If you are an occupational therapist (OT), you likely became an OT to help people regain their independence and find meaning in their daily lives. You probably did not choose this career because you were passionate about medical billing and diagnostic codes. Yet, here we are.
Let’s be honest: navigating the world of ICD-10 codes can sometimes feel like trying to read a map written in a language you only half-understand. You know it’s important, but it’s easy to get lost in the details. However, these seemingly random strings of numbers and letters are the keys that unlock reimbursement, justify your skilled interventions, and tell the full story of your patient’s journey.
This guide is designed to be your friendly, reliable companion through the world of ICD-10 codes. We will walk through the most common categories you will encounter, discuss how to code ethically and accurately, and help you avoid the pitfalls that lead to denied claims.
Think of this not as a boring textbook chapter, but as a conversation. Let’s demystify coding together.
ICD-10 Codes for Occupational Therapists
Why Understanding ICD-10 Matters to Your Practice
Before we dive into specific codes, it is worth taking a moment to understand the “why.” Why does an OT need to be precise about a diagnosis code written by a physician?
The Gateway to Reimbursement
In the simplest terms, without a valid and appropriate ICD-10 code, your clinic does not get paid. Insurance companies use these codes to determine medical necessity. The code tells the payer why you provided the therapy. If the code doesn’t match the treatment you provided, or if it doesn’t justify the need for skilled intervention, the claim will be denied.
Telling the Patient’s Full Story
A diagnosis code is more than just a billing requirement. It is a piece of clinical shorthand. When you add “M17.11 (Unilateral primary osteoarthritis, right knee)” to your evaluation, you are providing a clear picture of the underlying cause of your patient’s difficulty getting in and out of the bathtub. It connects the “what” (the diagnosis) to the “why” (the functional limitation).
The “Specificity” Imperative
If there is one golden rule of ICD-10, it is this: be specific. Gone are the days of vague codes. ICD-10 demands detail. Which side of the body? Was it an initial encounter or a follow-up? Is this a chronic condition or an acute injury? This level of detail is not just bureaucratic busywork; it paints an accurate clinical picture and ensures proper payment.
Important Note: This guide provides an overview of common coding scenarios. It is not a substitute for official coding manuals or the clinical judgment of the diagnosing physician. Always code to the highest level of specificity based on the available documentation.
The Heavy Hitters: Most Common ICD-10 Categories for OTs
While OTs work with a vast array of conditions, certain diagnostic categories appear in our schedules more often than others. Let’s break down the most common families of codes you will encounter.
Neurological Conditions (G00-G99)
This is a major category for OTs, covering everything from strokes to Parkinson’s disease. These codes often describe the disease itself, while you will use additional codes to describe the specific manifestations like drooling, muscle spasticity, or gait problems.
-
G81.0- Flaccid hemiplegia: This refers to weakness on one side of the body without increased muscle tone.
-
G81.1- Spastic hemiplegia: This refers to weakness on one side of the body with increased muscle tone and stiffness.
-
G20 – Parkinson’s disease: A progressive movement disorder. You might pair this with codes for tremor, gait disturbance, or difficulty with activities of daily living (ADLs).
-
G35 – Multiple sclerosis (MS): An autoimmune disease affecting the brain and spinal cord.
-
G83.9 – Paralytic syndrome, unspecified: Used when a patient presents with paralysis but the specific type isn’t detailed.
Musculoskeletal Conditions (M00-M99)
This is likely the category you will use the most. It covers everything from arthritis to back pain. Pay close attention to laterality (left, right, bilateral) in this section.
-
M17.0 – Bilateral primary osteoarthritis of knee: A perfect example of a specific code.
-
M17.11 – Unilateral primary osteoarthritis, right knee: Note the specificity: unilateral, primary, right knee.
-
M54.2 – Cervicalgia: Neck pain.
-
M54.5 – Low back pain: A very common code, but try to use a more specific one if the diagnosis exists, such as M51.27 for a disc disorder.
-
M75.1 – Rotator cuff tear or rupture, not specified as traumatic: Often used in outpatient hand therapy.
-
S codes (Injury, poisoning and certain other consequences of external causes): These are used for acute injuries.
-
S06.5X1A – Traumatic subdural hemorrhage with loss of consciousness of 30 minutes or less, initial encounter: Notice the 7th character “A” for the initial encounter.
-
Mental and Behavioral Health (F01-F99)
OTs play a vital role in mental health, addressing the functional limitations caused by these conditions. Coding in this area must be handled with particular sensitivity and accuracy.
