In the intricate ecosystem of modern healthcare, communication is paramount. Clinicians, administrators, insurers, and researchers must speak a common, precise language to ensure patient safety, facilitate accurate reimbursement, and track public health trends. At the heart of this communication for hospital inpatient procedures in the United States lies a complex, yet elegantly logical, system: the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS). More than just a random string of letters and numbers, an ICD-10-PCS code is a rich, multi-layered narrative. It tells a complete story about a medical procedure: what was done, where it was done, why it was done, how the surgeon reached the site, what was used, and what was the ultimate objective.
This article serves as your definitive guide to deciphering this narrative. We will embark on a detailed journey through each of the seven characters that constitute an ICD-10-PCS code, moving beyond simple definitions to a deep, practical understanding. Whether you are a seasoned coder looking to refine your expertise, a healthcare administration student, a clinical professional seeking to understand the backend of patient records, or a curious individual fascinated by medical data, this exploration will equip you with the knowledge to comprehend the language of procedures. We will dissect the system’s architecture, unravel its most complex component—the root operation—and build codes from the ground up through real-world case studies. Prepare to unlock the secrets held within each character and appreciate the power of precision that ICD-10-PCS brings to healthcare.
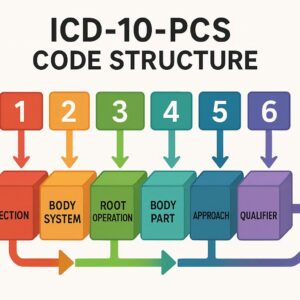
ICD-10-PCS Code Structure
2. The Foundation: Understanding the “Why” Behind ICD-10-PCS
To truly master ICD-10-PCS, one must first understand the problems it was designed to solve. Its predecessor for coding inpatient procedures, ICD-9-CM Volume 3, was a system showing its age. It was largely numeric, limited in scope, and unable to accommodate the rapid advancements in medical technology.
From ICD-9-CM Volume 3 to ICD-10-PCS: A Paradigm Shift
ICD-9-CM Volume 3 was running out of space. With a primarily decimal-based structure, it offered a limited number of available codes. This led to “lumping” dissimilar procedures together under a single code, which obscured clinical detail. For example, a single code might describe a type of repair, but it wouldn’t specify the approach (open vs. laparoscopic) or the specific device used. This lack of granularity had significant implications for data analysis, reimbursement accuracy, and tracking patient outcomes.
ICD-10-PCS was developed by the Centers for Medicare & Medicaid Services (CMS) as a complete replacement, built from the ground up with several key design objectives in mind:
-
Expandability: The alphanumeric structure (using both numbers and letters) provides a vastly larger pool of possible codes, ensuring the system can grow with medical innovation for decades to come.
-
Standardization and Consistency: Each code has a standardized, multi-axial structure. The meaning of a character is consistent across the system. For instance, the character ‘0’ in the Approach position always means “Open.”
-
Precision and Specificity: The seven-character format forces a level of detail that was impossible in ICD-9-CM. Every aspect of the procedure must be specified, creating a complete and unambiguous clinical picture.
-
Uniqueness: The goal is for each code to represent a single, unique procedure. This eliminates ambiguity and ensures that data extracted from the codes is clean and analytically valuable.
3. The Architectural Blueprint: The 7-Character Alphanumeric Code
An ICD-10-PCS code is not a word; it is a coordinate. Each of its seven characters represents a specific piece of information, and its position within the code is fixed and meaningful. The structure can be visualized as follows:
[Section] [Body System] [Root Operation] [Body Part] [Approach] [Device] [Qualifier]
Each character can be a number (0-9) or a letter (A-H, J-N, P-Z, excluding O and I to avoid confusion with digits 0 and 1). This gives us 34 possible values for each character position (10 numbers + 24 letters). The potential combinations are virtually limitless, fulfilling the design goal of expandability.
4. Character 1: Section – The Universe of Procedures
The first character is the highest level of categorization. It defines the broad “universe” or general type of procedure performed. There are ten sections in ICD-10-PCS, with the “Medical and Surgical” section (character ‘0’) being the most frequently used.
-
0: Medical and Surgical – Procedures performed on the physiological body systems, typically involving cutting, inserting, removing, or altering tissue.
-
1: Obstetrics – Procedures related to pregnancy, childbirth, and the puerperium.
-
2: Placement – Procedures for placing devices, appliances, or materials into body regions and orifices for immobilization, protection, or other purposes (e.g., casting, splinting, traction).
-
3: Administration – Procedures for introducing therapeutic, prophylactic, or diagnostic substances into the body (e.g., intravenous infusion, vaccination).
