, and enthesitis (inflammation where tendons/ligaments attach to bone). The pattern of joint involvement can vary greatly.
Gout and Crystal-Induced Arthropathies: The Agony of the Crystal
Gout is caused by the deposition of uric acid crystals in a joint, leading to sudden, severe attacks of pain, redness, and tenderness, often in the big toe. It is a metabolic disorder linked to uric acid levels in the blood. Other types, like pseudogout, are caused by calcium pyrophosphate crystals.
Juvenile Idiopathic Arthritis (JIA): Arthritis in the Young
JIA is an umbrella term for several types of arthritis that occur in children under the age of 16. It is characterized by persistent joint inflammation, and its various subtypes have different presentations and prognoses.
Other Forms: Spondyloarthritis, Lupus, and More
This category includes ankylosing spondylitis (which primarily affects the spine), arthritis associated with inflammatory bowel disease (enteropathic arthritis), and arthritis as a manifestation of systemic diseases like lupus (SLE).
4. Navigating the ICD-10-CM Chapter: Diseases of the Musculoskeletal System and Connective Tissue (M00-M99)
This chapter is the home for most arthritis codes. It is organized into blocks based on the type of disorder. The most relevant blocks for arthritis are:
-
M00-M02: Infectious arthropathies
-
M05-M14: Inflammatory polyarthropathies (This is where RA, PsA, and other systemic arthritides live)
-
M15-M19: Osteoarthritis (Polyosteoarthritis and OA of specific joints)
-
M20-M25: Other joint disorders
-
M30-M36: Systemic connective tissue disorders (e.g., SLE)
-
M45: Ankylosing spondylitis
Understanding this structure is the first step in finding the correct code.
5. Deep Dive: Coding Osteoarthritis (M15-M19)
Coding for OA requires extreme precision regarding the site, laterality, and whether it is primary or secondary.
M15: Polyosteoarthritis is used when OA affects multiple joints. This is a less common code.
M16: Osteoarthritis of hip
M17: Osteoarthritis of knee
M18: Osteoarthritis of first carpometacarpal joint (base of the thumb)
M19: Other and unspecified osteoarthritis (used for all other sites like shoulder, elbow, ankle, etc.)
Site and Laterality: The Core of Specificity
The fourth through seventh characters specify the exact joint and which side is affected.
-
Example 1:
M17.0is “Bilateral primary osteoarthritis of knee.” The “0” indicates both knees. -
Example 2:
M17.11is “Unilateral primary osteoarthritis, right knee.” The “11” specifies right knee. -
Example 3:
M19.011is “Primary osteoarthritis, right shoulder.” Here, the “01” specifies the shoulder joint, and the “1” specifies the right side.
Primary vs. Secondary: Knowing the Etiology
-
Primary (Idiopathic) OA: There is no known underlying cause. It is generally attributed to aging and “wear and tear.”
-
Secondary OA: The joint degeneration is a direct result of a known cause, such as a previous trauma, obesity, congenital deformity, or another disease.
-
Coding Secondary OA: You must use a code from the M19.0- (secondary osteoarthritis of other joints) or other specific site categories for secondary OA. Crucially, you must also code the underlying cause first. For example, if OA is due to old trauma, you would code the injury sequelae (e.g., S83.011A, Old tear of medial meniscus) first, followed by the secondary OA code (e.g., M23.21, Derangement of medial meniscus due to old tear).
-
Coding Scenarios and Examples
-
Scenario: A 68-year-old patient presents with long-standing pain in both knees. X-rays show significant joint space narrowing and osteophytes. The physician diagnoses “primary osteoarthritis of both knees.”
-
Code:
M17.0(Bilateral primary osteoarthritis of knee)
-
-
Scenario: A 55-year-old former construction worker has severe pain in his right shoulder. He has a history of a rotator cuff tear 10 years ago. The physician states the osteoarthritis is secondary to the old trauma.
-
Code 1:
S43.421A(Old tear of rotator cuff, right shoulder) *Note: The ‘A’ initial encounter is incorrect for an old injury; a sequelae code from the S43.4- category with a 7th character ‘S’ for sequela would be needed, but this illustrates the principle.* -
Code 2:
M19.211(Post-traumatic osteoarthritis, right shoulder)
-
6. Deep Dive: Coding Rheumatoid Arthritis (M05-M06)
RA coding is complex due to its systemic nature and the need to code for organ involvement.
M05: Seropositive rheumatoid arthritis (Rheumatoid Factor positive)
M06: Other rheumatoid arthritis (includes seronegative RA and other specific types like rheumatoid nodule)
The Rheumatoid Factor Distinction (Seropositive vs. Seronegative)
The physician’s documentation of the patient’s serological status (positive or negative for RF or anti-CCP antibodies) is critical.
-
M05.9– Seropositive RA, unspecified -
M06.0– Seronegative RA
Organ System Manifestations: The Critical “With”
The power of ICD-10-CM is its ability to show causality using combination codes. For RA, many codes include the arthropathy with the organ involvement.
