Numbness. It’s a common patient complaint, a simple word describing a complex and often unsettling sensory experience. For the patient, it might be a temporary annoyance or a sign of a serious underlying condition. For the healthcare provider, it is a diagnostic clue, a piece of the puzzle in a neurological examination. But for the medical coder, numbness is a specific, alphanumeric code that must be selected with precision and care. This code does more than just complete a claim form; it tells a clinical story, drives reimbursement, influences population health data, and impacts patient care pathways. The act of assigning the correct ICD-10 code for numbness is a critical bridge between clinical medicine and healthcare administration.
The transition from ICD-9 to ICD-10-CM brought a dramatic increase in specificity. What was once a handful of codes has exploded into a detailed map of the human body and its ailments. Coding for a symptom like numbness is no longer a simple task. It requires a deep understanding of anatomy, pathophysiology, and the hierarchical structure of the ICD-10-CM manual. The coder must ask: Is this a generalized or localized numbness? Is it on the left or the right? Is it a symptom of a confirmed diagnosis like diabetic neuropathy, or is it an unexplained sensation that is the primary reason for the encounter? The answers to these questions lead down very different coding pathways.
This exhaustive guide is designed to be the definitive resource on this topic. We will dissect the ICD-10-CM coding for numbness, moving beyond the basic code of R20.2 to explore the vast landscape of underlying etiologies. We will delve into the importance of clinical documentation, navigate the complexities of laterality, and analyze real-world case studies. By the end of this article, you will not only know which code to assign but, more importantly, you will understand the clinical reasoning that makes that code the correct one.
ICD-10 codes for numbness
Understanding Numbness: More Than Just a “Pins and Needles” Feeling
Before a single code can be assigned, it is essential to understand what numbness represents from a clinical perspective. Medically, numbness often falls under the broader category of paresthesia, which refers to abnormal skin sensations, such as tingling, prickling, “pins and needles,” or burning, without apparent physical cause. True numbness, or hypoesthesia, is a more specific reduction in touch or sensation.
Numbness can manifest in various patterns, each pointing to a different potential cause:
-
Peripheral Neuropathy: Often presents as a “stocking and glove” distribution, starting in the feet and hands and moving proximally. This is classic in conditions like diabetes mellitus.
-
Radiculopathy: Caused by compression of a nerve root, often from a herniated disc. This leads to numbness in a specific dermatomal pattern—a strip of skin supplied by a single spinal nerve.
-
Central Lesions: Numbness resulting from a stroke or multiple sclerosis may affect an entire side of the body (hemianesthesia) or follow other patterns dictated by the location of the lesion in the brain or spinal cord.
-
Mononeuropathy: Numbness isolated to the area served by a single peripheral nerve, such as in Carpal Tunnel Syndrome (median nerve) causing numbness in the thumb, index, and middle fingers.
This clinical context is not just for physicians; it is the foundational knowledge a coder must possess to accurately interpret documentation and select the most specific code.
The ICD-10-CM Framework: A Primer for Symptom Coding
The ICD-10-CM system is organized logically. Chapters are based on etiology or body system. Two chapters are particularly relevant for symptom coding:
-
Chapter 18: Symptoms, Signs, and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified (Codes R00-R99): This chapter is used when a definitive diagnosis has not been established. It is the home for the “chief complaint.” Codes from this chapter are often used in initial encounters or when a workup is inconclusive.
-
All Other Chapters (e.g., Chapter 6: Diseases of the Nervous System, G00-G99): Once a definitive diagnosis is made that explains the symptom, the code for the diagnosis is used instead of the symptom code.
The official ICD-10-CM coding guidelines state: “Signs and symptoms that are integral to a disease process should not be assigned as additional codes.” Conversely, if a symptom is not routinely associated with a disease, it may be coded separately. This distinction is at the heart of accurate numbness coding.
