If you’re navigating medical records, billing, or historical health data, you’ve likely encountered the term “ICD-9 code for COPD.” While the healthcare world has transitioned to ICD-10, understanding the legacy ICD-9 system remains crucial. It’s the key to unlocking decades of patient data, research, and billing history. This guide will provide you with a deep, clear, and practical understanding of the specific ICD-9 codes used for Chronic Obstructive Pulmonary Disease (COPD), their clinical nuances, and their place in modern healthcare documentation.
Think of ICD-9 codes as the old language of diagnosis. To accurately interpret the past, you need to be fluent in it. This isn’t just about memorizing numbers; it’s about understanding a system that categorized one of the world’s most prevalent respiratory conditions. Whether you’re a medical coder, a healthcare student, a researcher, or a patient curious about your own records, this article will serve as your definitive reference.
We’ll move beyond a simple list of codes. We’ll explore what each code truly represents, how they were used in real-world clinical settings, and why the shift to ICD-10 was necessary for conditions as complex as COPD. Our journey will be thorough, filled with practical examples, comparative tables, and essential notes to ensure you gain not just information, but actionable knowledge.
ICD-9 Codes for COPD
Why ICD-9 Codes for COPD Still Matter
You might wonder, “If ICD-10 is the current standard, why spend time on ICD-9?” The reasons are more significant than you may think.
-
Historical Data Analysis: A vast repository of epidemiological studies, treatment outcomes, and public health trends is coded in ICD-9. Researchers analyzing long-term COPD trends or the impact of past interventions must understand this coding language.
-
Legacy Records and Continuity of Care: Patient charts often contain diagnoses recorded under the old system. Understanding these codes is vital for interpreting a patient’s full medical history, especially for a chronic, progressive disease like COPD.
-
Billing and Legal Audits: Insurance claims and legal cases involving care provided before October 2015 were processed using ICD-9. Auditors and analysts must be proficient in this system to review historical claims accurately.
-
Foundation for Learning: ICD-9 provides a simpler framework to grasp diagnostic coding concepts. Understanding its limitations makes the increased specificity of ICD-10 more meaningful and easier to master.
As Dr. Anya Sharma, a pulmonologist and medical informatics specialist, notes: “ICD-9 codes are the chapters of the first draft of modern medical record-keeping. We’ve written more detailed editions since, but you can’t understand the whole story without reading the beginning.”
This quote perfectly encapsulates the enduring value of this knowledge. Let’s begin by breaking down the core codes themselves.
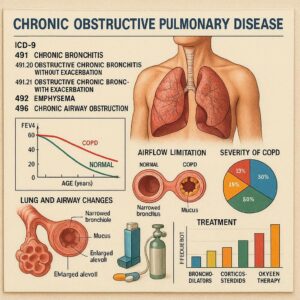
The Core ICD-9 Codes for COPD: 491, 492, and 496
In the ICD-9-CM (Clinical Modification) system, COPD was not a single code but a category encompassing several related conditions. The three primary codes fell under the broader chapter of “Chronic Obstructive Pulmonary Disease and Allied Conditions” (490-496).
The following table provides a high-level overview of these cornerstone codes.
| ICD-9 Code | Code Description | Clinical Focus & Key Characteristics |
|---|---|---|
| 491 | Chronic Bronchitis | Inflammation of the bronchial tubes with chronic cough and sputum production. Diagnosis required symptoms on most days for at least 3 months in two consecutive years. |
| 492 | Emphysema | Damage to the alveoli (air sacs) in the lungs, leading to loss of elasticity and air trapping. Primarily defined by anatomical changes seen on imaging or pathology. |
| 496 | Chronic Airway Obstruction, Not Elsewhere Classified | A code for obstructive lung disease when the specific type (chronic bronchitis or emphysema) was not documented or was a mixture of both. |
Important Note: Code 490, Bronchitis, not specified as acute or chronic, was explicitly excluded from being used for COPD. It was for acute or simple bronchitis. This is a critical distinction that often led to coding errors.
