Navigating the world of medical coding, even for a condition as common as a gastrointestinal (GI) bleed, can feel like deciphering an ancient language. While the healthcare industry in the United States transitioned to ICD-10-CM on October 1, 2015, understanding the legacy ICD-9 code for GI bleed remains crucial. Why? Historical data analysis, auditing older records, understanding the evolution of coding specificity, and even dealing with certain legacy systems or research datasets all require fluency in ICD-9.
This comprehensive guide is designed to be your enduring reference. We’ll move beyond a simple code lookup to explore the logic, documentation requirements, and clinical nuances behind accurately classifying a GI bleed under the ICD-9 system. Whether you’re a medical coder auditing old charts, a healthcare professional refreshing your knowledge, or a student of health informatics, this deep dive will equip you with a thorough understanding.
ICD-9 Codes for Gastrointestinal Bleed
Understanding the ICD-9-CM System: A Snapshot in Time
The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) was the diagnostic coding standard in the U.S. for over three decades. Compared to its successor, ICD-10, it was characterized by a much smaller code set (around 14,000 codes vs. over 68,000 in ICD-10) and less clinical specificity.
A Key Limitation: In ICD-9, the code for a GI bleed often lacked precise anatomical detail. While ICD-10 allows you to specify the exact part of the colon (e.g., angiodysplasia of colon with hemorrhage), ICD-9 frequently required broader categories. This inherent lack of granularity is the central theme when looking back at these codes.
Why Knowing ICD-9 Codes Still Matters
-
Historical Record Review: Analyzing patient histories or outcomes from pre-2015 data.
-
Legal and Audit Cases: Reviewing medical-legal or billing audit cases that originated before the transition.
-
Research Continuity: Understanding older epidemiological studies or maintaining longitudinal research datasets.
-
System Migration: Working with older practice management or EHR software that may still reference ICD-9 logic.
The Foundational ICD-9 Code for GI Bleed: 578.9
In the ICD-9-CM universe, the most general, unspecified code for a gastrointestinal hemorrhage was:
578.9 – Hemorrhage of gastrointestinal tract, unspecified
This code was the equivalent of a catch-all. It was used when the medical documentation did not specify the origin (upper vs. lower) or the nature (e.g., ulcer, diverticula) of the bleed. From a coding and billing perspective, 578.9 was often considered a “low-specificity” code and could be seen as a red flag for auditors if more specific information was available in the chart.
Important Note: “Unspecified codes are necessary when the clinical information available is insufficient to assign a more specific code. However, their overuse can indicate gaps in clinical documentation and may impact reimbursement in historical contexts.” – *Principle of ICD-9-CM Coding*
The Critical Importance of Documentation
Under ICD-9, as now, the code assigned was a direct reflection of the provider’s documentation. Coders could only code what they could read. Key documentation elements needed to move beyond 578.9 included:
-
Site: Upper GI (esophagus, stomach, duodenum) vs. Lower GI (jejunum, ileum, colon, rectum).
-
Etiology: Peptic ulcer, diverticulosis, angiodysplasia, hemorrhoids, varices.
-
Acuity: Acute versus chronic blood loss.
-
Manifestations: Signs of anemia, hypovolemia.
Breaking Down GI Bleed Codes by Site and Cause
To code accurately, one had to navigate the ICD-9 index and tabular list. Here is a structured breakdown of the most common ICD-9 codes for GI bleeds, organized by anatomical site.
Upper Gastrointestinal Hemorrhage (Codes 530.xx – 537.xx)
Upper GI bleeds originate from a source proximal to the ligament of Treitz (esophagus, stomach, duodenum).
| ICD-9 Code | Code Description | Clinical Context & Notes |
|---|---|---|
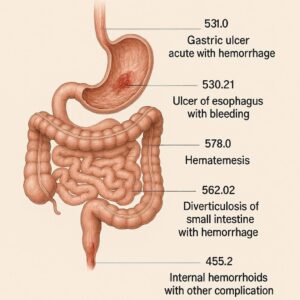
| 531.0x | Acute gastric ulcer with hemorrhage | Requires a 5th digit to specify obstruction status (0=without obstruction, 1=with obstruction). |
| 531.2x | Acute gastric ulcer with hemorrhage and perforation | For bleeding ulcers that have also perforated. |
| 532.0x | Acute duodenal ulcer with hemorrhage | 5th digit required for obstruction. |
| 530.21 | Ulcer of esophagus with hemorrhage | Esophageal ulcer causing bleed. |
| 530.82 | Esophageal hemorrhage | Bleeding from the esophagus, not specified as ulcer or varices. |
| 456.0 | Esophageal varices with bleeding | A major cause of upper GI bleed in patients with portal hypertension. |
| 537.83 | Angiodysplasia of stomach and duodenum with hemorrhage | Vascular malformation causing bleed. |
| 535.0x | Acute gastritis with hemorrhage | 5th digit specifies presence of obstruction. |
Lower Gastrointestinal Hemorrhage (Codes 558.xx – 569.xx)
Lower GI bleeds originate from the small intestine or colon.
