Navigating medical billing and diagnostic codes can feel like learning a foreign language. If you’re researching medical records, handling billing, or simply trying to understand an old diagnosis, you may have encountered the term “ICD-9 code for infertility.” While this coding system is a historical artifact in modern medicine, understanding it remains crucial for dealing with past records and comprehending the evolution of medical classification.
This comprehensive guide will demystify the ICD-9 coding for infertility. We’ll explore the specific codes, explain why this system is no longer in use, and provide you with the essential knowledge to bridge the gap between past and present medical documentation. Our goal is to turn a complex topic into clear, actionable information you can trust.
ICD-9 Code for Infertility
Understanding the ICD-9 Coding System: A Brief History
Before we dive into the specific code for infertility, let’s establish what ICD-9 was. The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) was the standard system used in the United States to classify and code all diagnoses, symptoms, and procedures for medical billing and statistical tracking.
Think of it as a massive, universal dictionary for health conditions. Every possible ailment had a corresponding numeric code. Hospitals, doctors, and insurance companies used these codes to communicate precisely about a patient’s condition, ensuring accurate billing and enabling public health officials to track disease trends.
ICD-9-CM was implemented in 1979 and served as the backbone of U.S. healthcare documentation for over 35 years. However, by the 2010s, it had become outdated. The system ran out of space for new codes, its structure was not detailed enough for modern medicine, and it couldn’t adequately align with contemporary medical terminology and technology.
“The transition from ICD-9 to ICD-10 was not merely an update; it was a necessary evolution to capture the complexity and specificity of 21st-century healthcare.” – National Center for Health Statistics
This set the stage for a significant change, which we’ll cover in detail. But first, let’s answer the core question.
The Primary ICD-9 Code for Infertility: 628
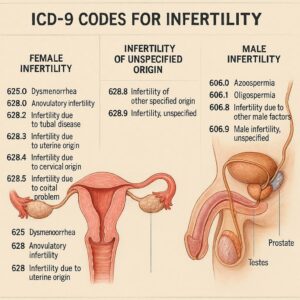
In the ICD-9-CM system, the umbrella code for female infertility is 628. This code is found in Chapter 14: “Diseases of the Genitourinary System.” It’s crucial to understand that “628” alone is a non-specific code. ICD-9-CM required greater specificity for accurate diagnosis and billing, so this parent code was always used with a fourth digit to clarify the etiology or type of infertility.
The complete code structure was 628.X, where “X” represents the essential fourth digit specifying the cause.
Breakdown of ICD-9-CM Infertility Codes (628.X)
The following table outlines the specific subcodes under 628, providing a clear view of how infertility was categorized.
| ICD-9-CM Code | Code Description & Clinical Focus |
|---|---|
| 628.0 | Infertility associated with anovulation. This code was used when infertility was primarily due to the female partner’s failure to ovulate (release an egg). Common causes include Polycystic Ovary Syndrome (PCOS), hypothalamic dysfunction, or premature ovarian failure. |
| 628.1 | Infertility of tubal origin. This applied when the cause was blocked or damaged fallopian tubes, preventing the egg and sperm from meeting. Causes include past pelvic inflammatory disease (PID), endometriosis, or prior surgery. |
| 628.2 | Infertility of uterine origin. This code indicated infertility related to abnormalities of the uterus itself, such as fibroids, adhesions (Asherman’s syndrome), or congenital malformations (like a septate uterus). |
| 628.3 | Infertility of cervical origin. This was used less frequently and related to problems with the cervix, such as hostile cervical mucus that impedes sperm passage or anatomical issues following a surgical procedure like a LEEP. |
| 628.4 | Infertility of other combined female factors. This served as a catch-all for cases where infertility resulted from multiple female factors listed above (e.g., both anovulation and tubal issues). |
| 628.8 | Infertility of other specified origin. This code was for documented female causes not listed elsewhere, such as certain immunological factors. |
| 628.9 | Unspecified infertility. This was the least specific code, used only when no definitive cause for the female infertility could be identified after a basic evaluation. |
Important Note for Readers: If you are reviewing a medical record or bill with one of these codes, remember it exclusively pertains to a female infertility diagnosis. ICD-9-CM had a completely separate chapter and code set for male conditions.
Male Infertility in ICD-9-CM
Male factor infertility was classified in a different chapter (Chapter 10: “Diseases of the Genitourinary System”) under the code range 606.X – Infertility, male. Similar to female codes, these required a fourth digit for specificity (e.g., 606.0 for azoospermia, 606.1 for oligospermia). This separation underscores an older conceptual model of infertility, which modern coding and treatment now view more as a combined “couple’s diagnosis.”
Why ICD-9 Codes Are No Longer in Use: The Transition to ICD-10
As of October 1, 2015, the United States mandated a nationwide transition from ICD-9-CM to ICD-10-CM (the Clinical Modification for diagnoses). This was not a trivial update. The shift was monumental and remains one of the most significant changes in healthcare administration.
Here’s a direct comparison of the two systems regarding infertility coding:
| Feature | ICD-9-CM (Old System) | ICD-10-CM (Current System) |
|---|---|---|
| Code Format | 3-5 digits, mostly numeric (e.g., 628.1) | 3-7 characters, alphanumeric (e.g., N97.0) |
| Specificity | Limited. Broad cause categories. | Highly detailed. Captures laterality, severity, and etiology. |
| Female Infertility Code | Chapter 14: Code 628.X | Chapter 14: Code Series N97.- |
| Male Infertility Code | Chapter 10: Code 606.X | Chapter 14: Code Series N46.- |
| Number of Codes | ~13,000 codes total | ~68,000 codes total |
The transition was necessary because:
-
ICD-9 was full: There were no more unused codes to describe new diseases or procedures.
