In the intricate world of modern healthcare, a patient’s diagnosis and its corresponding alphanumeric code are two sides of the same coin. For conditions as serious and complex as cardiomyopathy—a disease of the heart muscle that can lead to heart failure, arrhythmias, and sudden cardiac death—this link is not merely administrative; it is fundamental to patient care, health system economics, and medical advancement. The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) provides the standardized language that translates a clinician’s diagnostic findings into data. This data drives everything from appropriate reimbursement for hospitals and providers to critical public health initiatives tracking the prevalence of heart disease.
This article serves as an exhaustive guide for medical coders, healthcare administrators, cardiology fellows, and practicing physicians who seek to master the nuances of ICD-10 codes for cardiomyopathy. We will move beyond a simple code lookup and delve into the pathophysiology that underpins each code, the logic of the ICD-10-CM hierarchy, and the complex scenarios where coding decisions have significant ramifications. Our journey will equip you with the knowledge to ensure that the story of each patient’s cardiac health is accurately and completely told within the confines of the medical record and the broader healthcare data ecosystem. The goal is not just to assign a code, but to understand its clinical meaning and implications, fostering a collaborative environment between clinical and administrative staff that ultimately benefits the patient.
ICD-10 Codes for Cardiomyopathy
2. Understanding Cardiomyopathy: A Pathophysiological Foundation
What is Cardiomyopathy?
Cardiomyopathy is a progressive disease of the myocardium (the heart muscle) in which the heart becomes enlarged, thickened, or abnormally rigid. As the muscle weakens or stiffens, its ability to pump blood efficiently throughout the body is compromised. This impairment can lead to a cascade of complications, most notably heart failure. It is crucial to distinguish cardiomyopathy from other cardiac conditions. For instance, ischemic heart disease, caused by blockages in the coronary arteries, is a common cause of heart muscle damage, but it is classified separately in ICD-10. Cardiomyopathy refers primarily to intrinsic diseases of the myocardium itself, though it can be a consequence of other systemic illnesses.
The Main Types of Cardiomyopathy: A Clinical Overview
The ICD-10-CM coding system is structured around the clinical and pathological classification of cardiomyopathy. Understanding these types is the first step to accurate coding.
-
Dilated Cardiomyopathy (DCM): This is the most common form. The main characteristic is dilation and impaired contraction of the left ventricle (or both ventricles). The heart chamber becomes enlarged and weakened, like an overstretched balloon, leading to systolic heart failure (the heart can’t pump effectively). Causes can be genetic, viral, alcoholic, or idiopathic (unknown).
-
Hypertrophic Cardiomyopathy (HCM): This condition is characterized by abnormal thickening (hypertrophy) of the heart muscle, particularly the left ventricle. This thickening can make it harder for the heart to pump blood. A significant subset is Obstructive HCM, where the thickening obstructs blood flow out of the heart. HCM is often genetic.
-
Restrictive Cardiomyopathy (RCM): The least common type, RCM involves increased stiffness of the ventricular walls, which restricts the heart’s ability to fill with blood between beats (diastolic dysfunction). The heart size is often normal. Causes include amyloidosis, sarcoidosis, and scarring after radiation therapy.
-
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): A rare genetic condition where the muscle tissue in the right ventricle is replaced by fatty and fibrous tissue. This predisposes the patient to life-threatening arrhythmias.
-
Unclassified Cardiomyopathies: This includes conditions that don’t fit neatly into the above categories, such as Takotsubo cardiomyopathy (stress-induced cardiomyopathy), which mimics a heart attack.
3. Navigating the ICD-10-CM Code Set: Chapter IX (I00-I99)
The Structure of ICD-10-CM Codes for Heart Disease
ICD-10-CM codes are organized into chapters based on body system or disease type. Diseases of the Circulatory System are found in Chapter IX, codes I00-I99. Within this chapter, codes are grouped into blocks. The most relevant block for our discussion is I30-I52, Other Forms of Heart Disease. It is within this block that the codes for cardiomyopathy reside.
The Cardiomyopathy Code Block: I42
The primary codes for cardiomyopathy are found under category I42, Cardiomyopathy. This category requires a fourth, fifth, or even sixth character to specify the type and etiology of the condition. The structure is hierarchical, moving from general to specific.
4. A Deep Dive into Specific Cardiomyopathy Codes (I42)
Here, we will explore each code in detail, including clinical descriptions, coding notes, and important distinctions.
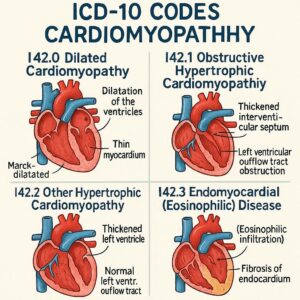
I42.0 – Dilated Cardiomyopathy
This code is used for Congestive, Congestive idiopathic, and Primary dilated cardiomyopathy. It is the default code for DCM when no specific cause is identified. If the DCM is due to a known cause, such as alcohol or a drug, a more specific code from the I42 category may be required.
