In the high-stakes realm of neurosurgery, few conditions present a more immediate and complex challenge than a bleeding cerebral arteriovenous malformation (AVM). This pathological tangle of blood vessels is a ticking time bomb within the brain, and its rupture is a life-threatening neurological emergency. As neurosurgeons navigate the delicate landscape of the human brain to obliterate this threat, their work is meticulously documented. This documentation becomes the raw material for another critical profession: the medical coder. The translation of a complex surgical procedure into the precise, alphanumeric language of ICD-10-PCS (International Classification of Diseases, Tenth Revision, Procedure Coding System) is not merely an administrative task; it is a fundamental process that impacts patient care records, reimbursement, research data, and hospital analytics. A single misstep in code selection can distort the clinical narrative, leading to financial loss for the healthcare facility and muddying the epidemiological data used to advance medical science. This article aims to be the definitive guide for medical coders, health information management (HIM) professionals, and coding students seeking to master the intricate process of accurately coding the surgical management of a bleeding cerebral AVM. We will embark on a detailed journey, dissecting the pathology, the surgical techniques, and the granular structure of ICD-10-PCS to build codes that are both technically accurate and clinically coherent.
ICD-10-PCS Coding for the Surgical Management of a Bleeding Cerebral Arteriovenous Malformation
2. Understanding the Pathology: What is a Cerebral AVM and Why Does it Bleed?
To code a procedure correctly, one must first understand the underlying disease. A cerebral Arteriovenous Malformation (AVM) is a congenital disorder, meaning it is present at birth, characterized by a complex, tangled web of abnormal blood vessels connecting arteries and veins in the brain. It is often described as a “bag of worms” due to its appearance.
In a normal circulatory system, oxygen-rich blood flows from the heart through thick-walled, high-pressure arteries, which gradually branch into smaller arterioles and then into microscopic capillaries. It is within these capillaries that the vital exchange of oxygen and nutrients for carbon dioxide and waste products occurs. The now oxygen-poor blood then drains into thin-walled, low-pressure venules and veins, returning it to the heart and lungs.
An AVM disrupts this elegant process entirely. It bypasses the capillary bed, creating a direct connection, called a fistula, between cerebral arteries and veins. This has two critical consequences:
-
High-Pressure Blood Shunting: Blood rushes directly from the high-pressure arterial system into the low-pressure venous system without the buffering effect of capillaries.
-
Structural Weakness: The veins subjected to this abnormal, high-pressure flow become dilated and tortuous, forming the nidus (the core of the malformation). These vessels are structurally abnormal, with thin, weak walls that lack the normal muscular and elastic layers.
The constant stress of high-pressure blood flow makes the AVM nidus highly susceptible to rupture. A rupture, or hemorrhage, leads to bleeding into the brain tissue (intracerebral hemorrhage), the spaces surrounding the brain (subarachnoid hemorrhage), or the ventricles (intraventricular hemorrhage). This event is a stroke, and its effects can be devastating, causing sudden severe headache, seizures, neurological deficits like weakness or speech problems, and even death. The primary goal of treatment for a ruptured AVM is to prevent re-bleeding, which carries a significantly high risk in the first year after the initial hemorrhage.
3. The Clinical Landscape: Diagnosis and Treatment Modalities for a Ruptured AVM
When a patient presents with symptoms suggestive of an intracranial hemorrhage, a rapid diagnostic workup is initiated. This typically involves neuroimaging studies:
-
Non-Contrast Head CT Scan: This is the first and fastest test to confirm the presence of acute bleeding.
-
CT Angiography (CTA) or MR Angiography (MRA): These specialized scans use contrast dye to visualize the blood vessels in the brain and are highly effective at identifying the AVM, defining its size, location, and feeding arteries/draining veins.
