In the intricate world of modern healthcare, a Traumatic Brain Injury (TBI) is documented not just through clinical notes and imaging reports, but through a precise, alphanumeric language: the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). To the uninitiated, codes like S06.0X0A or S06.5X9D may seem like impersonal, bureaucratic jargon. However, these codes are far from arbitrary. They are a critical linchpin connecting patient care, medical research, public health policy, and healthcare economics. Each digit holds significance, painting a detailed picture of the injury’s nature, its severity, the circumstances under which it occurred, and the stage of treatment the patient is in.
Accurate ICD-10 coding for TBI is a discipline that demands a symbiotic understanding of clinical medicine and administrative precision. A miscoded chart is not merely a clerical error; it can lead to denied insurance claims, skewed epidemiological data that misguides public health efforts, and an incomplete medical record that fails to communicate the true complexity of the patient’s condition to future providers. This article serves as an exhaustive guide for medical coders, healthcare administrators, clinicians, researchers, and even informed patients and advocates, demystifying the complex coding system that underpins the management and understanding of traumatic brain injury. We will journey from the foundational principles of ICD-10 to the nuanced application of its codes, ensuring that by the end, you will see these codes not as cold numbers, but as a vital narrative tool in the story of a patient’s health.
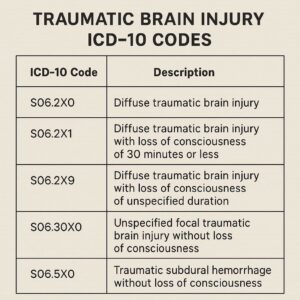
Traumatic Brain Injury ICD-10 Codes
2. Understanding the Foundation: What is the ICD-10-CM?
The International Classification of Diseases (ICD) is the global standard for diagnostic health information, maintained by the World Health Organization (WHO). The “Tenth Revision” (ICD-10) was adopted by the WHO in 1990. However, the United States uses a clinically modified version, aptly named ICD-10-CM, which was implemented on October 1, 2015, replacing the outdated ICD-9-CM system.
The ICD-10-CM is vastly more detailed and specific than its predecessor. While ICD-9-CM had around 13,000 codes, ICD-10-CM boasts over 68,000. This expansion was necessary to capture the complexity of modern medicine, allowing for greater specificity in describing a patient’s condition, including laterality (left, right, bilateral), etiology, anatomic site, and severity.
The primary purposes of the ICD-10-CM are:
-
Morbidity Classification: Tracking diseases and health conditions.
-
Epidemiology: Studying the incidence, distribution, and control of diseases in populations.
-
Clinical Care: Supporting treatment decisions and outcomes measurement.
-
Health Services Research: Analyzing utilization and quality of care.
-
Billing and Reimbursement: Providing the codes required for insurance claims and determining payment based on Diagnosis-Related Groups (DRGs) and other payment models.
For TBI, this specificity is paramount. The difference between a concussion and a subdural hemorrhage is immense in terms of treatment, prognosis, and resource utilization, and the coding system must reflect that.
3. The Clinical Landscape of Traumatic Brain Injury (TBI)
Before one can code a condition, one must understand it clinically.
Defining Traumatic Brain Injury
A TBI is defined as an alteration in brain function, or other evidence of brain pathology, caused by an external force. The “alteration in brain function” can include any period of decreased or lost consciousness, loss of memory for events immediately before or after the injury (amnesia), neurological deficits (e.g., weakness, loss of balance, vision changes, disorientation), or any alteration in mental state at the time of the injury (e.g., feeling dazed, confused, or disoriented).
Mechanisms and Common Causes of TBI
The external force can be a direct blow to the head, a jolt to the body that causes the brain to whip back and forth within the skull (as in whiplash), or a penetrating injury like a gunshot wound. Common causes include:
-
Falls (the leading cause, especially in young children and older adults)
-
Motor vehicle accidents
-
Being struck by or against an object (e.g., sports injuries, assaults)
-
Explosive blasts and other combat-related injuries (a significant cause for military personnel)
The Spectrum of Severity: Mild, Moderate, and Severe
TBIs are classified by severity, typically using tools like the Glasgow Coma Scale (GCS), the length of loss of consciousness (LOC), and the duration of post-traumatic amnesia (PTA).