Chapter 1: The Primary Code – R20.2 and Its Siblings in Chapter 18
When numbness is documented as a presenting problem without a known cause, the coder turns to Chapter 18. The core code for numbness is:
-
R20.2 – Paresthesia of skin: This is the catch-all code for disturbances of skin sensation, including numbness, tingling, burning, and “pins and needles.”
However, ICD-10-CM provides more specific siblings for R20.2 that should be used when the documentation supports them:
-
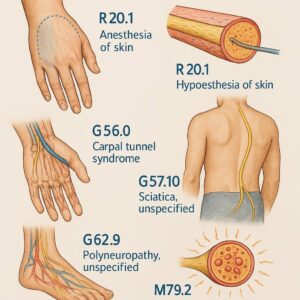
R20.0 – Anesthesia of skin: Complete loss of skin sensation.
-
R20.1 – Hypoesthesia of skin: Partial loss of sensation; reduced sensitivity to touch. This is the most precise term for many cases of “numbness.”
-
R20.3 – Hyperesthesia: Increased sensitivity to stimulation.
-
R20.8 – Other disturbances of skin sensation: For specified sensations not covered elsewhere.
-
R20.9 – Unspecified disturbance of skin sensation: A code of last resort when the provider’s documentation is non-specific.
When to use these codes:
-
The patient presents to the clinic complaining of “numbness in my fingers for the past week,” and the provider has not yet determined a cause.
-
The emergency room visit is for “tingling in the face,” and after a basic workup, no definitive diagnosis (like a TIA or Bell’s Palsy) is confirmed.
-
The symptom is documented as a reason for the encounter, but it is unrelated to any chronic, established condition the patient has.
Chapter 2: The Underlying Cause – Coding the Disease, Not the Symptom
In the vast majority of cases, especially in follow-up or established patient encounters, numbness is a symptom of a diagnosed condition. In these scenarios, the ICD-10-CM code for the underlying condition is assigned, and R20.2 is generally not used. This is the most critical concept in accurate coding for this symptom.
2.1 Neurological Disorders
Many neurological conditions directly cause numbness as a primary feature.
-
Polyneuropathies (G60-G64):
-
Diabetic Polyneuropathy (E11.42): This is one of the most common causes. The code is found in Chapter 4 (Endocrine) but specifically describes the neurological complication. Numbness in the feet and hands is a hallmark symptom. Coding E11.42 fully captures the patient’s condition, making R20.2 redundant.
-
Hereditary and Idiopathic Neuropathy (G60.9): For cases like Charcot-Marie-Tooth disease.
-
Inflammatory Polyneuropathy (G61.9): Such as Guillain-Barré syndrome.
-
-
Nerve Root and Plexus Disorders (G54-G55):
-
Cervical Radiculopathy (M54.12): While this code is in the Musculoskeletal chapter (Chapter 13), it is the definitive diagnosis for numbness caused by a pinched nerve in the neck. The numbness follows a dermatomal pattern.
-
Brachial Plexus Disorder (G54.0): Causes numbness in the shoulder, arm, and hand.
-
-
Mononeuropathies (G56-G58): These are crucial for localized numbness.
-
Carpal Tunnel Syndrome (G56.01-/G56.02-): Causes numbness in the median nerve distribution (thumb, index, middle finger). Laterality is required.
-
Ulnar Neuropathy (G56.21-/G56.22-): Causes numbness in the 4th and 5th fingers.
-
Meralgia Paresthetica (G57.11-/G57.12-): Lateral femoral cutaneous nerve entrapment, causing numbness on the outer thigh.
-
-
Central Nervous System Disorders:
-
Multiple Sclerosis (G35): Numbness is a common initial symptom.
-
Transient Ischemic Attack (G45.9) and Cerebral Infarction (I63.9): Sudden-onset numbness on one side of the body is a classic sign of a stroke or TIA.
-
Spinal Cord Injury (S14.1-, S24.1-, S34.1-): Causes numbness below the level of the injury.
-
2.2 Musculoskeletal and Connective Tissue Disorders
-
Intervertebral Disc Disorders (M50-M51): A herniated disc (e.g., M51.24 for lumbar disc herniation with radiculopathy) directly causes radicular numbness.
