In the modern medical landscape, technology and precision are inextricably linked. Nowhere is this more evident than in the use of lasers, which have revolutionized treatment across numerous specialties, from ophthalmology to urology. The Neodymium-doped Yttrium Aluminum Garnet (Nd:YAG) laser stands as a pinnacle of this technological evolution, offering surgeons a tool of remarkable accuracy for a diverse range of procedures. It can delicately open a clouded membrane behind the lens of the eye to restore vision in a matter of minutes or precisely vaporize obstructive prostate tissue to alleviate urinary symptoms. This power, however, brings with it a parallel need for precision in a different language: the language of medical coding.
Accurate procedural coding using the Current Procedural Terminology (CPT®) system is the critical bridge between the advanced care provided by a clinician and the appropriate reimbursement from a payer. A misunderstanding or misapplication of a single digit in a CPT code can lead to claim denials, delayed payments, audits, and even compliance issues. This article serves as an exhaustive guide to demystifying the CPT codes associated with YAG laser procedures. We will move beyond simple code listings and delve into the nuances of documentation, modifier use, medical necessity, and the intricate guidelines that govern correct coding. Whether you are a seasoned coder, a practicing surgeon, a clinic administrator, or a billing specialist, mastering this information is essential for ensuring that the remarkable benefits of YAG laser technology are matched by equally remarkable administrative accuracy.
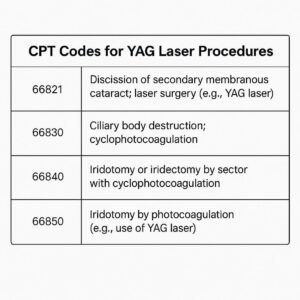
CPT Codes for YAG Laser Procedures
2. Understanding the YAG Laser: More Than Just a Beam of Light
Before assigning a code, it is imperative to understand the tool itself. The Nd:YAG laser is not a monolithic device; its application is defined by its unique physical properties and how they interact with human tissue.
The Science Behind Nd:YAG Laser Technology
The term “Nd:YAG” is an acronym describing its core components:
-
Nd (Neodymium): A rare-earth element that serves as the dopant or active medium. Its atoms are excited by an external light source (like a flashlamp) to produce laser light.
-
YAG (Yttrium Aluminum Garnet): A synthetic crystalline structure that hosts the neodymium atoms.
This laser produces light with a wavelength of 1064 nanometers, which lies in the near-infrared spectrum. This specific wavelength is crucial because it is poorly absorbed by pigments like melanin and hemoglobin but is highly absorbed by water only at very high power densities. This allows the YAG laser to perform its signature action: optical breakdown.
Instead of cutting or heating tissue like a CO2 laser, the focused YAG laser beam creates a microplasma at the target site. This plasma expansion creates a shockwave that mechanically disrupts, cuts, or vaporizes the tissue with minimal thermal damage to the surrounding areas. This photodisruptive property makes it ideal for procedures requiring precise, non-contact internal surgery, such as cutting a cloudy capsule in the eye or breaking up vitreous strands.
Key Ophthalmic and Surgical Applications
The YAG laser’s properties make it exceptionally useful in ophthalmology, but its applications extend far beyond:
-
Posterior Capsulotomy: Clearing opacification of the posterior lens capsule after cataract surgery.
-
Iridotomy: Creating a small hole in the peripheral iris to relieve pressure and treat or prevent angle-closure glaucoma.
-
Vitreolysis: Cutting vitreous strands or opacities that float in the visual axis (“floaters”).
-
Trabeculoplasty: Applying laser spots to the trabecular meshwork to improve aqueous outflow in open-angle glaucoma (though SLT uses a different type of YAG laser and is technically photochemical, not photodisruptive).
-
Dermatology: Vascular lesions, tattoo removal, hair removal, and skin rejuvenation.
-
Urology: Vaporization of the prostate (GreenLight laser, a KTP laser which is a frequency-doubled YAG laser) and lithotripsy (breaking up urinary stones).
-
Dentistry: Periodontal surgery and caries removal.
-
Otolaryngology: Treating vocal cord lesions and airway stenosis.
Understanding why a YAG laser is chosen for a specific procedure is the first step toward understanding how to code it correctly.