-
Digital Subtraction Angiography (DSA): This is the gold standard for AVM diagnosis. It is an invasive procedure where a catheter is threaded into the arteries supplying the brain, and contrast is injected while taking X-ray images. DSA provides the most detailed map of the AVM’s angioarchitecture, which is crucial for planning treatment.
The management of a ruptured AVM is multifaceted and often involves a combination of the following modalities, decided by a multidisciplinary team of neurosurgeons, interventional neuroradiologists, and radiation oncologists.
-
Microsurgical Resection: This is the classic “open surgery” approach. A neurosurgeon performs a craniotomy (opening the skull) and uses an operating microscope and specialized instruments to meticulously dissect and remove the entire AVM nidus. This offers the advantage of immediate cure if complete resection is achieved.
-
Endovascular Embolization: An interventional neuroradiologist threads a microcatheter from an artery in the groin up into the precise arteries feeding the AVM. Through this catheter, liquid embolic agents (like Onyx or n-BCA glue) or coils are deployed to block off the blood vessels within the AVM. Embolization is rarely curative on its own for large AVMs but is often used pre-operatively to reduce blood flow and size, making surgical resection safer, or as a palliative measure.
-
Stereotactic Radiosurgery (SRS): This is a non-invasive treatment that uses highly focused, high-dose beams of radiation (e.g., Gamma Knife, CyberKnife) targeted precisely at the AVM nidus. The radiation causes the abnormal vessels to thicken and close off gradually over 1-3 years. It is typically reserved for small, deep-seated AVMs that are too risky for surgery. It is not suitable for an active, life-threatening hemorrhage as its effect is delayed.
4. Introduction to ICD-10-PCS: The Foundation of Procedural Coding
ICD-10-PCS is a multi-axial procedural classification system used in inpatient hospital settings in the United States. Unlike its diagnosis counterpart (ICD-10-CM), which is derived from the World Health Organization’s system, PCS was developed by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). Its structure is entirely logical and built on seven characters, each representing an aspect of the procedure. Every character’s value must be specified to create a complete and valid code.
The seven characters represent:
-
1st Character: Section (e.g., Medical and Surgical, Placement, etc.)
-
2nd Character: Body System (e.g., Central Nervous System, Peripheral Nervous System)
-
3rd Character: Root Operation (The objective of the procedure)
-
4th Character: Body Part (The specific site of the procedure)
-
5th Character: Approach (How the surgeon accessed the site)
-
6th Character: Device (Any device left in place)
-
7th Character: Qualifier (A further specification, if needed)
For a bleeding AVM, the procedure will almost always fall under the Medical and Surgical section on the Central Nervous System.
5. Deconstructing the AVM Repair: The Pivotal Choice of Root Operation
The most critical and often challenging step in coding an AVM procedure is selecting the correct Root Operation. The root operation defines the goal of the procedure. For AVM repair, the two primary contenders are Extirpation and Excision. The clinical documentation is key to making this distinction.
5.1. Root Operation: Extirpation – The Primary Choice
The official definition of Extirpation is: Taking or cutting out solid matter from a body part. The PCS guidelines further clarify that the solid matter may be an abnormal physical byproduct of a biological function (like a thrombus or calculus) or a foreign body. Most importantly, the guidelines explicitly state that the root operation Extirpation is used for procedures in which the sole objective is to take out or eliminate solid matter from the body part, and the solid matter is not a device.
A bleeding AVM is a solid, abnormal structure (the nidus) that is the source of the pathological condition. The objective of microsurgical resection is to “take out” this solid matter from the brain tissue. Therefore, the root operation Extirpation (code value B) is the most appropriate and commonly used selection for the open surgical resection of a cerebral AVM.
5.2. Root Operation: Excision – A Less Common but Valid Alternative
The official definition of Excision is: Cutting out or off, without replacement, a portion of a body part. The PCS guidelines specify that the qualifier DIAGNOSTIC is used to identify excision procedures that are biopsies.