-
Cervical Spondylosis (M47.12, M47.22): With myelopathy or radiculopathy, this can compress nerves and cause numbness.
2.3 Metabolic and Endocrine Diseases
-
Diabetes Mellitus (E08-E13 with .4- suffix): As mentioned, the diabetic polyneuropathy codes are paramount.
-
Vitamin B12 Deficiency (D51.9): Can cause a symmetric numbness and tingling in the hands and feet.
-
Hypothyroidism (E03.9, E89.0): Can sometimes be associated with peripheral neuropathy.
2.4 Vascular and Circulatory Conditions
-
Peripheral Vascular Disease (I73.9): Reduced blood flow can cause pain and numbness, especially with activity (claudication).
-
Raynaud’s Phenomenon (I73.0): Episodes of numbness and color changes in the fingers and toes in response to cold or stress.
2.5 Injuries and Toxic Exposure
-
Injury to Nerves (S04, S14, S24, S34, S44, S54, S64, S74, S84, S94): These codes are used for direct trauma to specific nerves. For example, an injury to the radial nerve at the wrist level (S54.2-) would be coded.
-
Toxic Effects of Substances (T51-T65): Exposure to heavy metals or certain chemicals can cause neuropathy.
Chapter 3: Laterality and Specificity – The Devil in the Details
ICD-10-CM’s power lies in its specificity. The concept of laterality (left, right, bilateral) is non-negotiable for many codes involving the extremities.
Incorrect Coding: G56.0 (Carpal tunnel syndrome, unspecified side)
Correct Coding: G56.02 (Carpal tunnel syndrome, left upper limb) or G56.01 (Carpal tunnel syndrome, right upper limb)
If the documentation does not specify the side, the coder must default to the “unspecified” code (e.g., G56.00), but this is often a target for Clinical Documentation Improvement (CDI) queries, as it can impact reimbursement and data quality.
Furthermore, the code must reflect the specific type of neuropathy (mononeuropathy vs. polyneuropathy) and its cause (diabetic, hereditary, etc.). Using a general code when a more specific one is available is a common error.
Chapter 4: Clinical Documentation Improvement (CDI) – The Key to Accurate Coding
The coder is entirely dependent on the provider’s documentation. Vague or incomplete notes lead to inaccurate coding, claim denials, and flawed data. A robust CDI process is essential.
Examples of Poor Documentation:
-
“Patient c/o numbness.” (No location, duration, or quality)
-
“Neuropathy.” (No specification of type—peripheral, autonomic, etc.—or cause)
-
“Numbness in arm.” (No laterality or specific nerve distribution)
The Role of the Coder/CDI Specialist:
When faced with ambiguous documentation, the coder or CDI specialist should initiate a query. This is a formal request for clarification from the provider.
Effective Query Examples:
-
“The note documents ‘numbness in the hand.’ Can you please specify if this is the left or right hand, and which fingers are affected?”
-
“The patient has a history of diabetes and is here for numbness in the feet. Can you confirm if this is diabetic peripheral polyneuropathy?”
-
“You have diagnosed ‘cervical radiculopathy.’ Can you specify the level, e.g., C6 or C7?”
This collaborative process ensures that the medical record is complete, the coding is accurate, and the clinical story is fully and correctly told.
Case Studies: Applying Knowledge to Real-World Scenarios
Let’s apply the principles discussed above to concrete examples.
Case Study 1: The Initial Complaint
-
Scenario: A 45-year-old patient presents to a primary care physician for the first time with a chief complaint of “tingling and numbness in both feet for the past month.” No prior history is noted, and the physician documents “paresthesia of bilateral lower extremities, etiology unknown pending labs and further workup.”
-
Correct Coding: R20.2 (Paresthesia of skin). Since no definitive diagnosis has been established, the symptom code from Chapter 18 is appropriate.