-
Mild TBI (mTBI/Concussion): GCS 13-15, LOC for 0-30 minutes, PTA for <24 hours. Symptoms can be subtle but debilitating (headache, dizziness, fatigue, cognitive fog).
-
Moderate TBI: GCS 9-12, LOC for 30 minutes to 24 hours, PTA for 1-7 days.
-
Severe TBI: GCS 3-8, LOC for >24 hours, PTA for >7 days. Often involves significant structural damage and long-term disability.
This clinical stratification directly informs coding choices, particularly the selection of the most specific code available.
4. Navigating the ICD-10-CM Coding Manual: A Structure Primer
ICD-10-CM is organized into 22 chapters, mostly based on body system or disease type. TBI codes are primarily found in two places.
The Chapter of Injury, Poisoning and Certain Other Consequences of External Causes (S00-T88)
This chapter, specifically the blocks S00-S09, covers “Injuries to the head.” This is the home for the majority of acute TBI codes. Codes in this chapter require an additional 7th character to specify the “type of encounter.”
The Importance of the 7th Character: Encounter Specificity
This is a critical concept in injury coding. The 7th character extends the code to provide context on the phase of care:
-
A: Initial encounter: Used while the patient is receiving active treatment for the injury (e.g., in the ER, during hospitalization, or at a follow-up visit where active treatment is still occurring).
-
D: Subsequent encounter: Used for routine care after the active phase of treatment is complete. This includes encounters for healing, recovery, monitoring, and management of complications that have arisen.
-
S: Sequela: Used for complications or conditions that arise as a direct consequence of the initial injury, but are themselves being treated at a later date (e.g., coding for epilepsy that developed due to a head injury years prior).
The Role of External Cause Codes (Chapter 20)
While not used for billing, external cause codes (V00-Y99) are crucial for completing the narrative. They describe how the injury occurred. For TBI, this is essential for public health tracking. These codes are secondary codes that provide information on:
-
Intent: Unintentional (accident), assault, self-harm, undetermined.
-
Mechanism: Fall, motor vehicle traffic accident, struck by object.
-
Place of Occurrence: Home, sports arena, street.
-
Activity: While playing football, while gardening.
-
Status: Person on duty (e.g., a worker), bystander.
Using these codes allows researchers to identify, for example, if TBIs from bicycle accidents are increasing in a specific region, informing preventative public safety campaigns.
5. The Core Codes: A Deep Dive into S06 for Intracranial Injury
The S06 category is the heart of TBI coding. It’s vital to note that these codes are hierarchical. The code for the most severe injury takes precedence. For example, if a patient has both a concussion (S06.0X-) and a subdural hemorrhage (S06.5X-), you code only the subdural hemorrhage, as it includes any associated loss of consciousness, which is the hallmark of a concussion.
S06.0X-: Concussion – The Invisible Injury
A concussion is a mild TBI caused by a bump, blow, or jolt to the head or body that causes the brain to move rapidly inside the skull.
-
Coding: The 5th character (X) is a placeholder. The 6th character specifies the presence and duration of loss of consciousness (LOC).
-
0: Loss of consciousness of 30 minutes or less
-
1: Loss of consciousness of 31 minutes to 59 minutes
-
2: Loss of consciousness of 1 hour to 5 hours 59 minutes
-
3: Loss of consciousness of 6 hours to 24 hours
-
4: Loss of consciousness greater than 24 hours
-
9: Concussion without loss of consciousness
-
-
Example:
S06.0X0A– Concussion with loss of consciousness of 30 minutes or less, initial encounter.
S06.1X-: Traumatic Cerebral Edema – The Swelling Menace
This is swelling of the brain tissue itself, a serious and potentially life-threatening condition that often accompanies severe TBIs.