Deep Dive: ICD-9 Code 491 – Chronic Bronchitis
Code 491 was the home for chronic bronchitis. Its definition was very specific and symptom-based, often summarized as “a chronic productive cough for three months in each of two successive years in a patient in whom other causes of chronic cough have been excluded.”
This code had several sub-codes, or “fifth digits,” that added important detail:
-
491.0 – Simple chronic bronchitis. This was used for the most common form.
-
491.1 – Mucopurulent chronic bronchitis. This indicated the presence of infected, pus-containing sputum.
-
491.2 – Obstructive chronic bronchitis. This was a crucial subtype where the inflammation led to measurable airway obstruction (confirmed by spirometry). It often overlapped significantly with emphysema in what was commonly called “COPD.”
-
491.8 – Other chronic bronchitis. A catch-all for other specified types.
-
491.9 – Unspecified chronic bronchitis.
Coding Scenario: A patient with a 10-year history of smoking presents with a daily productive cough for the past 4 years. Spirometry shows mild airway obstruction. The physician documents “Chronic obstructive bronchitis.”
-
Correct ICD-9 Code: 491.2 (Obstructive chronic bronchitis).
Deep Dive: ICD-9 Code 492 – Emphysema
Unlike chronic bronchitis, emphysema (492) was defined by its structural pathology. The code represented the irreversible enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls.
Its sub-codes were:
-
492.0 – Emphysematous bleb.
-
492.8 – Other emphysema.
The clinical diagnosis was often based on a combination of physical exam (barrel chest, decreased breath sounds), imaging (hyperinflated lungs on X-ray, CT scan showing bullae), and lung function tests showing air trapping.
A key point of confusion: Many patients have both emphysema and chronic bronchitis. In ICD-9, if the physician documented both, both codes (491.2 and 492.8) could be used together. This was a fundamental way the system tried to capture the complexity of COPD.
Deep Dive: ICD-9 Code 496 – The “Unspecified” Obstruction
Code 496 was one of the most frequently used—and sometimes misused—codes in the ICD-9 COPD set. Its full title was “Chronic airway obstruction, not elsewhere classified.”
It was intended for cases of clinically significant, chronic airway obstruction where the physician did not specify whether it was primarily emphysema or chronic bronchitis. In everyday practice, it was often used as a generic “COPD” code when the clinical documentation was vague.
Guideline for Use:
-
Use 496 if: The documentation states only “COPD,” “chronic obstructive lung disease,” or “chronic airway obstruction” without further specification.
-
Do NOT use 496 if: The documentation specifies “chronic bronchitis” (use 491.x) or “emphysema” (use 492.x). 496 was a residual category.
Important Note for Readers: The over-reliance on code 496 was a major driver for the creation of ICD-10. It provided little detail for tracking disease subtypes, severity, or complications, hindering quality research and targeted care management.
Comparative Analysis: ICD-9 Codes in Practice
To visualize how these codes applied to different patient presentations, consider the following table.
| Patient Presentation & Documentation | Primary ICD-9 Code | Rationale & Additional Codes |
|---|---|---|
| “70-year-old male, long-time smoker, with dyspnea on exertion. CT chest shows panlobular emphysema.” | 492.8 (Other emphysema) | Documentation specifies emphysema based on imaging. |
| “Patient with history of COPD presents with increased cough and thick, green sputum for 1 week.” | 491.1 (Mucopurulent chronic bronchitis) + 466.0 (Acute bronchitis) | The acute exacerbation with purulent sputum points to 491.1. The acute episode may be separately coded. |
| “Diagnosis: COPD. Patient has chronic shortness of breath and airway obstruction per PFTs.” | 496 (Chronic airway obstruction, NOS) | Documentation is non-specific, using only the umbrella term “COPD.” |
| “Established patient with severe obstructive chronic bronchitis and bullous emphysema.” | 491.2 (Obstructive chronic bronchitis) and 492.8 (Other emphysema) | Physician documents both components of the disease. Both codes are assigned. |
| “Patient with chronic cough, no obstruction on spirometry.” | 491.0 or 491.9 (Simple/Unspecified chronic bronchitis) | Symptoms meet definition of chronic bronchitis, but without obstruction. Code 496 would be incorrect. |
The Critical Transition from ICD-9 to ICD-10 for COPD
The shift from ICD-9 to ICD-10 on October 1, 2015, was a revolution in diagnostic coding, especially for chronic diseases like COPD. The limitations of ICD-9—vague codes, lack of detail—were directly addressed.
