Right upper quadrant (RUQ) pain is one of the most common clinical presentations in emergency departments, primary care offices, and gastroenterology practices worldwide. It is a symptom, a cry for help from the body, signaling a potential disturbance in a region densely packed with vital organs—the liver, gallbladder, bile ducts, duodenum, head of the pancreas, right kidney, and hepatic flexure of the colon. For the clinician, the challenge is diagnostic: to unravel the mystery of the pain’s origin. For the medical coder, the challenge is translational: to convert the clinician’s findings into a precise, alphanumeric language that the healthcare system understands—the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM).
This translation is not a mere administrative task; it is a critical function that reverberates throughout the healthcare ecosystem. An accurately assigned ICD-10 code for RUQ pain and its underlying cause directly influences patient care quality, drives appropriate reimbursement, fuels vital public health data, and supports clinical research. Using a generic or incorrect code can lead to claim denials, skewed health statistics, and an incomplete picture of the patient’s health journey. This article aims to be the definitive guide for medical coders, health information management professionals, and even clinicians seeking to understand the coding perspective. We will journey beyond the basic code R10.11, exploring its proper application, the crucial step of identifying the etiology, and the nuanced rules that govern accurate and compliant coding. We will dissect complex scenarios, clarify guidelines, and empower you to transform a simple symptom into a accurately coded clinical story.
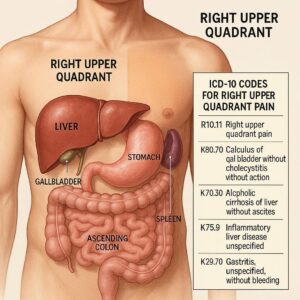
ICD-10 for Right Upper Quadrant Pain
Chapter 1: The Landscape of Abdominal Pain in ICD-10-CM
The ICD-10-CM chapter on “Symptoms, Signs, and Abnormal Clinical and Laboratory Findings” (Chapter 18) is where nonspecific complaints like pain are classified. Category R10, “Abdominal and pelvic pain,” is the home for these codes. It is essential to understand that codes within the R10 category are, by definition, symptom codes. They represent a problem that has not yet been, or cannot be, linked to a definitive diagnosis.
The structure of R10 is anatomically precise, a significant improvement from previous coding systems. This specificity allows for a more accurate reflection of the patient’s presentation.
-
R10.0 – Acute abdomen: This is a surgical emergency, describing severe, sudden-onset pain with signs of peritoneal inflammation (rigidity, guarding, rebound tenderness). It is not used for simple, localized pain.
-
R10.1 – Pain localized to upper abdomen: This is where our focus code resides.
-
R10.11 – Right upper quadrant pain
-
R10.12 – Left upper quadrant pain
-
R10.13 – Epigastric pain
-
-
R10.2 – Pelvic and perineal pain
-
R10.3 – Pain localized to other parts of lower abdomen: This includes right and left lower quadrant pain.
-
R10.8 – Other abdominal pain: A catch-all for dyspepsia, generalized pain, and other unspecified types.
This structured approach underscores a fundamental principle in modern medical coding: specificity is paramount. The days of using a generic “abdominal pain” code are over when the documentation allows for a more precise description.
Chapter 2: The Primary Code – R10.11: A Deep Dive
ICD-10-CM Code R10.11: Right upper quadrant pain is the cornerstone for coding this specific symptom. Its official definition is straightforward, but its application requires careful consideration.
When to Use R10.11:
This code is assigned when the physician’s documentation explicitly states “right upper quadrant pain,” “RUQ pain,” “pain in the right upper abdomen,” or similar phrasing that clearly localizes the discomfort to that anatomical region. It is the appropriate code for the initial encounter when the pain is the primary reason for the visit and a definitive diagnosis has not been established.
Clinical Context and Patient Presentation:
A patient presenting with R10.11 may describe a variety of sensations: a dull ache, a sharp, stabbing pain, or a colicky (cramping) pain. It may be constant or intermittent. It can radiate to the right scapula or shoulder (a classic sign of gallbladder disease) or be associated with intake of fatty foods. The coder does not diagnose, but understanding these associations helps in anticipating the linked diagnosis codes that may follow.
Limitations of R10.11:
It is critical to remember that R10.11 is a symptom code. Per the ICD-10-CM Official Guidelines for Coding and Reporting, “Codes for symptoms, signs, and ill-defined conditions from Chapter 18 are not to be used as a principal diagnosis when a related definitive diagnosis has been established.” This is the single most important rule governing the use of R10.11. Once the cause of the pain is identified, that etiological code takes precedence.