-
4: Measurement and Monitoring – Procedures for determining the level of physiological or physical function (e.g., cardiac stress test, electroencephalogram).
-
5: Extracorporeal Assistance and Performance – Procedures for temporarily taking over the function of a physiological system (e.g., hemodialysis, cardiac bypass).
-
6: Extracorporeal Therapies – Procedures that utilize equipment outside the body to perform therapies on body fluids (e.g., shockwave lithotripsy, ultraviolet light therapy).
-
7: Osteopathic – Osteopathic manipulative treatment.
-
8: Other Procedures – Miscellaneous procedures that do not fit into the other sections (e.g., acupuncture, resuscitation).
-
9: Chiropractic – Chiropractic manipulative treatment.
For the remainder of this article, we will focus primarily on the Medical and Surgical section, as it is the most complex and illustrative of the system’s principles.
5. Character 2: Body System – Pinpointing the Anatomical Region
The second character refines the location from the general section to the specific body system upon which the procedure was performed. This character’s meaning is dependent on the Section from Character 1. For example, in the Medical and Surgical section (0), the value ‘H’ represents the “Skin and Breast” body system, while in the Obstetrics section (1), ‘H’ represents the “Pregnancy” body system.
Common Body System values in the Medical and Surgical Section include:
-
0: Central Nervous System and Cranial Nerves
-
2: Heart and Great Vessels
-
3: Upper Arteries
-
4: Lower Arteries
-
5: Veins
-
7: Gastrointestinal System
-
8: Hepatobiliary System and Pancreas
-
9: Skin, Subcutaneous Tissue and Breast
-
B: Endocrine System
-
C: Eye
-
D: Ear, Nose, Sinus
-
F: Respiratory System
-
G: Mouth and Throat
-
H: Urinary System
-
J: Female Reproductive System
-
K: Male Reproductive System
-
L: Musculoskeletal System
-
N: Hernia Body System (A unique body system specifically for hernia repair)
-
P: Lymphatic and Hemic Systems
6. Character 3: Root Operation – The Core of the Procedure
This is the most critical and often the most challenging character to master. The Root Operation defines the objective or the intent of the procedure. It answers the question, “What was the provider trying to accomplish?” There are 31 distinct root operations in the Medical and Surgical section. Misidentifying the root operation is the most common source of coding errors, as it fundamentally changes the entire code.
To make this manageable, we can group the 31 root operations into logical categories based on their objective.
Groups of Root Operations: Taking Out vs. Putting In
-
Excision (B): Cutting out or off, without replacement, a portion of a body part. The body part is not the entire organ. (e.g., liver biopsy, polyp removal).
-
Resection (T): Cutting out or off, without replacement, all of a body part. (e.g., total colectomy, total nephrectomy).
-
Destruction (5): Eradicating a portion of a body part without physical removal, using methods like ablation, cautery, or fulguration. No specimen is sent to pathology.
-
Extraction (D): Pulling out or off all or a portion of a body part by the use of force. The key is the use of force. (e.g., suction D&C, removal of a foreign body).
-
Drainage (9): Taking or letting out fluids and/or gases from a body part. (e.g., incision and drainage of an abscess, thoracentesis).
-
Transplantation (Y): Putting in or on all or a portion of a living body part from a person or animal to physically take the place and/or function of all or a portion of a similar body part. (e.g., kidney transplant, heart transplant).
-
Reattachment (M): Putting back in or on all or a portion of a separated body part to its normal location or other suitable location. (e.g., reattachment of a finger).
-
Insertion (H): Putting in a non-biological device that remains after the procedure is completed. (e.g., inserting a central venous catheter, inserting a pacemaker).
-
Replacement (R): Putting in or on a device that replaces a body part that may have been taken out or whose function has permanently ceased. (e.g., total hip replacement, mitral valve replacement with a prosthetic valve).
-
Supplement (U): Putting in or on a device that reinforces or augments a body part without replacing the body part. The body part remains in place. (e.g., hernia repair with mesh, spinal fusion with hardware).
-
Restriction (V): Partially closing the orifice or lumen of a tubular body part. (e.g., tubal ligation, gastroesophageal fundoplication).
-
Occlusion (L): Completely closing the orifice or lumen of a tubular body part. (e.g., endovascular embolization of an artery).
-
Dilation (7): Expanding an orifice or lumen of a tubular body part. (e.g., percutaneous transluminal angioplasty, esophageal dilation).