Why ICD-9 Was Insufficient for Modern COPD Care
-
Lack of Specificity: Code 496 told you nothing about the type, severity, or underlying cause of the obstruction.
-
No Detail on Complications: There was no way to code if the COPD was associated with an acute exacerbation or lower respiratory infection in a single code.
-
Limited Etiology Codes: While you could add a separate code for tobacco use (305.1), it wasn’t integrated into the COPD code itself.
-
Inability to Capture Severity: ICD-9 had no mechanism to indicate whether the COPD was mild, moderate, or severe based on lung function.
How ICD-10 Transformed COPD Coding
ICD-10 uses a single code set, J44.-, for COPD, but with extensive detail via later characters. Let’s contrast the systems:
| Feature | ICD-9 (491, 492, 496) | ICD-10 (J44.-) |
|---|---|---|
| Disease Type | Separate codes for bronchitis (491), emphysema (492), and unspecified (496). | Combined into J44, with ability to specify with emphysema (J43.-) if needed. |
| Exacerbations | Required separate codes for acute bronchitis (466.0) or other acute conditions. | Built into the primary code (e.g., J44.1 for COPD with acute exacerbation). |
| Associated Conditions | Required multiple codes (e.g., one for COPD, one for acute bronchitis, one for tobacco use). | Can be integrated (e.g., J44.0 for COPD with acute lower respiratory infection). |
| Severity | Not captured in the code. | Not directly in the base code, but often indicated via associated codes for FEV1 results. |
| Etiology | Separate code for tobacco use (305.1). | Tobacco use is captured via a separate but essential code from series Z77.22, History of tobacco use. |
Example Translation:
-
ICD-9: 496 (COPD, unspecified) + 466.0 (Acute bronchitis) + 305.1 (Tobacco use disorder)
-
ICD-10: J44.1 (COPD with acute exacerbation) + Z77.22 (History of tobacco use)
The ICD-10 code provides a clearer, more complete clinical picture in a more efficient package.
Practical Applications: Using ICD-9 Knowledge Today
Your understanding of ICD-9 codes for COPD isn’t just academic. It applies in several real-world scenarios.
For Medical Coders and Auditors:
-
Reviewing Legacy Records: You can accurately abstract data from old charts for quality reporting or research.
-
Handling Old Appeals: You can defend or challenge claims from the ICD-9 era with confidence.
-
Educating Clinicians: You can explain why current ICD-10 documentation needs to be more specific by showing the limitations of old, vague codes like 496.
For Healthcare Providers and Students:
-
Understanding Disease History: Reading old research or a patient’s past records becomes meaningful.
-
Appreciating Coding Evolution: You see firsthand how better data leads to better disease management frameworks.
For Patients and Advocates:
-
Deciphering Old Records: You can better understand diagnoses listed on past medical summaries or billing statements.
-
Participating in Research: You can comprehend studies that use ICD-9 data to track long-term health outcomes.
Common Pitfalls and Errors with ICD-9 COPD Codes
Even experienced professionals could stumble. Here are the most frequent mistakes to avoid:
-
Using 490 for Chronic Conditions: Code 490 was for acute bronchitis. Using it for a chronic condition was incorrect.
-
Defaulting to 496 When Specificity Exists: If the record said “emphysema,” coders should use 492.8, not the easier 496.
-
Ignoring Fifth Digits: Not specifying between simple (491.0), mucopurulent (491.1), or obstructive (491.2) chronic bronchitis lost valuable clinical data.