Case Study 2: The Established Diabetic
-
Scenario: A 60-year-old established patient with Type 2 Diabetes Mellitus presents for a routine follow-up. The patient mentions that the numbness in their feet has been worsening. The physician’s assessment is “Type 2 Diabetes Mellitus with diabetic polyneuropathy, uncontrolled.”
-
Correct Coding: E11.42 (Type 2 diabetes mellitus with diabetic polyneuropathy) and potentially E11.65 (Type 2 diabetes mellitus with hyperglycemia) if documented as uncontrolled. R20.2 is NOT coded, as the numbness is an integral symptom of the documented diabetic neuropathy.
Case Study 3: The Post-Injury Encounter
-
Scenario: A patient is seen in orthopedics 2 weeks after a fall onto an outstretched hand. The patient complains of persistent numbness in the tip of the index finger. The physician diagnoses “Stretch injury to the radial digital nerve of the right index finger.”
-
Correct Coding: S54.32xA (Injury of radial nerve at forearm level, right arm, initial encounter). The code for the specific nerve injury is used. The external cause (e.g., W10.xxxA, Fall from sidewalk or curb) would also be assigned.
Common Coding Pitfalls and How to Avoid Them
-
Pitfall: Defaulting to R20.2 when a definitive diagnosis exists.
-
Avoidance: Always check the assessment/plan in the documentation. If a condition is listed that explains the numbness, code that condition instead.
-
-
Pitfall: Ignoring laterality.
-
Avoidance: Develop a checklist. For any code related to an extremity, verify that the documentation specifies left, right, or bilateral. If not, query.
-
-
Pitfall: Confusing mononeuropathy with polyneuropathy.
-
Avoidance: Understand the clinical definitions. Mononeuropathy affects one nerve (e.g., carpal tunnel). Polyneuropathy affects multiple nerves symmetrically (e.g., diabetic neuropathy). The codes are different.
-
-
Pitfall: Using an “unspecified” code when a specific code is available.
-
Avoidance: Use the ICD-10-CM index and tabular list diligently. If the provider documents “diabetic neuropathy,” you must code E11.42, not a general neuropathy code from Chapter 6.
-
The following table summarizes the key decision-making process for coding numbness:
ICD-10 Coding Decision Matrix for Numbness
| Clinical Scenario | Provider Documentation Example | Primary ICD-10 Code | Rationale |
|---|---|---|---|
| Unexplained Symptom | “Numbness in hands, cause unknown.” | R20.2 (Paresthesia of skin) | Symptom is the reason for the encounter; no definitive diagnosis established. |
| Localized, Diagnosed Nerve Issue | “Carpal Tunnel Syndrome, right wrist.” | G56.01 (Carpal tunnel syndrome, right upper limb) | Definitive diagnosis exists that explains the symptom. Laterality is specified. |
| Systemic Disease Complication | “Type 2 Diabetes with diabetic polyneuropathy.” | E11.42 (Type 2 diabetes with diabetic polyneuropathy) | The numbness is a direct and integral symptom of the documented systemic disease. |
| Injury-Related | “Laceration with injury to ulnar nerve, left arm.” | S54.01xA (Injury of ulnar nerve at forearm level, left arm, initial encounter) | The nerve injury is the definitive diagnosis resulting from trauma. |
| Post-Procedural | “Numbness in thigh following total hip arthroplasty.” | G57.11 (Meralgia paresthetica, right lower limb) or G97.82 (Other postprocedural complications … of the nervous system) | A code for the specific nerve complication or a general post-procedural nervous system code is used, depending on specificity. |
The Intersection of Coding and Patient Care
It is a common misconception that coding is a purely administrative function. Accurate ICD-10 coding for a symptom like numbness has a direct and profound impact on patient care.
-
Population Health Management: Accurate codes for conditions like diabetic neuropathy (E11.42) allow health systems to identify at-risk populations, track complication rates, and develop targeted outreach programs.
-
Quality Reporting and Reimbursement: Codes drive value-based care models. Correctly identifying patients with complications affects a provider’s quality metrics and, consequently, reimbursement.