-
Example:
M05.331is “Rheumatoid arthritis of right wrist with rheumatoid lung disease.” This single code tells the entire story. -
Other manifestations have their own specific codes:
-
M05.39-– RA with other organ systems involvement -
M05.2-– RA with vasculitis -
M06.3-– Rheumatoid nodule
-
If a specific combination code does not exist, you must code the RA and the manifestation separately.
Coding Scenarios and Examples
-
Scenario: A patient with known seropositive RA presents for a flare-up. The note states “RA with active synovitis in both hands and known rheumatoid lung disease.”
-
Code 1:
M05.341(RA of right hand with involvement of organs and systems) – but this requires laterality. If both hands are affected, you may need two codes or an unspecified code if the documentation isn’t specific. -
Code 2:
M05.342(RA of left hand with involvement of organs and systems) -
*Alternatively, if the lung disease is the focus, a code like M05.31- (RA of shoulder with organ involvement) might be used if the shoulder is affected, but the documentation must support it.* This scenario highlights the need for precise documentation.
-
-
Scenario: A patient is newly diagnosed with seronegative rheumatoid arthritis. No organ involvement is noted.
-
Code:
M06.09(Other specified rheumatoid arthritis, multiple sites) orM06.09(if unspecified site). The exact code depends on the sites documented.
-
7. Deep Dive: Coding Psoriatic Arthritis (M07) and Enteropathic Arthropathies (M09)
The codes under M07 are specifically for psoriatic arthropathy affecting various joints. The fourth and fifth characters define the site.
-
M07.60-– Psoriatic arthritis of unspecified site -
M07.61-– Psoriatic arthritis of shoulder -
M07.62-– Psoriatic arthritis of elbow -
…and so on for wrist, hand, hip, knee, ankle/foot, and other sites.
Coding Tip: You must also code the underlying psoriasis (L40.5-) separately. There is no combination code that includes both the skin and joint manifestation.
Enteropathic Arthropathies (M09) are arthritis associated with gastrointestinal diseases like Crohn’s (K50.-) or Ulcerative Colitis (K51.-). Code first the underlying GI disease, followed by the arthritis code from M09.
8. Deep Dive: Coding Gout (M10) and Other Crystal Arthropathies
Gouty Arthropathy vs. Gout Attack
This is a key distinction.
-
Gouty Arthropathy (M1A.-): These are codes for chronic gout. They have a 7th character to indicate stage (e.g., 0 – without tophus, 1 – with tophus).
-
Gout (M10.-): These are codes for the acute attacks.
Coding Drug-Induced and Secondary Gout
Gout can be caused by medications or other conditions that lead to high uric acid levels.
-
Idiopathic Gout:
M10.0-– Idiopathic gout -
Lead-induced Gout:
M10.1-– You must also code the toxic effect of lead (T56.0-). -
Drug-induced Gout:
M10.2-– You must also code the adverse effect of the drug (e.g., T50.0X5A for adverse effect of thiazide diuretics). -
Gout due to Renal Impairment:
M10.3-– You must also code the chronic kidney disease (N18.-).
9. Deep Dive: Coding Juvenile Idiopathic Arthritis (M08)
JIA codes are for patients under 16 years of age. The subtypes are critical:
-
M08.0– Unspecified juvenile rheumatoid arthritis -
M08.2– Juvenile rheumatoid arthritis with systemic onset (Still’s disease) -
M08.3– Juvenile rheumatoid polyarthritis (seronegative) -
M08.4– Pauciarticular juvenile rheumatoid arthritis
10. The Importance of Laterality and Specificity
The transition from ICD-9 to ICD-10 was a 14,000-code system to a 68,000-code system largely due to increased specificity. Using unspecified codes (which typically end in .9, like M19.90 – Unspecified osteoarthritis of unspecified site) is highly discouraged. It can lead to:
-
Claim Denials: Payers may see it as insufficient documentation for medical necessity.
-
Inaccurate Data: It muddies public health data, making it harder to track diseases in specific populations or joints.
-
Poor Patient Care: It fails to paint an accurate picture of the patient’s condition for other providers.
Always code to the highest level of specificity documented.
11. Documentation: The Physician’s Role in Accurate Coding
Accurate coding is impossible without precise clinical documentation. Coders can only code what they read. Physicians must document:
-
Type of Arthritis: e.g., “rheumatoid,” “osteo,” “psoriatic.”
-
Specific Joint(s) Affected: e.g., “left knee,” “proximal interphalangeal joints of both hands.”
-
Laterality: Clearly state “right,” “left,” or “bilateral.”
-
Etiology: Specify “primary,” “secondary,” “post-traumatic,” “idiopathic.”
-
Manifestations: For RA, note any associated organ involvement (e.g., “rheumatoid lung disease”).
-
Serological Status: For RA, note “seropositive” or “seronegative.”
-
Chronic vs. Acute: For gout, note “chronic tophaceous gout” or “acute gout attack.”