-
Not Coding Co-existing Conditions: Failing to list both 491.2 and 492.8 when both were present provided an incomplete picture.
-
Missing Tobacco Use Code: While not part of the COPD code itself, omitting 305.1 for active smokers was a common oversight that impacted risk adjustment and billing.
Helpful List: Quick Reference for Accurate ICD-9 COPD Coding
-
Step 1: Look for the physician’s specific terminology.
-
Step 2: If “emphysema” is stated, code 492.8.
-
Step 3: If “chronic bronchitis” is stated, determine the type and code from the 491.x series.
-
Step 4: If only “COPD” or “chronic airway obstruction” is stated, use 496.
-
Step 5: Check if both chronic bronchitis and emphysema are documented; if so, use both 491.2 and 492.8.
-
Step 6: Always consider adding code 305.1 for tobacco use if applicable.
Conclusion
Understanding the ICD-9 codes for COPD—primarily 491 for chronic bronchitis, 492 for emphysema, and 496 for unspecified obstruction—is essential for interpreting decades of healthcare data and ensuring continuity in patient care. While the ICD-10 system now offers superior specificity, the legacy of ICD-9 remains locked in millions of records, making fluency in this “old language” a valuable professional skill. By mastering these codes and their clinical meanings, you unlock a clearer understanding of the disease’s history, its management evolution, and the critical importance of precise diagnostic documentation.
Frequently Asked Questions (FAQ)
Q1: What was the most common ICD-9 code used for COPD?
A: Code 496, “Chronic airway obstruction, not elsewhere classified,” was often the most commonly used because it served as a catch-all when physician documentation was not specific. However, in well-documented records, the more specific codes 491.2 (obstructive chronic bronchitis) and 492.8 (emphysema) were frequently used, either alone or together.
Q2: Can a patient have both an ICD-9 code for chronic bronchitis and emphysema?
A: Yes, absolutely. In fact, this combination was very common. When a physician documented both conditions, medical coders were instructed to assign both 491.2 (Obstructive chronic bronchitis) and 492.8 (Emphysema). This provided a more accurate representation of the patient’s complex disease state than using the generic code 496.
Q3: How do I find out which ICD-9 code was used for my old diagnosis?
A: You can review old medical billing statements (Explanation of Benefits from your insurer), hospital discharge summaries, or physician notes from before October 2015. The diagnosis code is usually listed next to the description of the service. You can also request a copy of your full medical records, which will include coded diagnosis lists.
Q4: Why did ICD-10 add so many more codes for COPD?
A: ICD-10 was designed to capture much more clinical detail. For COPD, this means being able to indicate in a single code whether the patient is having an exacerbation (J44.1), has a concurrent lower respiratory infection (J44.0), or is in a stable state (J44.9). This specificity improves tracking of disease patterns, treatment outcomes, and healthcare resource utilization, leading to better research and care models.
Additional Resources
For those looking to delve deeper into historical coding or understand the transition more fully, we recommend:
-
The Centers for Medicare & Medicaid Services (CMS) ICD-9-CM Official Guidelines for Coding and Reporting (Archive): The definitive source for official coding rules during the ICD-9 era.
-
The American Lung Association (lung.org): Provides excellent patient-centered and clinical information on COPD, including its history and definitions.
-
Global Initiative for Chronic Obstructive Lung Disease (GOLD) Reports (goldcopd.org): The international standard for COPD diagnosis, management, and prevention. While focused on clinical practice, it helps understand the disease entities being coded.
Disclaimer: This article is for informational and educational purposes only. It is based on historical coding guidelines and does not constitute medical or coding advice. For current diagnostic coding, always use the official ICD-10-CM code set and the most recent official coding guidelines. For medical advice, always consult with a qualified healthcare professional. The author and publisher are not responsible for any errors or omissions or for any outcomes related to the use of this information.
Date: December 30, 2025
Author: The Editorial Team at CodeCraft Clinical Insights