-
Coding: The 6th character uses the same LOC scale as S06.0X-.
-
Example:
S06.1X3D– Traumatic cerebral edema with loss of consciousness of 6-24 hours, subsequent encounter.
S06.2X-: Diffuse and Focal Brain Injury
This code covers a range of primary brain injuries, including diffuse axonal injury (widespread tearing of nerve fibers) and more specific focal contusions or lacerations.
-
Coding: The 6th character uses the same LOC scale.
-
Example:
S06.2X1A– Diffuse traumatic brain injury with loss of consciousness of 31-59 minutes, initial encounter.
S06.3-: Focal Brain Injury and Beyond
This is a catch-all for other specific types of focal brain injury not covered elsewhere.
S06.4-: Epidural Hemorrhage
A bleed between the skull and the dura mater (the tough outer membrane), often due to a skull fracture tearing an artery. It’s a neurosurgical emergency characterized by a “lucid interval” where the patient seems fine before rapidly deteriorating.
-
Coding: The 5th character specifies with or without loss of consciousness.
-
0: Without loss of consciousness
-
1: With loss of consciousness of any duration
-
9: With loss of consciousness of unspecified duration
-
-
Example:
S06.4X0A– Epidural hemorrhage without loss of consciousness, initial encounter.
S06.5-: Traumatic Subdural Hemorrhage
A bleed between the dura mater and the brain surface (in the subdural space), usually from torn veins. Common in falls in the elderly, even minor ones, and can be acute or chronic.
-
Coding: Uses the same 5th character structure as S06.4-.
-
Example:
S06.5X1D– Traumatic subdural hemorrhage with loss of consciousness, subsequent encounter.
S06.6-: Traumatic Subarachnoid Hemorrhage
A bleed into the subarachnoid space, where cerebrospinal fluid circulates. This can cause a sudden, severe “thunderclap” headache.
-
Coding: Uses the same 5th character structure as S06.4- and S06.5-.
-
Example:
S06.6X9A– Traumatic subarachnoid hemorrhage with loss of consciousness of unspecified duration, initial encounter.
S06.8-: Other Intracranial Injuries
This includes injuries like primary blast injury of the brain.
S06.9-: Unspecified Intracranial Injury
This is a vague code that should be used only when the medical documentation is insufficient to assign a more specific code. It is generally discouraged as it provides little clinical or epidemiological value.
Summary of Key S06 Intracranial Injury Codes
| ICD-10 Code | Description | Key Clinical Note | 5th/6th Character Guidance |
|---|---|---|---|
| S06.0X- | Concussion | Mild TBI. Code includes any altered mental status. | 6th char: Specifies duration of LOC (0-4, 9) |
| S06.1X- | Traumatic Cerebral Edema | Serious brain swelling. Often secondary to other injury. | 6th char: Specifies duration of LOC (0-4, 9) |
| S06.2X- | Diffuse Traumatic Brain Injury | Includes diffuse axonal injury (DAI). | 6th char: Specifies duration of LOC (0-4, 9) |
| S06.4X- | Epidural Hemorrhage | Arterial bleed, often with lucid interval. Neurosurgical emergency. | 5th char: 0 (no LOC), 1 (with LOC), 9 (unspec LOC) |
| S06.5X- | Traumatic Subdural Hemorrhage | Venous bleed. Common in elderly after falls. Can be acute/chronic. | 5th char: 0 (no LOC), 1 (with LOC), 9 (unspec LOC) |
| S06.6X- | Traumatic Subarachnoid Hemorrhage | Bleed into CSF space. Causes thunderclap headache. | 5th char: 0 (no LOC), 1 (with LOC), 9 (unspec LOC) |
| S06.9X- | Unspecified Intracranial Injury | Use sparingly. Indicates lack of specific documentation. | 5th char: 0 (no LOC), 1 (with LOC), 9 (unspec LOC) |
6. Associated Injuries and Sequela: Coding the Complete Picture
A TBI rarely occurs in isolation. Coders must be vigilant for associated conditions that require their own codes.