For an AVM, if the documentation indicates that only a portion of the AVM was removed—for example, a surgeon biopsies a small piece of the malformation for pathological confirmation but does not attempt a curative resection—then the root operation Excision (code value B) would be correct. However, in the context of treating a ruptured AVM, the goal is typically complete removal, making Extirpation the far more likely choice.
5.3. Comparative Table: Extirpation vs. Excision for AVM
The following table provides a clear comparison to aid in root operation selection.
| Feature | Root Operation: Extirpation | Root Operation: Excision |
|---|---|---|
| Definition | Taking or cutting out solid matter from a body part. | Cutting out or off, without replacement, a portion of a body part. |
| Application to AVM | Removal of the entire AVM nidus (the solid matter) from the brain. | Removal of only a portion of the AVM nidus. |
| Clinical Goal | Curative treatment; elimination of the pathological entity. | Typically diagnostic (biopsy) or partial/debulking procedure. |
| Analogy | Removing a tumor (the solid matter) from an organ. | Taking a biopsy sample from a lesion. |
| ICD-10-PCS Character 3 | B | B (Yes, the same character value, but defined by the intent and documentation) |
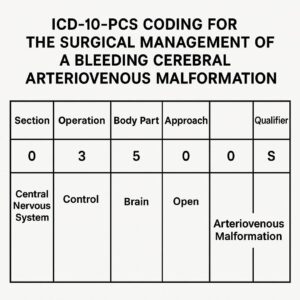
6. Building the Code: A Step-by-Step Walkthrough of the 7 Characters
Let’s construct a PCS code for a typical scenario: Craniotomy for microsurgical resection of a ruptured AVM in the right parietal lobe.
1st Character – Section: 0
-
Explanation: “0” represents the Medical and Surgical section, which encompasses all invasive procedures performed for the purpose of cutting, removing, altering, or inserting.
2nd Character – Body System: 0
-
Explanation: “0” represents the Central Nervous System and Cranial Nerves. This is the correct body system for a procedure on the brain parenchyma, such as the parietal lobe.
3rd Character – Root Operation: B
-
Explanation: As established, “B” represents Extirpation—taking out the solid matter (the AVM nidus) from the brain part.
4th Character – Body Part: 8
-
Explanation: This character specifies the precise anatomical site. We must consult the PCS tables for the Central Nervous System body system. The value “8” corresponds to Parietal Lobe, Right. Other common values would be “7” for Parietal Lobe, Left; “A” for Frontal Lobe, Right; “B” for Frontal Lobe, Left; “C” for Temporal Lobe, Right; “D” for Temporal Lobe, Left; “F” for Occipital Lobe, Right; and “G” for Occipital Lobe, Left. Specificity is paramount.
5th Character – Approach: 0
-
Explanation: The approach describes the technique used to reach the procedure site. A craniotomy is an Open approach. The PCS definition of Open is: Cutting through the skin or mucous membrane and any other body layers necessary to expose the site of the procedure. The value for Open is “0”. Other approaches for different AVM treatments could be Percutaneous (3) for endovascular procedures or External (X) for radiosurgery.
6th Character – Device: Z
-
Explanation: This character identifies any device that remains in the body after the procedure is completed. In a straightforward AVM resection, no device is typically left behind. Therefore, we use the value “Z” which means No Device.
7th Character – Qualifier: Z
-
Explanation: The qualifier provides additional information about the procedure. For an Extirpation procedure in the central nervous system, no specific qualifier is needed for a standard resection. Thus, we use the value “Z” which means No Qualifier.
Complete ICD-10-PCS Code: 00B80ZZ
-
Decoded: Extirpation of matter from Right Parietal Lobe, Open Approach.