12. Common Coding Pitfalls and How to Avoid Them
| Pitfall | Example | How to Avoid It |
|---|---|---|
| Using Unspecified Codes | Using M19.90 for a patient with documented primary OA of the right knee. | Always review the record for site and laterality. Use M17.11. |
| Misunderstanding Laterality | Coding M17.12 (left knee) when the note says “right knee pain.” | Pay meticulous attention to the documented laterality. |
| Missing Underlying Cause | Coding secondary OA without coding the cause (e.g., old fracture, obesity). | Code first the underlying cause. Follow the ICD-10 guidelines for “Code also” and “Code first” notes. |
| Confusing Chronic and Acute Gout | Using a chronic code (M1A.-) for an acute flare-up. | Match the code to the encounter. Use M10.- for acute attacks. |
| Incorrectly Linking Manifestations | Not coding the associated psoriasis for psoriatic arthritis. | Remember that some conditions (like PsA and psoriasis) require two separate codes. |
13. Beyond the Code: The Impact of Accurate Arthritis Coding
Accurate coding is not just an administrative task. It has real-world consequences:
-
Patient Care: Correct codes ensure a patient’s medical history is accurately reflected, guiding future treatment decisions.
-
Research and Public Health: Accurate data allows researchers to identify trends, study the effectiveness of treatments, and understand the true prevalence of different arthritis types, guiding funding and resource allocation.
-
Reimbursement: Precise coding ensures healthcare providers are reimbursed fairly and appropriately for the complexity of care they provide, reducing claim denials and audits.
14. The Future: ICD-11 and Beyond
The WHO released ICD-11, which came into effect in January 2022. ICD-11 offers even more granularity and a modernized digital structure. While the U.S. has not yet set a timeline for transitioning to ICD-11-CM, it represents the future of classification. It includes more detailed codes for laterality and severity, and its electronic format allows for better data integration. Understanding the principles of specificity in ICD-10 is the perfect foundation for adapting to ICD-11.
15. Conclusion
Mastering ICD-10 coding for arthritis requires a dual understanding of clinical medicine and coding guidelines. It demands a meticulous eye for detail, from the specific joint and side affected to the underlying etiology and systemic manifestations. Moving beyond unspecified codes is not merely a billing requirement but a fundamental practice for ensuring quality patient care, advancing medical research, and maintaining the financial health of medical practices. As the landscape of medical classification evolves, the core principle remains unchanged: precise documentation is the bedrock of precise coding.
16. Frequently Asked Questions (FAQs)
Q1: What is the most common mistake in arthritis coding?
A: The most common mistake is using an unspecified code (e.g., M19.90) when the medical record contains enough information to use a more specific code that identifies the site and laterality. Always code to the highest level of detail provided.
Q2: How do I code a patient with multiple types of arthritis?
A: You code all conditions that are documented and relevant to the current encounter. The primary reason for the visit should be sequenced first. For example, a patient seen for a flare-up of rheumatoid arthritis who also has pre-existing osteoarthritis of the knee would have the RA code sequenced first, followed by the OA code.
Q3: What if the physician’s documentation is unclear or conflicting?
A: The coder cannot assume or interpret. If the documentation is unclear regarding laterality, type, or etiology, the physician must be queried for clarification. It is a crucial part of the coder’s role to ensure the documentation supports the codes being assigned.
Q4: When should I use a code from Chapter 13 (M00-M99) vs. a code from another chapter?
A: Use Chapter 13 for the arthritis itself. If the arthritis is a manifestation of a disease classified elsewhere (e.g., enteropathic arthritis from Crohn’s disease), you must “code first” the underlying disease from its respective chapter (e.g., Chapter 11 for digestive diseases), followed by the arthritis code from Chapter 13.
Q5: Are there codes for the severity or stage of arthritis?
A: ICD-10-CM does not have specific codes for severity stages like “mild,” “moderate,” or “severe.” However, for chronic gout (M1A), the 7th character indicates the presence of a tophus (tophus/i), which implies advanced disease. Severity is typically captured in the clinical notes and through other code systems like CPT for services rendered.
17. Additional Resources
-
The Official ICD-10-CM Guidelines: https://www.cms.gov/medicare/icd-10/2024-icd-10-cm (Updated annually; always use the current version).
-
Centers for Disease Control and Prevention (CDC) – ICD-10-CM: https://www.cdc.gov/nchs/icd/icd-10-cm.htm
-
American Academy of Professional Coders (AAPC): https://www.aapc.com/ (Offers training, certifications, and resources for medical coders).
-
American Health Information Management Association (AHIMA): https://www.ahima.org/ (Another leading authority on health information and coding).
-
Arthritis Foundation: https://www.arthritis.org/ (Provides excellent clinical information on all forms of arthritis for patient and professional education).
Date: September 19, 2025
Disclaimer: This article is intended for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or coding. The codes and guidelines referenced are subject to change. Always consult the most current, official ICD-10-CM coding manuals and guidelines for accurate coding and billing.