Chapter 3: Beyond the Symptom Code: The Imperative of Etiology
The real art and science of coding RUQ pain lies in moving from the “what” (the symptom) to the “why” (the cause). The symptom code R10.11 often acts as a placeholder until diagnostic workup—such as blood tests (LFTs, lipase, amylase), ultrasound, CT scans, or HIDA scans—reveals the underlying pathology.
The transition in coding mirrors the clinical diagnostic process:
-
Initial Encounter (Undiagnosed): The patient presents with RUQ pain. The physician documents the symptom and orders tests. The correct code is R10.11.
-
Follow-up/Confirmed Diagnosis Encounter: The ultrasound confirms acute cholecystitis. The reason for the encounter is now the treatment of acute cholecystitis. The principal diagnosis code becomes K81.0 (Acute cholecystitis), and R10.11 may be used as a secondary code if the pain is still being actively managed, though it is often redundant once the cause is known.
This process highlights that while R10.11 is essential, it is often a temporary code. The coder must be vigilant in reviewing the entire medical record to identify when a definitive diagnosis has been reached.
Chapter 4: Common Etiologies of RUQ Pain and Their Specific Codes
The right upper quadrant is a crossroads of multiple organ systems. A proficient coder must be familiar with the common conditions that cause pain here and their corresponding ICD-10-CM codes. The following table provides a structured overview.
Common Etiologies of Right Upper Quadrant Pain and Their ICD-10 Codes
| Organ System | Condition | ICD-10-CM Code | Clinical Notes & Coding Considerations |
|---|---|---|---|
| Hepatobiliary | Cholelithiasis (Gallstones) | K80.XX-series | Requires a 5th digit for type (e.g., K80.20 for calculus of gallbladder without cholecystitis). A 6th character may be needed for obstruction. |
| Acute Cholecystitis | K81.0 | Inflammation of the gallbladder. Often caused by an obstructing stone. | |
| Chronic Cholecystitis | K81.1 | Long-standing inflammation. | |
| Biliary Colic | K80.20 | Pain due to temporary cystic duct obstruction by a stone. | |
| Choledocholithiasis | K80.3-K80.5 | Stone in the common bile duct. Can cause obstruction and jaundice. | |
| Hepatitis (Alcoholic) | K70.XX | Liver inflammation. Code also for alcoholic dependence if applicable. | |
| Hepatitis (Viral) | B15-B19 | Specific codes for Hepatitis A, B, C, etc. | |
| Liver Abscess | K75.0 | ||
| Pancreatic | Acute Pancreatitis | K85.XX | Can be biliary, alcoholic, or idiopathic. A code from K85.0-K85.3 is used for the cause, and K85.8-K85.9 for other/unspecified causes. |
| Pancreatic Pseudocyst | K86.3 | A complication of pancreatitis. | |
| Gastrointestinal | Peptic Ulcer Disease | K25-K28 | Duodenal ulcers (K26) are a common cause of epigastric/RUQ pain. |
| Gastroesophageal Reflux Disease (GERD) | K21.0 | Can sometimes present with upper abdominal pain. | |
| Functional Dyspepsia | K30 | Diagnosis of exclusion for persistent pain/fullness. | |
| Renal | Nephrolithiasis (Kidney Stone) | N20.0 (Calculus of kidney) | Pain can radiate from the flank to the RUQ and groin. |
| Pyelonephritis (Kidney Infection) | N10 (Acute) / N11 (Chronic) | ||
| Pulmonary | Right Lower Lobe Pneumonia | J18.XX | Can cause referred pain to the abdomen, mimicking an abdominal condition. |
| Pulmonary Embolism | I26.XX | Can present with pleuritic chest/upper abdominal pain. | |
| Cardiac | Myocardial Ischemia/Infarction | I20-I21 | Especially involving the inferior wall, can present with epigastric/RUQ pain, nausea, and vomiting. |
| Other | Herpes Zoster (Shingles) | B02.XX | Before the rash appears, the pain can be localized and severe. |
| Abdominal Muscle Strain | S39.012A (Strain of muscle, fascia and tendon of abdomen, initial encounter) | Requires an external cause code from Chapter 20. |
4.1 Hepatobiliary System: The Gallbladder and Liver
The gallbladder is the most frequent offender in RUQ pain. Coding for gallstone disease (K80) is highly specific, accounting for the presence of cholecystitis and obstruction. For example, K80.44 (Acute cholecystitis with chronic cholecystitis with obstruction) tells a very specific clinical story. Liver conditions like hepatitis and abscesses are also coded here, with viral hepatitis falling under Chapter 1 (Infectious Diseases).
4.2 The Pancreas: A Deeper Source of Pain
Acute pancreatitis (K85) is a serious condition that often presents with severe epigastric pain that can radiate to the back and be perceived in the RUQ. The coding for pancreatitis has been expanded to allow for specification of the cause (e.g., K85.1 for biliary, K85.2 for alcoholic).