| ICD-9 Code | Code Description | Clinical Context & Notes |
|---|---|---|
| 562.13 | Diverticulosis of colon with hemorrhage | One of the most common causes of major lower GI bleed. |
| 569.85 | Angiodysplasia of colon with hemorrhage | Common in elderly patients. |
| 569.3 | Hemorrhage of rectum and anus | A broad category for rectal bleeding. |
| 455.x | Hemorrhoids | 455.2: Internal hemorrhoids with bleeding. 455.5: External hemorrhoids with bleeding. 455.8: Unspecified hemorrhoids with bleeding. |
| 556.8 | Other ulcerative colitis with hemorrhage | For bleeds due to inflammatory bowel disease. |
| 558.9 | Other and unspecified noninfectious gastroenteritis and colitis | Sometimes used for unspecified colitis with bleed. |
Miscellaneous & Unspecified Codes
| ICD-9 Code | Code Description | When It Was Used |
|---|---|---|
| 578.9 | Hemorrhage of GI tract, unspecified | Default when no site or cause is documented. |
| 578.1 | Blood in stool | Symptom code for melena or hematochezia without confirmed source. |
| 280.0 | Iron deficiency anemia secondary to blood loss (chronic) | A frequent secondary code to indicate the consequence of chronic GI bleeding. |
| 285.1 | Acute posthemorrhagic anemia | Used for anemia due to acute, significant blood loss. |
From Clinical Picture to Accurate Code: A Step-by-Step Process
How would a coder approach a historical record? The process was methodical.
-
Review the Final Diagnoses: Start with the discharge summary or problem list.
-
Consult the Procedural Notes: Endoscopy (EGD, colonoscopy), capsule endoscopy, or angiography reports are goldmines for specificity. They state exactly what was found and where.
-
Analyze the History & Physical (H&P) and Progress Notes: Look for descriptions of hematemesis (vomiting blood), melena (black, tarry stool), or hematochezia (bright red blood per rectum).
-
Check Laboratory and Pathology Results: Falling hemoglobin/hematocrit, blood urea nitrogen (BUN) rise, and pathology from biopsies confirm and specify causes.
-
Navigate the ICD-9 Manual:
-
Index: Look up main terms like “Hemorrhage,” “Bleeding,” “Ulcer,” or “Diverticulosis,” then navigate to the subterms (e.g., “gastric,” “with hemorrhage”).
-
Tabular List: Always verify the code in the numeric tabular list for complete instructions, inclusion notes, and exclusion notes.
-
-
Assign the Most Specific Code: Never code a symptom (578.1) if a definitive diagnosis (562.13) is established. Follow the ICD-9 hierarchy of specificity.
Case Study Example: Applying ICD-9 Logic
-
Scenario: A 70-year-old patient presents to the ER in 2014 with sudden, painless bright red blood per rectum. Colonoscopy reveals active bleeding from a diverticulum in the sigmoid colon.
-
Documentation Keywords: Hematochezia, diverticulosis, active bleeding, sigmoid colon.
-
ICD-9 Code Assignment: 562.13 (Diverticulosis of colon with hemorrhage). The coder would not use 578.9 or 578.1 because a more specific cause was identified.
-
Potential Secondary Code: 285.1 (Acute posthemorrhagic anemia) if the Hgb dropped significantly.