Groups of Root Operations: Altering Diameter and Routes
-
Bypass (1): Altering the route of passage of the contents of a tubular body part. This can be done by rerouting to a different downstream site, rerouting to an upstream site, or rerouting to a completely different body system. (e.g., coronary artery bypass graft, gastric bypass for obesity).
-
Division (8): Cutting into a body part without draining fluids and/or gases or removing a portion of it. The goal is to separate or transverse the body part’s entirety. (e.g., severing a nerve to relieve pain, division of spinal nerve root).
Groups of Root Operations: Defining Objectives of Procedures
-
Inspection (J): Visually and/or manually exploring a body part. No interventions are performed. (e.g., diagnostic laparoscopy, exploratory thoracotomy).
-
Map (K): Locating the route of passage of electrical impulses and/or functional areas in a body part. (e.g., cardiac electrophysiological study).
-
Control (3): Stopping, or attempting to stop, post-procedural or other acute bleeding. This is used only as the sole procedure performed or when the control of bleeding is the only procedure performed in an anatomical region. (e.g., controlling bleeding at a surgical site via suture ligature).
-
Repair (Q): Restoring, to the extent possible, a body part to its normal anatomical structure and function. Used only when no other, more specific root operation applies (e.g., suturing a laceration).
-
Fusion (G): Joining together portions of an articular body part, rendering the articular body part immobile. (e.g., spinal fusion, ankle arthrodesis).
-
Alteration (S): Modifying the anatomical structure of a body part without affecting its function, and done for aesthetic purposes. (e.g., breast augmentation, face lift).
-
Creation (4): Making a new structure or a structure that did not exist previously. This is only used for sex-change operations. (e.g., creation of a vagina in a male-to-female transgender patient).
* Common Root Operation Pairs – Distinguishing Between Similar Objectives*
| Root Operation Pair | Key Distinguishing Factor | Example 1 | Example 2 |
|---|---|---|---|
| Excision (B) vs. Resection (T) | Portion vs. All of the body part. | Excision: Partial nephrectomy (only part of the kidney is removed). | Resection: Total nephrectomy (the entire kidney is removed). |
| Excision (B) vs. Destruction (5) | Specimen sent to pathology? | Excision: Polypectomy with specimen sent for analysis. | Destruction: Fulguration of a skin lesion; no tissue is sent to pathology. |
| Insertion (H) vs. Replacement (R) | Is a native body part being replaced? | Insertion: Putting in a chemotherapy port; no body part is being replaced. | Replacement: Total knee arthroplasty; the native knee joint is replaced. |
| Restriction (V) vs. Occlusion (L) | Partially vs. Completely closed. | Restriction: Tubal ligation; the fallopian tubes are partially closed. | Occlusion: Fallopian tube embolization; the tubes are completely closed. |
| Bypass (1) vs. Dilation (7) | Rerouting vs. Expanding the existing route. | Bypass: Coronary artery bypass graft; blood is rerouted around a blockage. | Dilation: Coronary angioplasty; the blocked artery is expanded with a balloon. |
7. Character 4: Body Part – The Specific Site of Action
The fourth character specifies the precise body part where the root operation was performed. This is where ICD-10-PCS achieves its renowned granularity. The body part values are specific to the Body System (Character 2) and the Root Operation (Character 3). For example, the body part “Liver” is broken down into:
-
Liver (general)
-
Right Lobe of Liver
-
Left Lobe of Liver
-
Hepatic Duct, Right
-
Hepatic Duct, Left
Accurate coding requires the coder to carefully review the operative report to identify the exact body part documented by the physician.
8. Character 5: Approach – The Pathway to the Procedure
The fifth character defines the approach, or the technique used to reach the site of the procedure. This is a crucial differentiator, as the same root operation on the same body part can have different codes based on the approach, reflecting significant differences in resource utilization and patient recovery.
-
0: Open – Cutting through the skin or mucous membrane and other body layers to expose the site of the procedure.
-
3: Percutaneous – Entry by puncture or minor incision of the skin, mucous membrane, or other body layers, with the use of guide wires, catheters, and/or endoscopic assistance. The procedure is performed under imaging guidance.
-
4: Percutaneous Endoscopic – Entry by puncture or minor incision of the skin, mucous membrane, or other body layers, with the use of an endoscope for visualization and instrumentation. This is the approach for most laparoscopic procedures.
-
7: Via Natural or Artificial Opening – Entry through a natural orifice (e.g., mouth, urethra) or a stoma.
-
8: Via Natural or Artificial Opening Endoscopic – Entry through a natural orifice or stoma with the use of an endoscope (e.g., colonoscopy, cystoscopy).