4.3 Gastrointestinal and Renal Causes
Duodenal ulcers (K26) are a classic cause of burning, epigastric/RUQ pain. Renal colic from a kidney stone (N20.0) typically causes flank pain, but as the stone moves, the pain can migrate anteriorly and downward, confusing the clinical picture.
4.4 Pulmonary and Cardiac “Masqueraders”
This is a critical area for coders. If a patient is admitted for RUQ pain, but the final diagnosis is right lower lobe pneumonia (J18.), the principal diagnosis must be pneumonia. Similarly, an inferior myocardial infarction (I21.4) can present with “indigestion” and upper abdominal pain. Coding this as a simple abdominal pain would be clinically and financially inaccurate. The coder must always be alert for these “zebras.”
Chapter 5: The Art of Sequencing: Primary Diagnosis, Co-diagnoses, and Manifestations
Sequencing—the order in which codes are listed—is governed by strict guidelines and directly impacts reimbursement via the Diagnosis-Related Group (DRG) system for inpatient claims.
-
Principal Diagnosis (Inpatient) / First-Listed Diagnosis (Outpatient): This is the condition established after study to be chiefly responsible for the admission or encounter.
-
Scenario: A patient is admitted for severe RUQ pain. After an ultrasound, they are diagnosed with acute cholecystitis and taken for a cholecystectomy.
-
Correct Sequencing: K81.0 (Acute cholecystitis) is the principal diagnosis. R10.11 (Right upper quadrant pain) may be listed as a secondary code, but it is often omitted as it is inherent to the cholecystitis.
-
-
Co-diagnoses and Co-morbidities (CCs/MCCs): These are other conditions that either exist at the time of admission or develop during the stay and affect patient management.
-
Scenario: The same patient with acute cholecystitis also has Type 2 Diabetes Mellitus (E11.9) which requires insulin sliding scale management during their stay.
-
Correct Sequencing: 1. K81.0, 2. E11.9. The diabetes is a co-morbidity that can impact the DRG and reimbursement.
-
-
Manifestations: Some conditions have underlying etologies with specific manifestations. In these cases, a “code first” note in the tabular list instructs the coder to sequence the underlying etiology first, followed by the manifestation.
-
Scenario: A patient has acute pancreatitis (K85.1) due to gallstones (K80.65).
-
Correct Sequencing: 1. K80.65, 2. K85.1. The gallstones are the underlying cause of the pancreatitis.
-
Chapter 6: Navigating the Official Coding Guidelines
The ICD-10-CM Official Guidelines for Coding and Reporting are the coder’s bible. Key rules relevant to RUQ pain include:
-
Section I.B.4 – Signs and Symptoms: “Codes that describe symptoms and signs are acceptable for reporting purposes when a related definitive diagnosis has not been established (confirmed) by the provider.”
-
Section II – Selection of Principal Diagnosis: The principal diagnosis is defined as “that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care.”
-
Section I.A.15 – Code Assignment and Clinical Criteria: “The assignment of a diagnosis code is based on the provider’s diagnostic statement that the condition exists. The provider’s statement that the patient has a particular condition is sufficient. Code assignment is not based on clinical criteria used by the provider to establish the diagnosis.”
This last point is crucial. Coders must code based on physician documentation, not their own interpretation of lab values or imaging reports.
Chapter 7: Clinical Documentation Improvement (CDI) – A Partnership for Accuracy
CDI is a proactive process where specialists (often nurses or coders) work with physicians to ensure the medical record accurately reflects the patient’s clinical status, treatments, and diagnoses. For RUQ pain, a CDI specialist might query the physician for clarification:
-
If the documentation states: “RUQ pain, likely biliary colic.”
-
Query: “Can the pain be further specified as ‘biliary colic’ or is it ‘unspecified abdominal pain’? Is there a confirmed diagnosis of cholelithiasis?”
-
-
If the documentation states: “Pancreatitis, likely due to ETOH.”
-
Query: “Can the acute pancreatitis be specified as alcoholic (K85.2) for greater coding specificity?”
-
These queries lead to more precise documentation, which in turn allows for more accurate coding, appropriate reimbursement, and better-quality data.
Chapter 8: Case Studies in Complexity – From Presentation to Final Code
Let’s apply our knowledge to realistic, complex scenarios.
Case Study 1: The Straightforward Gallbladder
-
Presentation: A 45-year-old female presents to the ED with sudden-onset, severe RUQ pain after a fatty meal. Pain radiates to her right scapula. Ultrasound shows gallstones and a thickened gallbladder wall with pericholecystic fluid.
-
Physician’s Final Diagnosis: Acute calculous cholecystitis.