3. The Foundation: Navigating the CPT® Code Set and Its Guidelines
The CPT® code set, published and maintained by the American Medical Association (AMA), is the uniform language for describing medical, surgical, and diagnostic services. It is essential to remember that CPT codes are intellectual property of the AMA, and their use requires a license. Coding professionals must always work from the most current, official AMA CPT® manual.
Key principles for using CPT codes include:
-
Code to the Highest Specificity: Always choose the code that most accurately describes the procedure performed. Do not use a nonspecific code if a more specific one exists.
-
Follow Code Descriptors and Instructional Notes: The text beneath the code number (the descriptor) and any notes in the manual (e.g., “Do not report…”, “Use…in conjunction with…”) are mandatory guidelines.
-
Understand the Global Surgical Package: Most surgical codes include the procedure itself, local anesthesia, and immediate postoperative care. Understanding what is and isn’t included prevents unbundling (separately coding for services included in the primary code).
-
Comply with Payer-Specific Policies: While CPT is a national standard, Medicare Administrative Contractors (MACs) and private insurers often publish Local Coverage Determinations (LCDs) and policies that provide further instructions on coding and documentation requirements.
4. A Deep Dive into Common YAG Laser CPT® Codes
This section provides a detailed analysis of the most frequently reported YAG laser codes, their clinical context, and coding nuances.
CPT 66821: YAG Laser Capsulotomy (Posterior Capsulotomy)
-
CPT Descriptor: “Discission of posterior capsule of lens; laser surgery (e.g., YAG laser) (1 or more stages).”
-
Clinical Context: After cataract surgery, the natural lens is removed, but the thin, clear posterior capsule that supported it is left intact. In a significant percentage of patients, this capsule becomes cloudy over months or years, causing blurred vision similar to the original cataract. This is called Posterior Capsular Opacification (PCO). A YAG laser capsulotomy is a non-invasive procedure where the surgeon uses the laser to create a small central opening in this cloudy membrane, instantly restoring clear vision.
-
Coding Guidance:
-
This code is typically billed as a separate procedure from the original cataract surgery, as it often occurs months or years later.
-
It is reported once per eye, regardless of the number of laser pulses used to create the opening.
-
The code includes the laser procedure and the associated patient evaluation on the same day.
-
Crucially, it is not reported if performed in the postoperative period of the original cataract surgery unless it is for a rare complication like a capsular distension syndrome. If performed during the global period of the cataract surgery (typically 90 days), a modifier may be required to indicate the procedure is unrelated to the original surgery’s normal recovery (e.g., modifier -79, Unrelated Procedure or Service by the Same Physician During a Postoperative Period).
-
-
Documentation Requirements: The medical record must clearly document the presence of a visually significant PCO, a decrease in visual acuity, and patient symptoms (e.g., glare, halos). The note should state that a YAG laser capsulotomy was performed.
CPT 66711: YAG Laser Iridotomy
-
CPT Descriptor: “Ciliary body destruction; photocoagulation (one or more sessions) (transscleral or endoscopic).” Note: This is a common point of confusion. The correct code for a laser iridotomy is 65820.
-
CPT 65820 (Correct Code): “Incision of iris, laser (e.g., argon, YAG); without iridectomy.”
-
CPT 66711 is for cyclophotocoagulation, a completely different procedure used to destroy the ciliary body and reduce aqueous production in severe, end-stage glaucoma. Using 66711 for an iridotomy is a significant error.
-
-
Clinical Context: Laser Peripheral Iridotomy (LPI) is used to treat or prevent angle-closure glaucoma. In this condition, the drainage angle between the iris and cornea is physically blocked, causing a dangerous rise in intraocular pressure (IOP). The YAG laser is used to create a small hole in the peripheral iris, allowing aqueous fluid to flow from the posterior chamber to the anterior chamber, bypassing the pupil block and opening the angle.
-
Coding Guidance:
-
Report 65820 for the YAG laser iridotomy.
-
Code once per eye, per session. If multiple sessions are needed to achieve a patent iridotomy, it may be reported again, but documentation must support the medical necessity of the repeat procedure.
-
Modifier -50 (Bilateral Procedure) is applicable if performed on both eyes on the same day.