-
F: Via Natural or Artificial Opening with Percutaneous Endoscopic Assistance – A hybrid approach (e.g., laparoscopically assisted vaginal hysterectomy).
-
X: External – Procedures performed directly on the skin or mucous membrane; procedures that are performed by application of external force through the skin (e.g., closed reduction of a fracture, external beam radiation).
9. Character 6: Device – What is Left Behind
The sixth character specifies the device that remains in the patient after the procedure is completed. This is a key component for tracking implants and understanding the nature of the intervention. If no device is left behind, this character is coded as Z: No Device.
The Device character is tightly linked to the Root Operation and Body Part. ICD-10-PCS uses “Device Aggregation Tables” which list the general type of device used. For example, the table for the body part “Knee Joint” under root operations like Replacement or Supplement includes values like:
-
J: Synthetic Substitute
-
K: Nonautologous Tissue Substitute
-
Z: No Device
It is critical to note that the device character does not specify the brand, model, or material of the device (e.g., it’s “Synthetic Substitute,” not “Smith & Nephew Genesis Total Knee Prosthesis, Cobalt-Chromium”).
10. Character 7: Qualifier – The Finishing Nuance
The seventh and final character is the qualifier. It provides additional information that further specifies an attribute of the procedure that is not captured in the other six characters. Its meaning is highly context-dependent.
Examples include:
-
Diagnostic vs. Therapeutic: In the root operation Inspection (J), the qualifier can be X: Diagnostic or other values.
-
Type of Tissue: In Bypass (1) procedures, the qualifier can specify the type of conduit used, such as Autologous Venous Tissue, Autologous Arterial Tissue, or Synthetic Substitute.
-
Specific Qualifier: For a Dilation (7) of a coronary artery, the qualifier Drug-eluting Intraluminal Device specifies that a drug-eluting stent was used.
11. Practical Application: Building a Code Step-by-Step
Let’s apply our knowledge by building codes for common procedures.
Case Study 1: Laparoscopic Cholecystectomy
-
Operative Report: The surgeon performs a laparoscopic removal of the gallbladder for cholelithiasis.
-
Character 1 (Section): This is a procedure on the physiological body system. 0 – Medical and Surgical
-
Character 2 (Body System): The gallbladder is part of the hepatobiliary system. F – Hepatobiliary System and Pancreas
-
Character 3 (Root Operation): The entire gallbladder is being cut out. This is T – Resection.
-
Character 4 (Body Part): The specific body part is the Gallbladder.
-
Character 5 (Approach): The procedure was performed laparoscopically. 4 – Percutaneous Endoscopic
-
Character 6 (Device): No device is left behind. Z – No Device
-
Character 7 (Qualifier): No further qualification is needed. Z – No Qualifier
Final ICD-10-PCS Code: 0FT44ZZ – Resection of Gallbladder, Percutaneous Endoscopic Approach
Case Study 2: Percutaneous Coronary Intervention with Drug-Eluting Stent
-
Operative Report: The cardiologist accesses the femoral artery percutaneously, advances a catheter to the heart, inflates a balloon to dilate a blocked coronary artery, and places a drug-eluting stent.
-
Character 1 (Section): 0 – Medical and Surgical
-
Character 2 (Body System): The coronary arteries are part of the heart’s vessel system. 2 – Heart and Great Vessels
-
Character 3 (Root Operation): The objective is to expand the lumen of the artery. 7 – Dilation
-
Character 4 (Body Part): The specific artery treated (e.g., Coronary Artery, One Artery or a more specific branch).
-
Character 5 (Approach): Access was through a percutaneous puncture. 3 – Percutaneous
-
Character 6 (Device): A drug-eluting stent is an intraluminal device. J – Intraluminal Device
-
Character 7 (Qualifier): The stent is drug-eluting. 4 – Drug-eluting
Final ICD-10-PCS Code (example for one artery): 02703J4 – Dilation of Coronary Artery, One Artery, Percutaneous Approach, Intraluminal Device, Drug-eluting
Case Study 3: Open Reduction and Internal Fixation of a Femoral Fracture
-
Operative Report: The orthopedic surgeon makes an open incision to realign a fractured femur and applies a metal plate and screws to hold the bone in place.
-
Character 1 (Section): 0 – Medical and Surgical
-
Character 2 (Body System): The femur is part of the musculoskeletal system. L – Musculoskeletal System
-
Character 3 (Root Operation): The objective is to put in a device that helps bring the fragments together and immobilize the site. This is S – Supplement (putting in a device that reinforces the body part).
-
Character 4 (Body Part): Femoral Shaft (or a more specific part of the femur).