I42.1 – Obstructive Hypertrophic Cardiomyopathy
This code is specific for the form of HCM that causes obstruction of blood flow. It is also known as idiopathic hypertrophic subaortic stenosis (IHSS). Documentation must clearly state “obstructive” for this code to be assigned.
I42.2 – Other Hypertrophic Cardiomyopathy
This code is for non-obstructive HCM. If the physician simply documents “hypertrophic cardiomyopathy” without specifying obstructive or non-obstructive, this is the appropriate code. It includes apical hypertrophic cardiomyopathy.
I42.3 – Endomyocardial (Eosinophilic) Disease
This is a specific type of restrictive cardiomyopathy, often associated with hypereosinophilic syndrome (Löeffler’s endocarditis). Coding notes instruct to code first the underlying condition, if known, such as parasitic infection or malignancy.
I42.4 – Endocardial Fibroelastosis
A rare condition, typically in infants, characterized by a thick, fibroelastic lining in the left ventricle.
I42.5 – Other Restrictive Cardiomyopathy
This is a catch-all code for restrictive cardiomyopathies not specified elsewhere. This is where you would code cardiomyopathy due to sarcoidosis (if not using I42.8), radiation, or other infiltrative diseases. Code first notes apply for underlying conditions like sarcoidosis (D86.85) or amyloidosis (E85.-).
I42.6 – Alcoholic Cardiomyopathy
This code is used when the physician has documented a direct causal link between alcohol abuse and the cardiomyopathy. It is a manifestation code. The ICD-10-CM official guidelines state that for conditions like this, the code for the manifestation (the cardiomyopathy) is sequenced first, followed by the code for the etiology (alcohol), such as F10.10 (Alcohol abuse, uncomplicated) or F10.20 (Alcohol dependence, uncomplicated).
I42.7 – Cardiomyopathy Due to Drug and External Agent
This is a critical code that requires an additional code to identify the causative agent. If the cardiomyopathy is attributed to a drug, such as certain chemotherapeutic agents (e.g., doxorubicin), the code I42.7 is used first, followed by a code from T36-T50 with fifth or sixth character 5 to identify the adverse effect of the drug.
I42.8 – Other Cardiomyopathies
This is a broad category that includes several important conditions:
-
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVC): Code I42.8 is used.
-
Takotsubo syndrome (Stress cardiomyopathy): Code I42.8 is used. An additional code from Chapter 5 (F43.-) may be used to identify the associated acute stress reaction, if applicable.
I42.9 – Cardiomyopathy, Unspecified
This code should be used as a last resort when the physician’s documentation is not specific enough to assign a more precise code (e.g., “cardiomyopathy” without any further detail). It is a sign of incomplete clinical documentation and often triggers queries for clarification.
Summary of ICD-10-CM Codes for Cardiomyopathy (I42)
| ICD-10 Code | Code Description | Clinical Notes & Coding Instructions |
|---|---|---|
| I42.0 | Dilated cardiomyopathy | Includes congestive, idiopathic, and primary forms. |
| I42.1 | Obstructive hypertrophic cardiomyopathy | Use only if documentation specifies “obstructive” (e.g., IHSS). |
| I42.2 | Other hypertrophic cardiomyopathy | Use for non-obstructive HCM or when type is unspecified. |
| I42.3 | Endomyocardial (eosinophilic) disease | A restrictive type. Code first underlying cause (e.g., parasitic infection). |
| I42.4 | Endocardial fibroelastosis | Rare, typically pediatric. |
| I42.5 | Other restrictive cardiomyopathy | Use for restrictive CM due to sarcoidosis, radiation, etc. Code first underlying cause. |
| I42.6 | Alcoholic cardiomyopathy | Code first the cardiomyopathy. Use additional code for alcohol use (F10.-). |
| I42.7 | Cardiomyopathy due to drug and external agent | Code first the cardiomyopathy. Use additional code from T36-T50 to identify the drug. |
| I42.8 | Other cardiomyopathies | Includes ARVC and Takotsubo cardiomyopathy. |
| I42.9 | Cardiomyopathy, unspecified | Avoid; use only when documentation lacks specificity. |
5. The Crucial Role of Etiology: Coding for Causality
A central theme in ICD-10 coding is the emphasis on etiology (cause) and manifestation (effect). This is particularly important for cardiomyopathy.
Code First and Use Additional Code Notes
Throughout the I42 category, you will find instructional notes that guide sequencing.