-
-
Documentation Requirements: The record must document the indication, such as narrow angles, appositional closure, elevated IOP, or acute angle-closure attack. Gonioscopy findings (visualization of the angle) are critical to support medical necessity.
CPT 65855: YAG Laser Vitreolysis
-
CPT Descriptor: “Vitreoretinal surgery; with laser photocoagulation.”
-
Clinical Context: This code is used when the YAG laser is employed to disrupt anterior vitreous strands that may be causing traction or opacities. A common application is for symptomatic vitreous floaters that significantly impair vision. It is important to distinguish this from pan-retinal photocoagulation (PRP) for diabetic retinopathy, which uses a different laser (e.g., argon) and is coded differently (67228).
-
Coding Guidance:
-
65855 is the correct code for YAG laser disruption of vitreous strands or opacities.
-
This is a highly specialized procedure, and its medical necessity is often scrutinized by payers. Documentation must be robust.
-
-
Documentation Requirements: The note should detail the patient’s symptomatic complaints, the vitreous opacities on examination (e.g., via slit lamp biomicroscopy), and how they directly affect activities of daily living. Pre- and post-procedure visual acuity should be recorded.
CPT 66030: YAG Laser Trabeculoplasty (Selective Laser Trabeculoplasty – SLT)
-
CPT Descriptor: “Trabeculoplasty by laser surgery.”
-
Clinical Context: This procedure is used to treat open-angle glaucoma. The laser (in this case, a Selective Laser Trabeculoplasty or SLT laser, which is a frequency-doubled Nd:YAG laser at 532 nm) is applied to the trabecular meshwork—the eye’s drainage system. The low-energy laser stimulates a biological response in these cells, improving the outflow of aqueous humor and reducing intraocular pressure.
-
Coding Guidance:
-
66030 is used for any type of laser trabeculoplasty, including Argon Laser Trabeculoplasty (ALT) and SLT.
-
It is typically performed on 180 degrees of the trabecular meshwork at a time.
-
It is coded once per eye per session, regardless of the number of laser applications.
-
-
Documentation Requirements: Document the type of glaucoma, baseline IOP, the reason for choosing laser therapy (e.g., intolerance to medications, desire to reduce medication burden), and the degree of angle treated.
Summary of Common Ophthalmic YAG Laser CPT Codes
| CPT Code | Procedure | Clinical Goal | Key Coding Consideration |
|---|---|---|---|
| 66821 | YAG Laser Capsulotomy | Restore vision after PCO | Do not report during global period of cataract surgery without a modifier. |
| 65820 | YAG Laser Iridotomy | Treat/prevent angle-closure glaucoma | Do not confuse with 66711 (cyclophotocoagulation). |
| 65855 | YAG Laser Vitreolysis | Disrupt symptomatic vitreous opacities | Medical necessity must be thoroughly documented. |
| 66030 | SLT (YAG) Trabeculoplasty | Lower IOP in open-angle glaucoma | Covers both ALT and SLT procedures. |
5. Beyond the Eye: YAG Laser Procedures in Other Specialties
The YAG laser’s versatility ensures its use across medicine.
Dermatology: CPT 17110 & 17111 (Destruction of Lesions)
-
Clinical Context: Lasers are workhorses in dermatology for destroying benign (e.g., sebaceous hyperplasia, warts, angiomas) and premalignant (e.g., actinic keratosis) lesions. The YAG laser, particularly in its long-pulsed mode, is effective for vascular lesions and hair removal.
-
Coding Guidance:
-
CPT 17110: “Destruction of benign lesions other than skin tags or cutaneous vascular proliferative lesions; up to 14 lesions.”
-
CPT 17111: “…15 or more lesions.”
-
Coding is based on the number of lesions destroyed, not the number of laser pulses. The code represents the entire session.
-
The code set includes destruction by any method, including laser, electrocautery, or cryotherapy.
-
For cutaneous vascular proliferative lesions (e.g., port-wine stains, hemangiomas), use codes 17106 (1-5 lesions) and 17107 (6-14 lesions) and 17108 (15 or more lesions).