-
Character 5 (Approach): An open incision was made. 0 – Open
-
Character 6 (Device): A plate and screws are an Internal Fixation Device.
-
Character 7 (Qualifier): No further qualification. Z – No Qualifier
Final ICD-10-PCS Code (example for shaft): 0QS60ZZ – Supplement of Femoral Shaft with Internal Fixation Device, Open Approach
12. Beyond the Medical and Surgical Section: An Overview of Other Sections
While the Medical and Surgical section is the most complex, the principles of the multi-axial structure apply to all sections. For example:
-
Administration (Section 3): Character 2 is the Body System (e.g., Circulatory), Character 3 is the Root Operation (e.g., Introduction), Character 4 is the Body Part/Orifice (e.g., Peripheral Vein), Character 5 is the Approach (e.g., Percutaneous), Character 6 is the Substance (e.g., Anti-neoplastic), and Character 7 is the Qualifier (e.g., High-dose Interleukin).
-
Placement (Section 2): Character 3 is the Root Operation (e.g., Immobilization, Traction), Character 4 is the Body Region (e.g., Upper Arm), and Character 5 is the Device (e.g., Splint).
13. The Art and Science of PCS Coding: Common Challenges and Expert Tips
Coding is not a mechanical task; it requires analytical thinking and a deep understanding of medical terminology and anatomy.
-
Relying on the Index and Tables: Always start with the PCS Index, but never code directly from it. The Index is a guide. The final code must be verified and selected from the corresponding PCS Table.
-
The Importance of Physician Documentation: The coder is entirely dependent on the clarity and completeness of the physician’s operative report. Queries are essential if documentation is ambiguous or lacking.
-
Avoiding Assumptions in Root Operation Selection: Do not assume the root operation based on the common name of the procedure. A “bypass” in common parlance might be a Bypass, Dilation, or Restriction in PCS. Always refer back to the definitions of the 31 root operations.
14. Conclusion: The Power of Precision
The ICD-10-PCS system, with its structured seven-character framework, transforms complex medical procedures into a standardized, precise language. Mastering the nuances of each character—especially the critical root operation—is fundamental to accurate coding. This precision is the bedrock of reliable healthcare data, driving appropriate reimbursement, advancing clinical research, and ultimately, improving patient care.
15. Frequently Asked Questions (FAQs)
Q1: Can a single surgical session have multiple ICD-10-PCS codes?
A: Absolutely. If multiple, distinct procedures are performed on different body parts or involving different root operations, each procedure should be coded separately. For example, a patient undergoing a laparoscopic cholecystectomy (0FT44ZZ) and a laparoscopic appendectomy (0DTJ4ZZ) during the same operation would have both codes.
Q2: How do I code a procedure where the intended root operation changes?
A: You code the procedure that was actually completed. For example, if a surgeon begins a laparoscopic cholecystectomy (Resection) but encounters severe adhesions and must convert to an open procedure to control bleeding (Control), you would code the open control of bleeding as the primary procedure if that was the only one completed.
Q3: What is the difference between the “Device” character and the “Qualifier” when both seem to describe a device?
A: The Device (Character 6) is the general category of device left in the body. The Qualifier (Character 7) provides a further attribute of that device or the procedure. In the coronary stent example, the Device is “Intraluminal Device” (J), and the Qualifier specifies it is “Drug-eluting” (4).
Q4: Where can I find the official coding guidelines?
A: The official ICD-10-PCS Coding Guidelines are updated annually by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). They are available on the CMS website.
16. Additional Resources
-
Centers for Medicare & Medicaid Services (CMS) ICD-10 Website: The primary source for official files, guidelines, and updates.
-
American Health Information Management Association (AHIMA): Offers a wealth of educational resources, practice exercises, and industry news for coding professionals.
-
American Academy of Professional Coders (AAPC): Provides certification, training, and networking opportunities for medical coders.
-
ICD-10 Code Browser Tools: Several online platforms (e.g., FindACode.com, ICD10Data.com) offer searchable browsers that can help visualize the PCS tables and their relationships.
Date: November 20, 2025
Author: The Medical Coding Insights Team
Disclaimer: The information contained in this article is for educational and informational purposes only and is not a substitute for professional medical coding advice, consultation, or training. Coding professionals must always rely on the most current, official ICD-10-PCS coding guidelines, manuals, and reference materials provided by the Centers for Medicare & Medicaid Services (CMS) and the Centers for Disease Control and Prevention (CDC). The authors and publishers are not responsible for any errors, omissions, or for any outcomes related to the use of this information.