-
F32.9 – Major depressive disorder, single episode, unspecified: Used for a diagnosis of depression.
-
F41.9 – Anxiety disorder, unspecified: A common comorbidity with many physical conditions.
-
F84.0 – Autistic disorder: A core diagnostic category for pediatric OTs.
-
F90.9 – Attention-deficit hyperactivity disorder, unspecified type: Another frequent code in pediatric and even adult OT practices.
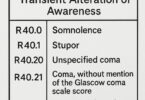
Symptoms, Signs, and Abnormal Findings (R00-R99)
These codes are used when a definitive diagnosis has not yet been made, but the patient presents with specific symptoms that require therapy. Remember, in many outpatient settings, a therapist cannot treat based solely on an “R” code for long; a definitive diagnosis is typically required after a certain number of visits.
-
R26.2 – Difficulty in walking, not elsewhere classified: A perfect functional code for a patient with gait instability.
-
R41.0 – Disorientation, unspecified: Useful for patients with confusion following a hospital stay.
-
R29.6 – Repeated falls: A critical code for OTs working in geriatrics or neuro rehab.
-
R63.3 – Feeding difficulties: A common code in both pediatric and geriatric settings.
Decoding the Code: A Quick Anatomy Lesson
ICD-10 codes are alphanumeric, and they are built for precision. Let’s look at a typical example:
M 17 . 11
-
Category: The first character is always a letter. Here, “M” denotes the “Diseases of the musculoskeletal system and connective tissue” chapter.
-
Classification: The first three characters (M17) represent the broader category. In this case, “Osteoarthritis of knee.”
-
Etiology, Anatomic Site, Severity: The characters after the decimal point provide the granular detail.
-
The fourth character (1) often specifies the type or site. In osteoarthritis, .1 often indicates primary, unilateral.
-
The fifth character (1) often specifies laterality. So, “1” equals right side.
-
Another common character you will see is the 7th Character. This is often used in injury (S and T) codes to indicate the episode of care.
-
A = Initial Encounter (active treatment)
-
D = Subsequent Encounter (routine care during healing)
-
S = Sequela (late effects or complications)
Common ICD-10 Codes for Occupational Therapists
To make this information more accessible, here is a table of some of the most frequently used codes across different practice settings.
| Diagnosis Description | ICD-10 Code | Practice Area | Key Specificity Note |
|---|---|---|---|
| Cerebral Infarction | I63.9 | Neuro / Geriatrics | Specify the type and artery if known. |
| Unilateral Primary OA, Right Hip | M16.11 | Outpatient / Geriatrics | Laterality is key here (1=Right, 2=Left). |
| Unilateral Primary OA, Left Hip | M16.12 | Outpatient / Geriatrics | Laterality is key here (1=Right, 2=Left). |
| Lumbar Spinal Stenosis | M48.06 | Outpatient / Geriatrics | The 6th digit specifies the site (lumbar). |
| Rotator Cuff Tear, Non-Traumatic | M75.10 | Hand Therapy / Outpatient | Different from an acute traumatic tear (S46.0-). |
| Difficulty in Walking | R26.2 | All Settings | A useful symptom code, but limited use time. |
| Autistic Disorder | F84.0 | Pediatrics | A core code for developmental delays. |
| Attention-Deficit Hyperactivity Disorder | F90.9 | Pediatrics / Adult MH | Use more specific codes if the type is known. |
| Major Depressive Disorder, Recurrent | F33.9 | Mental Health | Indicates an ongoing, episodic condition. |
| Alzheimer’s Disease, Unspecified | G30.9 | Geriatrics / Neuro | Often paired with dementia in ADL codes. |
| Encounter for Occupational Therapy | Z51.89 | All Settings | Note: This is an adjunct code, never a primary diagnosis. |
Mastering the Art of Code Selection
Knowing what the codes mean is half the battle. The other half is knowing how to select the right one in a real-world clinical scenario. This is where the skill comes in.
The “First-Listed” or Primary Diagnosis
The primary diagnosis is the main reason for the therapy services. It is the condition that is the focus of your treatment. In a perfect world, this is a definitive medical diagnosis like “G20 – Parkinson’s disease.”
However, what if a patient with Parkinson’s is seeing you specifically because they keep falling at night? You would still list G20 first, as it is the underlying condition causing the falls. You would then add a secondary code, like R29.6 (Repeated falls) , to capture the specific symptom you are addressing.