Comparative Analysis: ICD-9 vs. ICD-10 for GI Bleed
The transition to ICD-10-CM was a revolution in specificity. This table highlights the dramatic shift.
| Aspect | ICD-9-CM | ICD-10-CM | Impact of Change |
|---|---|---|---|
| Code Structure | 3-5 digits, mostly numeric. | 3-7 characters, alphanumeric. | Allows for vastly more combinations and detail. |
| Specificity for Site | Often broad (e.g., “colon”). | Highly precise (e.g., “sigmoid colon,” “transverse colon”). | Improves disease tracking, research, and reimbursement accuracy. |
| Specificity for Etiology | Combined with site (e.g., 531.0x). | Separate codes for laterality, acuity, and associated conditions. | Clearer clinical picture from the code itself. |
| Example: Diverticular Bleed | 562.13 (Diverticulosis of colon with hemorrhage). | K57.31 (Diverticulosis of large intestine with bleeding, without perforation or abscess). Further specificity: – K57.32 (with perforation and abscess) – K57.5X (for small intestine). |
ICD-10 distinguishes between large/small intestine and complications. |
| Example: Gastric Ulcer Bleed | 531.0x (Acute gastric ulcer with hemorrhage). | K25.0 (Acute gastric ulcer with hemorrhage). Plus, ICD-10 requires no 5th digit for obstruction; it’s a clearer, standalone code for the complication. | Streamlined and more intuitive categorization. |
| Unspecified Code | 578.9 (Hemorrhage of GI tract, unspecified). | K92.2 (Gastrointestinal hemorrhage, unspecified). | Similar concept, but part of a much more detailed hierarchy. |
Essential Lists for Accurate ICD-9 Coding
Documentation “Must-Haves” for Specific Coding
To avoid the unspecified 578.9, physicians needed to document:
-
The precise anatomical site of the bleed (e.g., gastric antrum, descending colon).
-
The underlying cause (e.g., NSAID-induced ulcer, diverticulosis).
-
The acuity of the bleed (acute vs. chronic).
-
Any associated complications (perforation, obstruction, anemia).
-
Confirmation method (e.g., “on EGD,” “seen on colonoscopy”).
Common Pitfalls & Errors in Historical Coding
-
Coding the Symptom Only: Using 578.1 (Blood in stool) when a definitive diagnosis like 562.13 was established.
-
Missing Combination Codes: ICD-9 had combination codes that included both the condition and the hemorrhage (e.g., 531.0x, 562.13). Using two separate codes was incorrect.
-
Ignoring the 5th Digit: For categories like ulcer codes (531-534), failing to add the required 5th digit to indicate obstruction (1) or no obstruction (0).
-
Overlooking Underlying Causes: Not coding the etiology when known (e.g., coding for ulcer bleed but missing code for chronic use of NSAIDs or H. pylori infection).
-
Sequencing Errors: Inpatient coding required sequencing the diagnosis that occasioned the admission (the GI bleed) as the principal diagnosis.
Frequently Asked Questions (FAQ)
Q: What is the most common ICD-9 code for a GI bleed?
A: In practice, 578.9 (unspecified hemorrhage) was used frequently due to documentation gaps. However, for known causes, 562.13 (diverticular bleed) and the 531.0x/532.0x series (bleeding ulcers) were among the most common specific codes.
Q: Can I still use ICD-9 codes for billing today?
A: No. For all healthcare services provided on or after October 1, 2015, in the U.S., you must use ICD-10-CM codes for diagnosis reporting on claims. Using ICD-9 will result in claim rejection.
Q: How do I convert an old ICD-9 code to ICD-10?
A: There is no simple 1-to-1 conversion. You must take the clinical description from the medical record and find the appropriate, more specific ICD-10-CM code. The Centers for Medicare & Medicaid Services (CMS) and the CDC provided general equivalence mappings (GEMs), but they are guides, not direct crosswalks.
Q: Why was ICD-9 replaced?
A: ICD-9-CM was outdated, lacked the specificity needed for modern medicine, and was no longer accommodative of new procedures and diagnoses. ICD-10 provides greater detail for patient care, public health tracking, and value-based reimbursement models.
Q: Where can I find official ICD-9 archives?
A: The CDC maintains an archive of the ICD-9-CM guidelines and codesets. The National Center for Health Statistics (NCHS) website is the authoritative source for historical code information.
Conclusion
Mastering the ICD-9 code for GI bleed required understanding a less granular but rule-based system centered on categories like 578.9, 562.13, and the 531.0x-534.0x series. While historic, this knowledge remains vital for interpreting pre-2015 data and appreciating the significant advances in clinical specificity brought by ICD-10-CM. Accurate coding, in any era, always begins and ends with precise, detailed clinical documentation.
Additional Resource:
For the official ICD-10-CM codes and guidelines that are currently in effect, please visit the Centers for Disease Control and Prevention (CDC) ICD-10 page: CDC ICD-10-CM.
Author: Medical Coding Specialist
Date: January 26, 2026
Disclaimer: This article is for informational purposes only and is based on historical ICD-9-CM data. For official coding, always consult the most current ICD-10-CM guidelines and your payer-specific policies.