Skull Fractures (S02.-)
A skull fracture is coded separately from the intracranial injury unless the code description includes the fracture (which S06 codes do not).
-
S02.0-: Fracture of vault of skull
-
S02.1-: Fracture of base of skull
-
S02.2-: Fracture of nasal bones
-
S02.3-: Fracture of orbital floor (blowout fracture)
-
S02.4-: Fracture of zygomatic and maxillary bones
-
S02.5-: Fracture of tooth
-
S02.6-: Fracture of mandible
-
S02.7-: Multiple fractures of skull and facial bones
-
S02.8-: Fractures of other skull and facial bones
-
S02.9-: Unspecified fracture of skull and facial bones
-
Laterality: Most fracture codes require a 6th character for laterality (1 – right, 2 – left, 0 – unspecified, 9 – not applicable).
-
Example: A patient with a TBI and a right parietal skull fracture would be coded as
S02.0X1A(Fracture of vault of skull, right, initial encounter) and the appropriate S06 code.
Open Wounds of the Head (S01.-)
If the injury includes an open wound (a laceration, avulsion, etc.), it must be coded separately.
-
S01.0-: Open wound of scalp
-
S01.1-: Open wound of eyelid and periocular area
-
S01.8-: Open wound of other parts of head
The Criticality of Coding Sequelae (Late Effects)
A sequela is a residual condition that occurs after the acute phase of an illness or injury has ended. Common sequelae of TBI include:
-
Epilepsy and recurrent seizures (G40.-)
-
Hemiplegia/hemiparesis (G81.-)
-
Cognitive deficits and memory problems (R41.-)
-
Headaches (G44.-)
-
Personality and behavioral changes (F07.0)
-
Hydrocephalus (G91.-)
When coding a sequela, two codes are typically used:
-
The sequela code itself (e.g.,
G40.509– Epilepsy, unspecified, not intractable, without status epilepticus). -
The old injury code with the 7th character S (e.g.,
S06.5X1S– Sequelae of traumatic subdural hemorrhage with loss of consciousness).
This pairing tells the complete story: the current problem is a direct result of a past injury.
7. The Art of Sequencing: Primary Diagnosis, Comorbidities, and Complications
The order in which codes are listed, known as sequencing, is crucial. The primary diagnosis is the condition chiefly responsible for the patient’s encounter. For an initial ER visit following a car accident, the most severe intracranial injury (e.g., S06.5X1A) would be the primary diagnosis. Associated injuries like a skull fracture or open wound would be listed as secondary diagnoses.
For a subsequent encounter focused on rehab for hemiparesis caused by the old TBI, the sequela code (G81.94 – Hemiplegia, unspecified, affecting left dominant side) might be the primary diagnosis, followed by the old injury code with the ‘S’ 7th character.
Complications arising during treatment (e.g., a hospital-acquired pneumonia) are also coded and sequenced appropriately based on the focus of care.
8. Case Studies: Applying Codes in Real-World Scenarios
Case Study 1: The Weekend Warrior’s Concussion
-
Scenario: A 22-year-old male is checked hard during an ice hockey game. He stumbles off the ice, is confused and reports “seeing stars.” He does not lose consciousness. He is evaluated in the ER. Diagnosis: Concussion without loss of consciousness.
-
Coding:
-
Primary Diagnosis:
S06.0X9A(Concussion without loss of consciousness, initial encounter) -
External Cause:
Y93.64(Activity, ice hockey) ANDW21.03XA(Struck by hockey stick, initial encounter) – Note: Multiple external cause codes can be used.Y92.810(Place, ice hockey rink) could also be added. -
Sequencing: S06.0X9A is primary as it’s the reason for the visit.
-
Case Study 2: The Complex Fall of an Elderly Patient
-
Scenario: An 80-year-old female with osteoporosis trips on a rug at home and falls, hitting her head. She is briefly dazed but does not lose consciousness. A CT scan in the ER reveals a small, acute right-sided subdural hemorrhage. She is admitted for observation.