-
Urology: CPT 52648 (Laser Vaporization of the Prostate)
-
Clinical Context: For men with Benign Prostatic Hyperplasia (BPH), laser enucleation or vaporization is a minimally invasive alternative to traditional surgery (TURP). The “GreenLight” laser is a KTP laser, which is a frequency-doubled Nd:YAG laser (532 nm wavelength) that is highly absorbed by hemoglobin, making it ideal for vaporizing the vascular prostate tissue.
-
Coding Guidance:
-
CPT 52648: “Laser vaporization of the prostate, including control of postoperative bleeding, complete (vasectomy, meatotomy, cystourethroscopy, urethral calibration and/or dilation, and internal urethrotomy are included).”
-
This is a comprehensive code that includes the entire surgical session and all the listed components. Do not report separate codes for cystoscopy or other included services.
-
This code is reported only once, regardless of the time or amount of tissue removed.
-
Otolaryngology and Other Applications
In ENT, a YAG laser can be used via a flexible or rigid scope to ablate lesions in the airway or on the vocal cords. The coding would fall under the endoscopic code for the anatomic site (e.g., 31541, Laryngoscopy, direct…with ablation…) with the laser being the method of ablation, not a separately coded service.
6. The Crucial Role of Modifiers: Telling the Complete Story
Modifiers are two-character suffixes appended to a CPT code to indicate that a service or procedure was altered in some way without changing the definition of the code itself. They are essential for providing context to payers.
-LT and -RT: Laterality is Non-Negotiable
-
Use: Append -LT (Left side) or -RT (Right side) to codes for procedures performed on paired organs (eyes, ears, kidneys, lungs, etc.).
-
Example: A YAG capsulotomy on the left eye is reported as 66821-LT.
-50: Bilateral Procedure
-
Use: Indicates that the same procedure was performed on both sides during the same operative session.
-
Example: If a surgeon performs SLT (66030) on both eyes during the same session, it is reported as 66030-50. Payer Note: Some payers prefer to see the code listed once with modifier -50, while others may want it listed on two lines with modifiers -RT and -LT. Always follow payer-specific billing guidelines.
-78 and -79: Unplanned and Related Procedures
-
-78 (Unplanned Return to the Operating Room): Used when a related procedure (e.g., a complication) is performed by the same physician during the postoperative period of the initial surgery. It signals that no global package payment should be made for the second procedure; only the intra-service work is billable.
-
-79 (Unrelated Procedure): Used when a procedure performed during a postoperative global period is unrelated to the original surgery. For example, a YAG capsulotomy (66821) performed 45 days after cataract surgery would typically need modifier -79 appended (66821-79) to indicate it is not a normal part of the cataract surgery follow-up care.
-51 and -59: Multiple Procedures and Distinct Services
-
-51 (Multiple Procedures): Applied to the second and subsequent procedures performed during the same session. It informs the payer to apply a multiple procedure reduction (often 50% to the technical component of the secondary procedures). Most modern billing software automatically applies this modifier.
-
-59 (Distinct Procedural Service): Used to identify procedures/services that are not normally reported together but are appropriate under the circumstances. It indicates that the procedure was distinct or independent from other services performed on the same day. Its use is highly scrutinized. A more specific “X” modifier (XE, XS, XP, XU) is now often preferred to provide more detail.
7. Documentation: The Bedrock of Accurate Coding and Reimbursement
The medical record is the foundation of every claim. Without clear, complete, and contemporaneous documentation, accurate coding is impossible, and the claim is vulnerable to denial.
Key Elements for a Successful YAG Laser Claim:
-
History & Medical Necessity: Document the patient’s symptoms, their duration, and how they impact functional vision or quality of life. Note any prior treatments tried and failed.
-
Examination Findings: Record precise visual acuity, IOP measurements, and detailed slit lamp findings. For capsulotomy: “3+ PCO obscuring view of the posterior segment.” For iridotomy: “Shallow anterior chambers with appositionally closed angles on gonioscopy.”
-
Procedure Note: Must include:
-
Informed consent obtained.
-
Anesthesia used (e.g., topical proparacaine).
-
Laser used (e.g., Nd:YAG).
-
Settings (e.g., power, number of pulses).
-
Anatomic location treated.