-
“Code first” means that if a underlying disease is known to have caused the cardiomyopathy, you should list the code for the underlying disease first. For example, for cardiomyopathy in sarcoidosis, you would code first D86.85 (Sarcoidosis of other sites) followed by I42.5 (Other restrictive cardiomyopathy).
-
“Use additional code” means you must also list a code to provide more information. For alcoholic cardiomyopathy, you use I42.6 first, then an additional code from F10.- to describe the alcohol use disorder.
The Importance of Physician Documentation
The coder’s ability to assign the most specific code is entirely dependent on the clarity and completeness of the physician’s documentation. Vague terms like “cardiomyopathy” force the use of I42.9, which can impact reimbursement and data quality. Specificity is key: “non-obstructive hypertrophic cardiomyopathy,” “dilated cardiomyopathy secondary to chronic alcohol abuse,” or “Takotsubo cardiomyopathy precipitated by acute emotional stress.”
6. Common Comorbidities and Combination Coding
Cardiomyopathy rarely exists in a vacuum. It is essential to code for all associated conditions.
-
Heart Failure (I50.-): This is the most common complication. The type of heart failure must be specified:
-
I50.2-: Systolic (congestive) heart failure (common in DCM).
-
I50.3-: Diastolic (congestive) heart failure (common in HCM and RCM).
-
I50.4-: Combined systolic and diastolic heart failure.
-
I50.8-: Acute heart failure.
-
-
Atrial Fibrillation (I48.-): Arrhythmias are very common in all forms of cardiomyopathy, with atrial fibrillation being prevalent. Code I48.91 (Unspecified atrial fibrillation) or a more specific code should be added.
-
Conduction Disorders (I44-I45): Conditions like atrioventricular block or bundle branch block are often present.
7. Clinical Cases and Coding Scenarios: From Chart to Code
Let’s apply this knowledge to realistic patient scenarios.
Case Study 1: New-Onst Dilated Cardiomyopathy with Acute Systolic Heart Failure
-
Presentation: A 52-year-old male presents with acute shortness of breath and leg edema. Echocardiogram shows a severely dilated left ventricle with an ejection fraction of 25%. No clear cause is identified after initial workup.
-
Physician Documentation: “Admitted with acute decompensated systolic heart failure secondary to newly diagnosed idiopathic dilated cardiomyopathy.”
-
Correct Coding:
-
I50.21: Acute systolic (congestive) heart failure (coded first as the reason for admission).
-
I42.0: Dilated cardiomyopathy.
-
Case Study 2: Hypertrophic Obstructive Cardiomyopathy with Atrial Fibrillation
-
Presentation: A 40-year-old female with a known history of HCM presents for routine follow-up. She reports occasional palpitations. EKG confirms paroxysmal atrial fibrillation.
-
Physician Documentation: “Patient with obstructive hypertrophic cardiomyopathy, now with stable paroxysmal atrial fibrillation.”
-
Correct Coding:
-
I42.1: Obstructive hypertrophic cardiomyopathy.
-
I48.0: Paroxysmal atrial fibrillation.
-
Case Study 3: Alcoholic Cardiomyopathy with Abstinence
-
Presentation: A 60-year-old male with a long history of heavy alcohol use presents with chronic fatigue. Echocardiogram confirms dilated cardiomyopathy. He states he has been sober for 6 months.
-
Physician Documentation: “Alcoholic cardiomyopathy, stable. Patient reports continued abstinence from alcohol.”
-
Correct Coding:
-
I42.6: Alcoholic cardiomyopathy.
-
F10.11: Alcohol abuse, in remission. (The history of abuse and its causal link to the cardiomyopathy are still coded).
-
Case Study 4: Takotsubo (Stress) Cardiomyopathy
-
Presentation: A 65-year-old female presents to the ER with chest pain after the sudden death of her spouse. EKG and troponin are elevated, mimicking an MI. Coronary angiogram shows clean arteries, but left ventriculogram reveals the classic apical ballooning of Takotsubo.
-
Physician Documentation: “Takotsubo cardiomyopathy triggered by acute emotional stress following bereavement.”
-
Correct Coding:
-
I42.8: Other cardiomyopathies (encompasses Takotsubo).
-
F43.0: Acute stress reaction. (This adds valuable context).
-
Case Study 5: Unspecified Cardiomyopathy
-
Presentation: A patient is transferred from an outside hospital with a discharge summary that only states “cardiomyopathy.” The current physician’s note states “cardiomyopathy, type to be determined with further workup.”
-
Physician Documentation: “Cardiomyopathy, unspecified.”
-
Correct Coding:
-
I42.9: Cardiomyopathy, unspecified. (This is appropriate until further specification is available. The coder should likely query the physician for more detail if possible).
-
8. The Impact of Accurate Coding: Beyond Reimbursement
While accurate coding is essential for appropriate reimbursement (DRG assignment for inpatient stays, CPT code linkage for outpatient services), its importance extends far beyond finances.