-
Correct Coding: K80.00 (Calculus of gallbladder with acute cholecystitis without obstruction). R10.11 is not necessary as the pain is a defining symptom of the cholecystitis.
Case Study 2: The Cardiac Masquerader
-
Presentation: A 60-year-old male with a history of hypertension presents to his PCP with complaints of “severe indigestion” and RUQ discomfort, associated with nausea. He is referred for an abdominal ultrasound, which is normal. Due to persistent symptoms, an EKG is performed, showing ST-segment elevation in inferior leads. He is rushed to the Cath lab.
-
Final Diagnosis: Acute inferior wall myocardial infarction.
-
Correct Coding: I21.4 (Non-ST elevation myocardial infarction of inferior wall). The symptom code R10.11 would be incorrect as the principal diagnosis. The reason for the admission and treatment was the heart attack.
Case Study 3: The Multi-Factorial Admission
-
Presentation: An elderly patient with a history of Alzheimer’s disease is admitted from a nursing home with RUQ pain and confusion. Workup reveals acute cholecystitis and severe dehydration. The dehydration is aggressively treated alongside management of the cholecystitis.
-
Final Diagnoses: Acute cholecystitis, Dehydration, Alzheimer’s disease.
-
Correct Coding:
-
Principal Diagnosis: K81.0 (Acute cholecystitis) – the condition that occasioned the admission.
-
Secondary Diagnoses: E86.0 (Dehydration) – a co-morbidity that complicated care. F02.80 (Dementia in other diseases classified elsewhere without behavioral disturbance) – another pre-existing co-morbidity.
-
Conclusion: The Code as a Clinical Story
Accurate ICD-10 coding for right upper quadrant pain transcends mere data entry. It begins with the precise symptom code R10.11 but demands a diligent search for the underlying etiology. Mastering the codes for common causes like cholecystitis, pancreatitis, and hepatitis, while remaining vigilant for masqueraders like cardiac and pulmonary events, is essential. By adhering to official guidelines, understanding the critical importance of code sequencing, and embracing the principles of CDI, the medical coder transforms a patient’s complaint of discomfort into a precise, data-rich narrative that drives quality care and ensures the financial integrity of the healthcare system.
Frequently Asked Questions (FAQs)
Q1: Can I use R10.11 as the primary diagnosis for an inpatient admission if the cause of the pain is never found?
A1: Yes. If, after a full and complete workup, the physician cannot determine a definitive cause for the RUQ pain and documents it as “unspecified” or “idiopathic,” then R10.11 is an acceptable principal diagnosis for the admission.
Q2: How do I code a patient with chronic RUQ pain from a known condition, like chronic cholecystitis?
A2: The established, chronic condition (e.g., K81.1, Chronic cholecystitis) becomes the first-listed diagnosis for the encounter. The symptom code R10.11 is typically not added, as the pain is an inherent feature of the chronic condition.
Q3: What is the difference between K80.20 (Calculus of gallbladder without cholecystitis) and “biliary colic”?
A3: Clinically, they are often the same. “Biliary colic” is the clinical term for the pain caused by the temporary obstruction described by K80.20. If the physician documents “biliary colic,” K80.20 is the correct code.
Q4: When a patient has cholelithiasis but no pain, should I code R10.11?
A4: No. Asymptomatic gallstones are coded to K80.20. Symptom codes are only used when the symptom (pain) is present and documented.
Q5: Where can I find the most up-to-date ICD-10-CM guidelines and codes?
A5: The Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) are the official publishers of the ICD-10-CM. Their websites offer the complete set of guidelines and the code set for free download.
Additional Resources
-
Centers for Medicare & Medicaid Services (CMS) ICD-10 Page: https://www.cms.gov/medicare/coding/icd10 (Source for official guidelines and codes)
-
American Health Information Management Association (AHIMA): https://www.ahima.org/ (Provides education, certifications, and resources for coding professionals)
-
American Academy of Professional Coders (AAPC): https://www.aapc.com/ (Another leading organization for coder education and certification)
-
National Center for Health Statistics (NCHS) ICD-10-CM Page: https://www.cdc.gov/nchs/icd/icd-10-cm.htm (The official source for the code set)
-
ICD-10-CM Official Guidelines for Coding and Reporting FY 2025: (A mandatory document for every coder, available from the CMS and NCHS websites).
Disclaimer: This article is for informational purposes only and is intended for medical coders and healthcare professionals. It is not a substitute for the official ICD-10-CM guidelines, coding manuals, or professional medical advice. Always consult the most current official resources and physician documentation for accurate coding and billing. The author and publisher are not responsible for any errors or omissions or for any outcomes resulting from the use of this information.
Date: October 24, 2025
Author: Dr. Anya Sharma, MD, CCS-P





