If you’re researching medical codes, you’ve likely encountered the term “ICD-9 code for cervical spondylosis.” Whether you’re a medical coder reviewing old records, a patient deciphering a bill, or a student learning about diagnostic classification, understanding this specific code is more than just memorizing a number. It’s about grasping a system that shaped healthcare documentation for decades.
This guide will provide a deep, clear, and entirely original exploration of ICD-9 code 721.0—the code for cervical spondylosis. We’ll move beyond the basic definition to explore its structure, its role in patient care and billing, and crucially, why it’s now a part of medical history. Our goal is to make this technical topic accessible and valuable, turning a simple code into a story about the evolution of modern medicine.
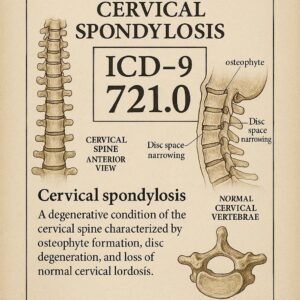
ICD-9 Code for Cervical Spondylosis
Understanding the Basics: What is Cervical Spondylosis?
Before we dive into codes, let’s establish what we’re classifying. Cervical spondylosis is not a single disease but an umbrella term.
In simple terms, cervical spondylosis refers to age-related wear and tear affecting the spinal disks in your neck. Think of it as the natural “aging” of your cervical spine. Over time, the discs that cushion the vertebrae dehydrate and shrink. Bones and ligaments can thicken, sometimes leading to bone spurs (osteophytes). This process can narrow the space for spinal nerves or the spinal cord itself.
Common symptoms include:
-
Neck pain and stiffness
-
Headaches, often originating at the back of the head
-
Tingling, numbness, or weakness in the arms, hands, or fingers
-
In more severe cases, loss of balance or coordination if the spinal cord is compressed
As Dr. Annette Carter, a retired orthopedic surgeon, notes: “Cervical spondylosis is almost a universal finding on imaging as we age. The key for clinicians is to distinguish between the normal radiographic signs of wear and the specific, symptomatic condition that requires intervention.”
This distinction—between a common imaging finding and a diagnosed condition—is precisely where accurate medical coding becomes critical.
The ICD-9 Coding System: A Foundational Framework
The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) was the diagnostic coding standard used in the United States from 1979 until October 1, 2015. Its primary purposes were:
-
Standardizing Diagnosis Reporting: Creating a common language for diseases and health conditions.
-
Enabling Epidemiology: Tracking the incidence and prevalence of diseases.
-
Supporting Billing and Reimbursement: Serving as the foundation for insurance claims and payment.
The system was hierarchical and numeric. Codes ranged from 3 to 5 digits, with greater specificity indicated by more digits.
Deconstructing Code 721.0: Cervical Spondylosis
The ICD-9-CM code for cervical spondylosis is 721.0. Let’s break down what each part signifies:
-
721: This is the parent category. In the ICD-9-CM index, 721 is “Spondylosis and allied disorders.” This broad category included various degenerative spinal conditions.
-
.0: This fourth digit provides the crucial specificity. The “.0” modifier pinpoints the location to the cervical region (the neck).
This structure highlights a key limitation of ICD-9: its general nature. Code 721.0 covered a wide spectrum of cervical degeneration without specifying:
-
The presence or absence of myelopathy (spinal cord compression) or radiculopathy (nerve root compression).
-
The exact level of the spine affected (e.g., C5-C6).
-
The severity of the condition.
Important Note for Readers: If you are dealing with a medical record or bill dated October 1, 2015, or later, the ICD-9 code 721.0 is no longer in active use. It has been replaced by a more detailed ICD-10-CM code. We will explore this critical transition in detail.
The Clinical and Administrative Role of Code 721.0
For over 35 years, this code was the essential link between a patient’s diagnosis and the healthcare system’s administrative engine.
In Clinical Documentation
Physicians used this diagnosis to succinctly communicate the reason for a patient’s visit, testing, or treatment. It summarized the clinical picture of neck degeneration in the patient’s chart.
In Medical Billing and Insurance
This is where the code became operational. Coders would translate the physician’s notes into the numeric code 721.0. This code was then placed on insurance claims (like the CMS-1500 form) to justify:
-
Office visits for evaluation and management of neck pain.
-
Diagnostic tests like cervical X-rays, CT scans, or MRIs.
-
Therapeutic procedures such as physical therapy, epidural steroid injections, or even spinal surgery.
Without this accurate code, claims could be delayed or denied, as the insurer would not see a medically necessary reason for the services provided.
The Transition from ICD-9 to ICD-10: A Necessary Evolution
On October 1, 2015, the U.S. healthcare system underwent a massive change, retiring ICD-9-CM and implementing ICD-10-CM. The transition was driven by the need for greater specificity, which improves patient care, public health tracking, and billing accuracy.
Why ICD-9 Code 721.0 Is Now Obsolete
The ICD-9 system was running out of space for new codes and lacked the clinical detail required for modern medicine. Code 721.0 was considered too “broad” or “unspecified” under the new standards.
The ICD-10-CM Equivalent: A New Level of Detail
In ICD-10-CM, cervical spondylosis is coded under category M47. The codes are alphanumeric and far more descriptive.
The direct, unspecified equivalent of 721.0 in ICD-10 is M47.812 – Spondylosis without myelopathy or radiculopathy, cervical region.