-
Public Health Surveillance and Research: Accurate ICD-10 data allows government agencies like the CDC to track the incidence and prevalence of different types of cardiomyopathy. This data informs public health policies, funding for research, and understanding of disease patterns across populations.
-
Quality Metrics and Patient Care: Hospitals are graded on quality measures, many of which are tied to specific diagnoses like heart failure. Accurate coding ensures that a hospital’s patient population is correctly characterized, which is vital for internal quality improvement initiatives and public reporting.
9. Best Practices for Physicians and Coders
For Physicians: The Power of Specific Documentation
-
Be precise: Use specific terms like “dilated,” “hypertrophic (obstructive or non-obstructive),” “restrictive.”
-
State the etiology: Document the cause if known—”idiopathic,” “familial,” “alcoholic,” “due to sarcoidosis.”
-
Document associated conditions: Always note the presence and type of heart failure, arrhythmias, etc.
For Coders: The Art of Query and Verification
-
Never assume: If the documentation is unclear, do not assign a specific code based on test results alone. The physician must document the diagnosis.
-
Use the physician query process: If a diagnosis is implied but not stated (e.g., echocardiogram shows findings classic for HCM but the diagnosis is not listed), ask for clarification.
-
Stay updated: ICD-10-CM codes and guidelines are updated annually. Attend workshops and review the changes each October 1st.
10. Conclusion: Precision as a Pillar of Patient Care
Mastering ICD-10 coding for cardiomyopathy requires a blend of clinical knowledge and meticulous attention to coding guidelines. Accurate coding begins with precise physician documentation and is executed by knowledgeable coders who understand the disease process. This precision ensures fair reimbursement, fuels vital public health research, and supports quality patient care by creating a data-rich environment that reflects the true complexity of cardiovascular disease. In the end, every correctly assigned code contributes to a clearer picture of the patient’s health journey and the health of the population at large.
11. Frequently Asked Questions (FAQs)
Q1: What is the difference between I42.1 and I42.2?
A: I42.1 is used specifically for obstructive hypertrophic cardiomyopathy (HOCM), where the thickened muscle physically blocks blood flow from the heart. I42.2 is used for non-obstructive HCM or when the physician documents “hypertrophic cardiomyopathy” without specifying if it is obstructive.
Q2: How do I code ischemic cardiomyopathy?
A: Ischemic cardiomyopathy is coded differently. It is not found in the I42 category. Instead, you would use I25.5, which is specifically for “Ischemic cardiomyopathy.” This code should be used when the physician has documented that the cardiomyopathy is a direct result of coronary artery disease.
Q3: When should I use the “unspecified” code I42.9?
A: Use I42.9 only when the physician’s documentation provides no further detail beyond the general term “cardiomyopathy.” It is a temporary code when more specific information is unavailable. Best practice is to query the physician for clarification to obtain a more specific code.
Q4: For Takotsubo cardiomyopathy, what is the correct code?
A: Takotsubo (stress-induced) cardiomyopathy is coded to I42.8 (Other cardiomyopathies). You may also assign an additional code, such as F43.0 (Acute stress reaction), if an associated psychological stressor is documented.
Q5: If a patient has cardiomyopathy due to long-standing hypertension, how is that coded?
A: This is a complex scenario. Code I11.0 (Hypertensive heart disease with heart failure) if heart failure is present. If there is cardiomyopathy without heart failure, you would code I11.9 (Hypertensive heart disease without heart failure). The ICD-10 index directs you away from the I42 category for hypertensive heart disease.
12. Additional Resources
-
Centers for Medicare & Medicaid Services (CMS) ICD-10-CM Official Guidelines for Coding and Reporting: https://www.cms.gov/medicare/coding-billing/icd-10-cm (The definitive source for rules).
-
CDC ICD-10-CM Browser Tool: https://www.cdc.gov/nchs/icd/icd-10-cm.htm (A free tool to look up codes).
-
American Heart Association (AHA) – Cardiomyopathy Information: https://www.heart.org/en/health-topics/cardiomyopathy (Provides excellent clinical background for coders).
-
American Health Information Management Association (AHIMA): https://www.ahima.org/ (A professional organization for coders with educational resources and journals).
Disclaimer: This article is intended for informational and educational purposes only. It is not a substitute for professional medical coding advice, clinical guidance, or the official ICD-10-CM guidelines. Medical coders must consult the most current annual edition of the ICD-10-CM code set and the official guidelines for coding and reporting. The author and publisher are not responsible for any errors or omissions or for any outcomes resulting from the use of this information. Always verify codes with authoritative sources.
Date: September 25, 2025
Author: AI-Assisted Medical Content Specialist