-
Description of the procedure itself and the endpoint (e.g., “A central opening approximately 3mm in diameter was created with 32 pulses.”).
-
Any complications and how they were managed.
-
Patient tolerance of the procedure.
-
-
Post-Procedure Instructions: Given to the patient regarding medications (e.g., topical steroid drops) and follow-up.
8. Navigating Medical Necessity and Avoiding Denials
Payers only reimburse for services they deem “reasonable and necessary.”
Crafting Bulletproof Diagnoses
The ICD-10-CM diagnosis code must align perfectly with the CPT procedure code.
-
For 66821 (Capsulotomy): The best code is H26.4- (After-cataract). Use additional digits to specify the type (e.g., H26.41, Soemmering’s ring). Avoid using Z96.1 (Presence of intraocular lens) as a primary diagnosis, as it describes a status, not a disease.
-
For 65820 (Iridotomy): Codes from category H40.0- (Glaucoma with angle-closure) are appropriate, such as H40.02 (Primary angle-closure glaucoma, chronic) or H40.03 (Primary angle-closure glaucoma, acute).
-
For 66030 (SLT): Use codes for H40.1- (Open-angle glaucoma).
Understanding Local Coverage Determinations (LCDs)
An LCD is a decision by a Medicare MAC about whether a service is reasonable and necessary. They often list:
-
Covered Diagnoses: The specific ICD-10 codes that support medical necessity.
-
Frequency Limitations: How often a service can be performed (e.g., capsulotomy is typically covered once per eye per lifetime).
-
Documentation Requirements: Specific elements that must be in the chart.
-
Coding: Always check the LCD for your geographic region before performing and billing a service.
9. The Coding Process: A Step-by-Step Workflow
-
Review the Encounter: Read the entire operative report and clinic note.
-
Abstract the Procedures: Identify all services performed.
-
Identify the Primary Code: Determine the main procedure (e.g., YAG capsulotomy).
-
Assign the CPT Code: Select the most specific code (66821).
-
Assign Modifiers: Append appropriate modifiers based on laterality, multiple procedures, or global period status (e.g., -LT).
-
Assign ICD-10-CM Codes: Link the most specific diagnosis code that justifies the procedure (e.g., H26.41).
-
Verify Medical Necessity: Cross-reference codes with payer policies and LCDs.
-
Submit the Claim: Transmit electronically via your practice management system.
10. Case Studies: Applying Knowledge to Real-World Scenarios
Case Study 1: The Bilateral Iridotomy
-
Scenario: A 65-year-old patient presents with narrow angles and elevated IOP in both eyes. The surgeon decides to perform prophylactic LPI on both eyes during the same visit.
-
Coding: 65820-50 (Laser iridotomy, bilateral procedure). Diagnosis: H40.03 (Primary angle-closure glaucoma, acute) or a code for narrow angle H40.03 or H40.022.
-
Rationale: Modifier -50 correctly indicates the procedure was performed on both eyes.
Case Study 2: Capsulotomy During the Global Period
-
Scenario: A patient had cataract surgery 30 days ago. They now present with significant visual blurring due to a clouded posterior capsule. The surgeon performs a YAG capsulotomy.
-
Coding: 66821-LT-79 (or -RT). Diagnosis: H26.41.
-
Rationale: Modifier -79 indicates this procedure was unrelated to the original cataract surgery. While PCO is a common long-term consequence, its treatment is not part of the 90-day global surgical package of the cataract extraction. Appending -79 prevents an automatic denial.
Case Study 3: SLT and Cataract Surgery
-
Scenario: A patient with glaucoma undergoing cataract surgery has SLT performed on the same eye during the same surgical session.
-
Coding: 66984 (Cataract surgery) and 66030-XS (SLT, separate structure). Diagnosis: H25.9 (Unspecified age-related cataract) and H40.11 (Primary open-angle glaucoma).
-
Rationale: Modifier -59 or, more specifically, -XS (Separate Structure) is used because the SLT is performed on the trabecular meshwork, a separate anatomical structure from the lens and capsule addressed by the cataract surgery. This indicates the procedures are distinct and both are billable.