However, the power of ICD-10 is in its specificity. The code can now describe exactly what type of cervical spondylosis is present:
| ICD-9 Code (Historic) | ICD-10-CM Code (Current) | Description |
|---|---|---|
| 721.0 | M47.812 | Cervical spondylosis without myelopathy or radiculopathy |
| 721.0 | M47.22 | Other spondylosis with radiculopathy, cervical region |
| 721.0 | M47.12 | Other spondylosis with myelopathy, cervical region |
| 721.0 | M47.892 | Other spondylosis, cervical region (for specific types not listed elsewhere) |
This table illustrates the dramatic leap in detail. A coder can now specify if the wear-and-tear is causing nerve compression (radiculopathy) or spinal cord compression (myelopathy), which are critically different clinical scenarios with distinct treatment paths.
Practical Implications: When and Why You Might Still See ICD-9 Code 721.0
Even though it’s obsolete for current billing, you may encounter 721.0 in several situations:
-
Reviewing Historical Medical Records: Patient charts dating before 2015 will use ICD-9 codes. Understanding 721.0 is key to interpreting these records.
-
Handling Older Insurance Claims or Appeals: Disputes or audits related to care provided before October 2015 will reference ICD-9 codes.
-
Academic Research: Studies analyzing long-term trends in spinal conditions often need to bridge data from the ICD-9 and ICD-10 eras, requiring an understanding of both systems.
-
Legacy Software Systems: Some older practice management or analytics tools may still reference ICD-9 codes in their databases.
Helpful List for Patients: If you see “721.0” on an old medical document, here’s what to do:
-
Don’t be alarmed. It was the standard code for neck arthritis/degeneration.
-
Check the date. If the document is from before Fall 2015, it’s historically accurate.
-
For current care, expect to see an ICD-10 code like M47.812 or a more specific variant on new bills and records.
-
Ask for clarification. Your doctor’s office or hospital medical records department can always explain the codes on your documents.
Beyond the Code: The Importance of Accurate Diagnosis
While coding is vital for administration, the true focus must always remain on the patient. A code is a snapshot; a diagnosis is a story.
“The danger in any coding system,” writes healthcare analyst Michael Torres in The Journal of Medical Economics, “is the potential for the code to oversimplify the patient’s experience. Code 721.0 could represent a patient with minor morning stiffness or one with severe neurological deficits. This is exactly why the granularity of ICD-10 represents a significant advance for both quality care and health data analytics.”
Accurate diagnosis of cervical spondylosis involves a thorough patient history, a physical exam, and often, imaging studies. Treatment is equally nuanced, ranging from conservative management (physical therapy, medications) to surgical intervention for severe cases.
Conclusion
The journey to understand the ICD-9 code for cervical spondylosis, 721.0, is more than a look at a retired number. It’s an exploration of how medicine classifies disease, documents care, and evolves to meet the need for greater precision. While this code served as the essential bridge between a patient’s neck pain and the healthcare system for decades, its replacement by the detailed ICD-10-CM system marks a positive shift toward specificity, improving everything from individual treatment plans to global health data.
Frequently Asked Questions (FAQ)
Q: I just saw 721.0 on a recent medical bill. Is this an error?
A: Yes, most likely. For any service provided on or after October 1, 2015, healthcare providers in the U.S. are required to use ICD-10-CM codes. A bill with 721.0 is likely outdated or incorrect. You should contact the billing department for a correction.
Q: What is the most common ICD-10 code for cervical spondylosis now?
A: The most common and direct equivalent is M47.812 (Spondylosis without myelopathy or radiculopathy, cervical region). However, your specific code will depend on whether you have accompanying nerve or spinal cord compression.
Q: Can cervical spondylosis be cured?
A: Cervical spondylosis is a degenerative, age-related condition, so it cannot be “cured” or reversed. However, symptoms can be very effectively managed through a combination of physical therapy, lifestyle modifications, medication, and in some cases, surgery. The goal is to relieve pain, improve function, and prevent neurological progression.
Q: Why is the specificity of ICD-10 so important?
A: Greater specificity leads to better patient care. It allows for more precise tracking of disease subtypes, improves the accuracy of epidemiological research, enables more targeted quality improvement projects, and ensures insurance reimbursement matches the complexity of the patient’s condition.
Q: As a medical student, do I still need to learn ICD-9 codes?
A: Your primary focus should be on mastering ICD-10-CM, as it is the active standard. However, a basic understanding of ICD-9 structure is helpful for reading older medical literature and understanding the historical context of coding. You will not use ICD-9 in clinical practice today.
Additional Resources
For the most authoritative and up-to-date information on medical coding, always refer to the official sources:
-
Centers for Disease Control and Prevention (CDC) ICD-10-CM Page: Provides the official guidelines, indexes, and files for the current coding system. https://www.cdc.gov/nchs/icd/icd-10-cm.htm
-
American Medical Association (AMA) CPT Codes: While ICD codes describe the diagnosis, CPT codes describe the procedures and services performed. Both are necessary for billing. https://www.ama-assn.org/practice-management/cpt
Disclaimer: This article is for informational and educational purposes only. It is not intended as medical advice, coding advice, or a substitute for professional consultation with a qualified healthcare provider or certified medical coder. Medical coding is complex and governed by official guidelines that change regularly. Always refer to the most current official ICD-10-CM code sets and guidelines for accurate, actionable information. The author and publisher disclaim any liability for errors or omissions or for any outcomes related to the use of this information.
Date: January 12, 2026
Author: The Editorial Team at SpineCode Insights