-
Coding:
-
Primary Diagnosis:
S06.5X0A(Traumatic subdural hemorrhage without loss of consciousness, initial encounter) -
Secondary Diagnosis:
S02.0XXA(Fracture of vault of skull, initial encounter) – If a fracture is documented. -
External Cause:
W18.09XA(Other fall on same level, initial encounter) ANDY92.009(Place, unspecified house) ANDY93.H9(Activity, other activity involving property and land maintenance, building, and repair) – if she was, for example, vacuuming. -
Note: Her osteoporosis (
M81.0– Age-related osteoporosis without current pathological fracture) is a contributing factor and should be coded as well, as it provides important clinical context.
-
Case Study 3: The Multi-Trauma Motor Vehicle Accident
-
Scenario: A 35-year-old driver is in a high-speed head-on collision. He is extracted from the vehicle with a GCS of 7. CT scans show a traumatic subarachnoid hemorrhage, diffuse cerebral edema, and a left tibia/fibula fracture. He is intubated and taken emergently to the OR for his leg.
-
Coding:
-
Primary Diagnosis:
S06.1X1A(Traumatic cerebral edema with loss of consciousness, initial encounter) – *This is chosen over S06.6X- as cerebral edema is often considered more severe and life-threatening.* -
Secondary Diagnoses:
-
S06.6X1A(Traumatic subarachnoid hemorrhage with LOC, initial encounter) -
S82.202A(Unspecified fracture of shaft of left fibula, initial encounter) -
S82.301A(Unspecified fracture of shaft of right tibia, initial encounter)
-
-
External Cause:
V43.52XA(Car driver injured in collision with car, initial encounter) ANDY92.410(Place, highway) – Intent is assumed unintentional.
-
9. The Why Behind the Code: Clinical, Financial, and Research Implications
Driving Reimbursement and Revenue Cycle Health
ICD-10 codes are the foundation of medical billing. They justify the medical necessity of the services provided (ER visit, CT scan, surgery, hospital stay). An incorrect or insufficiently specific code can lead to claim denials, delays in payment, and audits. For example, coding a simple concussion (S06.0X9A) will map to a lower-weighted DRG than coding a subdural hemorrhage requiring neurosurgical intervention (S06.5X1A), which accurately reflects the higher resource utilization and justifies greater reimbursement.
Informing Public Health Initiatives and Epidemiological Research
Public health agencies like the CDC rely on aggregated ICD-10 data to:
-
Track the incidence of TBIs nationally.
-
Identify high-risk populations (e.g., teenagers, elderly).
-
Monitor the effectiveness of prevention programs (e.g., helmet laws, fall prevention in seniors).
-
Understand the leading causes of TBI (e.g., has the opioid crisis led to an increase in fall-related TBIs?).
-
Allocate funding for research and support services.
Without accurate and specific coding, this data is flawed, and public health efforts are based on an incorrect understanding of the problem.
Supporting Quality of Care and Patient Outcomes
Accurate coding creates a robust and precise medical record. This allows for:
-
Improved Care Coordination: A future provider can instantly understand the severity and nature of a past TBI.
-
Outcomes Tracking: Hospitals can analyze data to see if patients with certain types of coded injuries have better or worse outcomes with different treatments.
-
Risk Adjustment: In value-based care models, accurate coding ensures a provider’s patient population is accurately assessed for acuity, so they are not penalized for treating sicker, more complex patients.
10. Best Practices and Common Pitfalls in TBI Coding
Best Practices:
-
Code to the Highest Specificity: Never use an “unspecified” code if the documentation supports a more specific one.
-
Query the Provider: If documentation is conflicting, incomplete, or unclear, initiate a formal physician query to obtain clarification.
-
Code All Associated Conditions: Remember to code fractures, open wounds, and any other related injuries.
-
Never Forget the 7th Character: Always append the correct 7th character (A, D, S).
-
Utilize External Cause Codes: Always assign external cause codes to complete the clinical picture, even if they are not required for reimbursement.