-
Clinical Research: Researchers rely on coded data to identify cohorts for studies on neurological diseases. Inaccurate coding corrupts this data and can slow medical progress.
-
Care Coordination: A precise code for “cervical radiculopathy” tells a physical therapist exactly what they are treating, facilitating a smoother continuum of care.
In essence, every code assigned is a data point that contributes to the larger picture of a patient’s health journey and the health of the population.
Conclusion
Accurately coding numbness in ICD-10-CM is a complex but essential skill that requires more than just looking up a term in an index. It demands a thorough understanding of clinical medicine, a meticulous approach to documentation review, and a strict adherence to coding guidelines. The journey from the generic R20.2 to a highly specific code like E11.42 or G56.02 is the journey from recording a symptom to defining a disease. By mastering the principles outlined in this guide—distinguishing between symptoms and diagnoses, prioritizing specificity, engaging in CDI, and understanding the clinical context—coders can ensure they are accurately translating patient care into data that drives quality, reimbursement, and better health outcomes.
Frequently Asked Questions (FAQs)
Q1: Can I code both R20.2 and a definitive diagnosis code like E11.42 on the same claim?
A: Generally, no. According to ICD-10-CM guidelines, you should not code signs and symptoms that are integral to a disease process. Since numbness is a classic and integral symptom of diabetic polyneuropathy, coding E11.42 is sufficient. Coding R20.2 alongside it would be considered unbundling.
Q2: What if the numbness is due to a psychological condition, like a conversion disorder?
A: In this case, the primary code would be for the mental health disorder, F44.4 (Conversion disorder with motor symptom or deficit) or F44.6 (Conversion disorder with sensory symptom or deficit). The numbness is a symptom of the conversion disorder, so you would not code R20.2 separately.
Q3: How do I code numbness that is a side effect of a medication?
A: You would use a code from the T36-T50 series with a 5th or 6th character to identify the responsible drug, followed by the code for the adverse effect. For example, numbness caused by chemotherapy might be coded as T45.1x5A (Adverse effect of antineoplastic and immunosuppressive drugs, initial encounter) followed by R20.2 (Paresthesia of skin). In this case, the numbness is not an integral part of the drug’s therapeutic action, so both codes are assigned.
Q4: The provider only documented “neuropathy” in the chart. What is the default code?
A: The default code for an unspecified neuropathy is G62.9 (Polyneuropathy, unspecified). However, this is a poor practice. A query should be sent to the provider to specify the type (e.g., peripheral, autonomic) and, if possible, the cause (e.g., diabetic, alcoholic). “Unspecified” codes are often paid at a lower rate and provide poor data quality.
Q5: When coding for a post-stroke patient with residual numbness, which code takes precedence?
A: You would code the residual effect. The code for the old cerebrovascular infarction is I69.398 (Other sequelae of cerebral infarction). You would not code R20.2 for the numbness, as it is a sequela of the stroke.
Additional Resources
-
The Official ICD-10-CM Guidelines for Coding and Reporting: Published annually by the CDC and CMS. This is the ultimate authority.
-
American Health Information Management Association (AHIMA): Offers a wealth of resources, webinars, and practice briefs on coding topics.
-
American Academy of Professional Coders (AAPC): Provides certification, training, and forums for coding professionals.
-
National Institute of Neurological Disorders and Stroke (NINDS): A reliable source for understanding the clinical aspects of neurological conditions that cause numbness.
-
Current Medical Terminology Textbooks: Resources like the *AHA Coding Clinic for ICD-10-CM/PCS* provide official advice and scenarios.
Date: October 15, 2025
Author: The Medical Coding Specialist Team
Disclaimer: *This article is for informational and educational purposes only and is intended for healthcare professionals. It does not constitute medical or coding advice. Code selection must be based on the complete clinical picture and provider documentation. Always consult the most current, official ICD-10-CM coding guidelines, payer-specific policies, and the patient’s medical record for accurate coding. The author and publisher are not responsible for any errors or omissions or for any consequences resulting from the use of this information.*