-
Lacked Clinical Detail: ICD-9 codes couldn’t describe the severity or complexity of a condition, which is vital for modern treatment plans and outcome measurement.
-
Impeded Global Health Data Sharing: Most other developed countries had already adopted ICD-10, hindering international health data comparison and research.
Coding Professional Insight: “Working with ICD-9 codes now feels like using a flip phone. It did the basic job, but ICD-10 is a smartphone—giving us precise GPS coordinates for a diagnosis instead of just the city name. For conditions like infertility, that precision directly impacts patient care and treatment pathways.”
Modern Coding: ICD-10-CM Equivalents for Infertility
Today, if you or a patient is diagnosed with infertility, a coder will use an ICD-10-CM code. The structure is more logical and detailed. Here’s how the old ICD-9 codes map to the current system.
Female Infertility (ICD-10-CM Series N97.-)
The primary code block is N97, “Female infertility.” The level of specificity is greatly enhanced.
-
N97.0 – Female infertility associated with anovulation. (Mapping from 628.0)
-
N97.1 – Female infertility of tubal origin. (Mapping from 628.1). This can be further specified:
-
N97.11 – With tubal block.
-
N97.12 – With peritoneal adhesions.
-
-
N97.2 – Female infertility of uterine origin. (Mapping from 628.2)
-
N97.8 – Female infertility of other origin.
-
N97.9 – Female infertility, unspecified.
Male Infertility (ICD-10-CM Series N46.-)
Male infertility is now logically placed in the same chapter as female infertility (Chapter 14).
-
N46.01 – Azoospermia
-
N46.021 – Oligospermia
-
N46.121 – Asthenospermia
-
N46.8 – Other male infertility
-
N46.9 – Male infertility, unspecified
Helpful List: Why the Specificity of ICD-10 Matters for Patients
-
Accurate Treatment: A code specifying “tubal block” (N97.11) directly informs a treatment plan toward laparoscopic surgery or IVF, whereas an unspecified code does not.
-
Improved Billing Accuracy: Specific codes reduce insurance claim denials and disputes, as the medical necessity for a procedure is clearer.
-
Enhanced Research: Public health researchers can track specific causes of infertility geographically and over time, leading to better understanding and resource allocation.
-
Personalized Care: Detailed coding contributes to a more precise medical record, which follows the patient and informs all future care.
Practical Scenarios: When You Might Still Encounter ICD-9 Codes
While ICD-9 is obsolete for current care, you may encounter these codes in several realistic situations:
-
Reviewing Historical Medical Records: If you are transferring care or compiling a full medical history, records from before October 2015 will use ICD-9 codes.
-
Handling Long-Term Disability or Legal Cases: Claims or cases originating before 2015 will be documented in ICD-9.
-
Academic Research or Data Analysis: Studies analyzing long-term trends may need to reconcile data across both coding systems.
-
Understanding Older Medical Literature: Textbooks or articles published before the transition will reference ICD-9 codes.
Actionable Advice: If you see an ICD-9 code and need to understand it in a modern context, use a reliable crosswalk tool. The Centers for Medicare & Medicaid Services (CMS) and the CDC provide general equivalency mappings (GEMs) to translate between ICD-9 and ICD-10. However, always consult with a medical professional or certified coder for accurate interpretation related to personal health.
Conclusion
Understanding the ICD-9 code for infertility, primarily code 628 and its specific fourth digits, provides a window into the history of medical classification and remains key for interpreting older health records. The transition to ICD-10-CM represented a vital leap forward, offering the granularity needed for today’s personalized medicine. Whether you’re a patient, a healthcare professional, or an administrator, recognizing the difference between these systems empowers you to navigate medical information with greater clarity and confidence, ensuring accurate communication in every aspect of health care.
Frequently Asked Questions (FAQ)
Q: I have an old bill with code 628.1. What does that mean for me today?
A: Code 628.1 indicated “Infertility of tubal origin.” It means your diagnosis prior to October 2015 was related to blocked or damaged fallopian tubes. For current care, your provider would use a more specific ICD-10 code like N97.11. You should discuss this history with your current physician, as it remains a relevant part of your medical history.
Q: Can a doctor still use an ICD-9 code for billing in 2026?
A: No. As of October 1, 2015, all HIPAA-covered entities (hospitals, doctors, insurers) in the U.S. are required to use ICD-10-CM for diagnosis coding. Using an ICD-9 code on a current claim would result in an immediate rejection.
Q: Was there a single ICD-9 code for “infertility” without a specified cause?
A: Yes. The code 628.9 – Unspecified infertility was used when no specific female cause was identified. Its ICD-10 equivalent is N97.9 – Female infertility, unspecified.
Q: How do I find out what my current infertility diagnosis code is?
A: You can ask your healthcare provider’s billing office or check the “Explanation of Benefits” (EOB) statement from your insurance company related to a recent visit. The diagnosis code will be listed there.
Additional Resources
For authoritative information on medical coding systems, visit:
-
The Centers for Disease Control and Prevention (CDC) ICD-10-CM Page: https://www.cdc.gov/nchs/icd/icd10cm.htm (This link provides official guidelines, files, and updates on the current coding system).
Disclaimer: This article is for informational and educational purposes only. It is not intended as medical advice, legal guidance, or official coding instruction. Always consult with a qualified healthcare provider for personal health matters and a certified medical coder or payer for specific billing and coding questions. While every effort has been made to ensure accuracy, coding guidelines are subject to change.