11. The Future of YAG Laser Coding: Emerging Technologies and Trends
The field is not static. Coders must stay informed about:
-
New Laser Technologies: The development of femtosecond lasers for cataract surgery has already created new codes (e.g., 0191T). New wavelengths and laser delivery systems will continue to emerge.
-
New CPT Codes: The AMA CPT Editorial Panel constantly reviews and updates the code set. A new application for YAG laser may eventually warrant its own specific code.
-
Value-Based Care: The shift from fee-for-service to value-based reimbursement may change how these procedures are bundled and paid for, emphasizing outcomes over volume.
-
Increased Scrutiny and AI: Payers are using increasingly sophisticated artificial intelligence to audit claims. Accurate, precise coding supported by impeccable documentation is more important than ever.
12. Conclusion: Mastering the Code to Empower Patient Care
The precise application of a YAG laser can dramatically improve a patient’s quality of life, restoring vision or relieving debilitating symptoms. This clinical precision must be mirrored by an equally precise approach to medical coding. Understanding the nuances of CPT codes like 66821, 65820, and 66030, wielding modifiers correctly, and building claims on a foundation of robust documentation are not merely administrative tasks—they are essential components of ethical and sustainable medical practice. By mastering this complex language, coding professionals ensure that providers are reimbursed fairly for their expertise, allowing them to continue offering these transformative technologies to the patients who need them.
13. Frequently Asked Questions (FAQs)
Q1: Can I bill for a YAG laser capsulotomy if it’s performed by the same surgeon who did the original cataract surgery?
A: Absolutely. It is a separate procedure. The key is timing. If it is performed after the 90-day global period of the cataract surgery, bill it normally (66821-LT/RT). If it is performed during the global period, you must append modifier -79 to indicate it is an unrelated procedure.
Q2: What is the difference between CPT 66711 and 65820? This is very confusing.
A: This is a critical distinction.
-
65820 is for an iridotomy—creating a hole in the iris to improve fluid flow within the eye. It’s for angle-closure glaucoma.
-
66711 is for cyclophotocoagulation—destroying part of the ciliary body to reduce fluid production in the eye. It’s a destructive procedure for end-stage, uncontrolled glaucoma. Using 66711 for an iridotomy is a major coding error.
Q3: How many YAG laser codes can I bill for during one patient session?
A: You can bill for all medically necessary and distinct procedures. For example, if a patient has a capsulotomy in one eye (66821) and an SLT in the other (66030) during the same visit, you would bill both codes with the appropriate laterality modifiers. If two procedures are performed on the same eye (e.g., capsulotomy and vitreolysis), you would bill both and append modifier -59 (or a more specific X modifier) to the secondary procedure to show they are distinct.
Q4: My payer denied a claim for YAG vitreolysis (65855) as “not medically necessary.” What can I do?
A: This is common. File an appeal with strong clinical documentation. Include:
-
Patient’s subjective complaints detailing how the floaters significantly impair vision (e.g., inability to read, drive).
-
Objective findings (e.g., “dense, central vitreous opacity visible on slit lamp exam”).
-
Visual acuity tests.
-
A letter of medical necessity from the surgeon.
-
References to any supporting scientific literature or payer policies.
Q5: Are there specific consent forms needed for YAG laser procedures?
A: While not a coding requirement per se, informed consent is a critical medico-legal and clinical best practice. The consent form should specifically mention the laser procedure, its benefits, risks (e.g., elevated IOP, retinal detachment, inflammation), and alternatives. This strengthens the overall defensibility of the claim.
14. Additional Resources
-
The American Medical Association (AMA): For the official CPT® code set, guidelines, and updates. https://www.ama-assn.org
-
The American Academy of Ophthalmology (AAO): Offers coding guides, newsletters, and resources specific to eye care. https://www.aao.org
-
The Centers for Medicare & Medicaid Services (CMS): For Medicare coverage policies, LCDs, and NCDs. https://www.cms.gov
-
Your Medicare Administrative Contractor (MAC): Find your local MAC’s website for the most relevant LCDs and billing articles.
-
The American Health Information Management Association (AHIMA): A premier association for health information and coding professionals. https://www.ahima.org
-
The American Academy of Professional Coders (AAPC): Provides certification, training, and local chapter networking for coders. https://www.aapc.com