-
Stay Updated: Attend coding webinars, read newsletters, and review the official ICD-10-CM Guidelines and Coding Clinic updates annually.
Common Pitfalls:
-
Coding Both Concussion and a More Severe Injury: Remember the hierarchy; code only the more severe intracranial injury.
-
Misapplying the 7th Character: Using “A” for a follow-up visit where the patient is only receiving physical therapy for sequela (should be “D” or “S”).
-
Ignoring Laterality: For skull fractures and other lateralized injuries, failing to specify right, left, or bilateral.
-
Under-coding Sequelae: Failing to link long-term neurological problems back to the original TBI.
11. The Future: A Glimpse at ICD-11
The WHO’s ICD-11 came into effect in January 2022, though the US is years away from implementing a clinical modification (ICD-11-CM). ICD-11 features a more modern, digital-friendly structure and offers even greater detail in some areas. For TBI, it introduces new codes for more nuanced specifications, such as the type of post-traumatic amnesia and the inclusion of imaging findings directly in the code structure. The move to ICD-11 will represent another significant shift, requiring extensive coder education and system updates.
12. Conclusion
The ICD-10 coding system for traumatic brain injury is a complex but indispensable framework that translates clinical reality into a standardized data language. Mastery of codes like those in the S06 category, along with associated injuries, sequelae, and external causes, is not an administrative task but a critical clinical and operational competency. Accurate coding ensures appropriate reimbursement, fuels vital public health research, and creates a precise patient record that supports high-quality care across the entire continuum, from the emergency room to long-term rehabilitation. It is the silent, powerful narrative that tells the full story of an injury and its lasting impact.
13. Frequently Asked Questions (FAQs)
Q1: What is the most important thing to remember when coding a TBI?
A: The hierarchy rule: code only the most severe type of intracranial injury documented. A more severe injury (e.g., a hemorrhage) includes any less severe associated injuries (e.g., a concussion).
Q2: When do I use the 7th character ‘S’ for sequela?
A: Use ‘S’ when the patient is being treated for a late effect or residual condition that is a direct consequence of a past TBI (e.g., epilepsy, paralysis, cognitive deficits). You will use two codes: one for the sequela condition itself and the original injury code with the ‘S’ character.
Q3: Are external cause codes mandatory for billing?
A: While CMS and other payers may not always require them for reimbursement, they are mandatory for complete and accurate reporting per official ICD-10-CM guidelines. They are crucial for public health tracking and should always be used.
Q4: What should I do if the physician’s documentation is unclear?
A: You should never guess. Initiate a formal physician query process to ask for clarification in the medical record. This is a best practice that protects the coder, the provider, and the healthcare organization.
Q5: How often do ICD-10 codes change?
A: The ICD-10-CM code set is updated annually on October 1st. It is essential for coders to review the new guidelines, new codes, deleted codes, and revised code titles every year.
14. Additional Resources
-
Centers for Disease Control and Prevention (CDC) – TBI Division: Provides extensive clinical guidance, data, statistics, and educational materials for professionals and the public. https://www.cdc.gov/traumaticbraininjury
-
CMS ICD-10-CM Official Guidelines for Coding and Reporting: The definitive source for coding rules. Updated annually. https://www.cms.gov/medicare/coding-billing/icd-10-codes
-
American Health Information Management Association (AHIMA): The premier association for health information management professionals, offering certifications, education, and resources on coding best practices. https://www.ahima.org
-
American Academy of Professional Coders (AAPC): A leading organization for medical coders, providing certification, training, and local chapter networking. https://www.aapc.com
-
AHA Coding Clinic for ICD-10-CM/PCS: The official publication from the American Hospital Association that provides authoritative advice and guidance on specific coding scenarios. (Subscription required).
Date: September 18, 2025
Disclaimer: This article is intended for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or accurate medical coding. The codes and guidelines referenced are subject to change; always refer to the most current official ICD-10-CM manuals and updates from the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS).