The Power of “With”
ICD-10 has a wonderful convention that allows you to link conditions. For example, a patient might have F02.80 (Dementia in other diseases classified elsewhere, without behavioral disturbance) . But if they are also aggressive, you would use F02.81 (…with behavioral disturbance) . This single code captures both the disease and the symptom.
Coding for Comorbidities
Your patient is more than just their primary diagnosis. They may have diabetes, high blood pressure, or obesity. While these may not be the reason for OT, they absolutely impact the plan of care. If a comorbidity affects your treatment approach—for example, if you need to monitor blood sugar during a session or adjust exercises for a patient with cardiac issues—it is clinically relevant and should be coded as a secondary diagnosis.
Common Pitfalls to Avoid
We all make mistakes, but some coding errors are more costly than others. Here are a few traps to watch out for:
-
Coding from a Suspected Diagnosis: Never code a condition that has not been formally diagnosed. You cannot code “probable Alzheimer’s.” You code the symptoms (like memory loss) until a definitive diagnosis is made.
-
Using Unspecified Codes Too Often: Codes ending in .9 or “unspecified” are sometimes necessary, but they should not be your default. They can trigger audits or lead to lower reimbursement because they don’t justify the medical necessity as strongly.
-
Ignoring Laterality: This is the most common “easy fix” error. If the diagnosis is for the left shoulder, make sure the code says left shoulder.
-
Mismatching Diagnosis and Treatment: This is a major red flag for auditors. If you are treating a patient for a right knee replacement, all your billed codes should reflect that. If your documentation talks about the left knee, you are inviting a denial.
Reader Tip: Create a cheat sheet. Print out a list of the top 50 codes you use in your specific setting. Laminate it and keep it at your desk. It will save you hours of searching over the course of a year.
Documentation: The Best Friend of Good Coding
You cannot have good coding without good documentation. The medical record must tell the same story as the claim form. Here is how your notes support your codes.
The “Double-Jointed” Note
Every note should link three key elements:
-
The Diagnosis: (e.g., S06.5X1A)
-
The Functional Limitation: (e.g., inability to dress self due to hemiparesis)
-
The Skilled Intervention: (e.g., therapeutic activity and caregiver training to teach one-handed dressing techniques)
If you document teaching one-handed dressing, and the diagnosis code is for a sprained ankle, an auditor will be confused. The diagnosis must support the need for the functional intervention, and the intervention must address the diagnosis.
Goal Writing and Coding
Your long-term goals should be a direct reflection of the diagnosis and the functional limitations. If the diagnosis is G81.9 (Hemiplegia) , and the limitation is R26.2 (Difficulty walking) , your goal should specifically target improving gait and safety.
“Patient will ambulate 150 feet with a standard walker and minimal assistance to access the bathroom independently, decreasing the risk of falls, within 4 weeks.”
This goal ties the diagnosis (hemiplegia causing weakness) to the symptom (difficulty walking) to the functional outcome (accessing the bathroom).
Practice Setting Deep Dives
Coding isn’t one-size-fits-all. Let’s look at how these principles apply in different OT settings.
In the Outpatient Clinic (Hand Therapy)
Here, precision is paramount. You are often dealing with specific anatomical structures.
-
Use the specific codes: For a trigger finger, use M65.30.
-
Capture the mechanism: Was it a work injury (Y93.h codes) or a repetitive strain?
-
Post-surgical codes: You will often use the aftercare codes (Z47.-) combined with the original condition code.
In Skilled Nursing Facilities (SNF) / Geriatrics
This setting is about complexity. Your patients often have a laundry list of diagnoses.
-
Prioritize the “Reason for Stay”: The primary diagnosis should be the condition most responsible for the patient receiving skilled therapy.
-
Capture the “Geriatric Syndromes”: Codes for weakness (M62.81), muscle wasting (M62.84), history of falls (Z91.81), and frailty (R54) are essential to justify the need for OT to maintain safety and function.
In Pediatrics (Early Intervention / School-Based)
This area has its own unique challenges, especially in a school setting where the “medical necessity” is tied to educational performance.
-
Developmental Delays: Use codes like F82 (Specific developmental disorder of motor function) .
-
Sensory Processing: While “Sensory Processing Disorder” is not a formal medical diagnosis in the ICD-10, you can use codes for related symptoms or associated diagnoses like autism (F84.0) or sensory issues in children (R48.8).
-
Collaboration with Physicians: Pediatric OTs often rely heavily on pediatricians to provide diagnostic codes that justify the therapy, as many “educational” diagnoses don’t translate directly to medical billing codes.
In Mental Health
-
Focus on Function: Your documentation must bridge the gap between the psychiatric diagnosis and the functional impairment. For example, a patient with F32.9 (Depression) may have a profound lack of motivation (avolition) that prevents them from performing basic hygiene tasks.
-
Coding the “Why”: Your note should explain that you are working on showering not just for cleanliness, but to establish a routine that combats the symptoms of depression.
The Future of OT Coding
The world of healthcare billing is constantly shifting. For OTs, the biggest recent change has been the increased scrutiny on “Medical Necessity.” Payers are demanding more and more proof that therapy is not just helpful, but medically necessary.
This means that simply documenting “Patient did 10 minutes of therapeutic exercise” is no longer enough. You must document why those 10 minutes are essential for this specific patient, based on their specific ICD-10 diagnosis.
Furthermore, the industry is moving toward value-based care. In this model, accurate coding is not just about getting paid for a single visit; it is about tracking outcomes and proving that your intervention, justified by the diagnosis, led to a meaningful improvement in the patient’s quality of life.
Your Coding Toolkit: Resources for Success
You don’t have to memorize the entire ICD-10 manual. Smart therapists use smart tools.
-
The Official ICD-10-CM Manual: Yes, it’s big and bulky. But it contains the official guidelines and notes that are essential for proper coding. It is the ultimate authority.
-
Coding Software/Apps: There are many excellent (and often free) apps and websites that allow you to search for codes by keyword. These are lifesavers for quick look-ups. Just ensure they are updated annually.
-
Superbills: A well-organized superbill customized to your clinic’s specialty can dramatically speed up the coding process.
-
Your Billing Specialist: Become friends with the person who does your billing. They are on the front lines of claim denials and know exactly which codes are getting rejected by specific insurance companies.
Conclusion
Mastering ICD-10 codes for occupational therapists is a journey, not a destination. It requires a blend of clinical knowledge, attention to detail, and a willingness to learn from your mistakes. By understanding the logic behind the codes, prioritizing specificity, and ensuring your documentation tells a complete and consistent story, you protect your practice, ensure fair reimbursement, and, most importantly, accurately represent the complex needs of the patients you serve. Remember that every code is an opportunity to advocate for your patient’s right to regain their independence.
Frequently Asked Questions (FAQ)
1. What is the difference between an ICD-10 code and a CPT code?
Think of it this way: the ICD-10 code is the “why” (the diagnosis, e.g., why does the patient need therapy?). The CPT code is the “what” (the treatment, e.g., what did you do during the session, like 97110 for therapeutic exercise). You need both on a claim form.
2. Can I use a patient’s symptoms as the primary diagnosis?
Yes, but with caution. If a definitive diagnosis hasn’t been established by a physician, you can use “R” codes for symptoms (like pain or difficulty walking). However, most insurance plans expect a definitive diagnosis code after a few visits to justify ongoing therapy.
3. What happens if I use the wrong ICD-10 code on a claim?
The most common outcome is that the claim is denied. You will then have to correct the code and resubmit the claim, which delays payment. In cases of a pattern of fraud or abuse, using incorrect codes can lead to audits, fines, or legal action.
4. How specific do I need to be with laterality (left vs. right)?
You must be as specific as the medical record allows. If the physician’s diagnosis specifies “left rotator cuff tear,” you must use the ICD-10 code for a left rotator cuff tear. If the record does not specify, you may have to use an unspecified code, but you should query the physician for more information.
5. What is a “Z” code, and when do I use it?
“Z” codes represent factors influencing health status or reasons for encounters that are not current diseases or injuries. For example, Z99.3 (Dependence on wheelchair) can be a useful secondary code. Z51.89 (Encounter for other specified aftercare) is sometimes used, but remember: it cannot be the primary reason for therapy.
Additional Resource
For the most up-to-date information, coding changes, and official guidelines, the only reliable source is the Centers for Medicare & Medicaid Services (CMS) website. You can download the official ICD-10-CM code sets and guidelines there.
Disclaimer
The information provided in this article is for general informational purposes only and does not constitute legal, billing, or medical advice. All coding scenarios must be based on the specific documentation in the patient’s medical record and the official coding guidelines. While we strive to keep the information accurate and up-to-date, coding rules and regulations are subject to change. You should always consult with a qualified billing specialist or refer to the official ICD-10-CM manual for definitive guidance.