7. Illustrative Case Studies: Applying Knowledge to Real-World Scenarios
Case Study 1: Craniotomy for Microsurgical Resection of a Ruptured Parietal Lobe AVM
-
Operative Report Summary: The patient was taken to the OR for a right parietal craniotomy. The dura was opened, and the cortex was exposed. Under microscopic guidance, the feeding arteries to the AVM were identified and coagulated. The AVM nidus was then meticulously dissected from the surrounding brain parenchyma and removed in its entirety. The draining vein was then divided. Hemostasis was achieved, and the dura, bone flap, and scalp were closed in layers.
-
Coding Analysis:
-
Root Operation: The goal was to remove the solid AVM nidus. This is Extirpation (B).
-
Body Part: The procedure was performed on the Right Parietal Lobe (8).
-
Approach: A craniotomy was performed, which is an Open (0) approach.
-
-
ICD-10-PCS Code: 00B80ZZ – Extirpation of matter from Right Parietal Lobe, Open Approach.
Case Study 2: Endovascular Embolization of a Bleeding Cerebellar AVM
-
Operative Report Summary: The patient underwent cerebral angiography confirming a ruptured AVM in the left cerebellar hemisphere supplied by the left Posterior Inferior Cerebellar Artery (PICA). A microcatheter was navigated via femoral artery access into the left PICA and then selectively into the feeding pedicle of the AVM. Under fluoroscopic guidance, a liquid embolic agent (Onyx) was injected, successfully obliterating a significant portion of the AVM nidus.
-
Coding Analysis:
-
Root Operation: The objective is not to “take out” matter but to occlude the lumen of the vessel. The root operation is Occlusion (L) – Completely closing an orifice or the lumen of a tubular body part.
-
Body System: This is still the Central Nervous System (0) as we are occluding an intracranial artery.
-
Body Part: The specific body part is the artery being occluded. We must find the correct code for the Left Posterior Inferior Cerebellar Artery. In the PCS table, this is body part value 6 (Posterior Inferior Cerebellar Artery, Left).
-
Approach: The catheter was inserted through the skin percutaneously. This is a Percutaneous (3) approach.
-
Device: A liquid embolic agent (Onyx) is considered an Intraluminal Device (6) that remains in the vessel.
-
-
ICD-10-PCS Code: 03L63CZ – Occlusion of Left Posterior Inferior Cerebellar Artery with Intraluminal Device, Percutaneous Approach. (Note: The 7th character Z is “No Qualifier” for this table).
Case Study 3: Stereotactic Radiosurgery for a Deep-Seated Ruptured AVM
-
Procedure Note Summary: A patient with a small, recently ruptured AVM in the left thalamus was deemed a poor candidate for surgery. The patient underwent Gamma Knife radiosurgery. A stereotactic head frame was placed, and high-resolution MRI was obtained for targeting. A high dose of radiation was precisely focused on the AVM nidus.
-
Coding Analysis:
-
Section: Radiosurgery falls under the Radiation Therapy section, not the Medical and Surgical section. The section character is D.
-
Body System: The body system is Central Nervous System (0).
-
Root Operation: The objective is to destroy the AVM tissue using ionizing radiation. The root operation is Beam Radiation (0).
-
Body Part: The target is the Thalamus. In the Radiation Therapy tables for the CNS, the value for Thalamus is 1 (for unilateral; if bilateral, specific codes exist).
-
Modality: This is Stereotactic Radiosurgery (Y).
-
Isotope/Qualifier: For Stereotactic Radiosurgery, the 6th character (Isotope) is Z (None), and the 7th character (Qualifier) is Z (No Qualifier).
-
-
ICD-10-PCS Code: D001ZZ – Beam Radiation of Thalamus using Stereotactic Radiosurgery.
8. Common Pitfalls and Coding Challenges: Avoiding Costly Errors
-
Confusing Extirpation and Excision: As detailed, this is the most common error. Always ask: “Was the goal to remove the entire abnormal solid matter (Extirpation) or just a piece of it (Excision)?”
-
Incorrect Body Part Assignment: The brain is highly specific in PCS. Confusing the frontal lobe with the parietal lobe, or failing to specify laterality, results in an incorrect code. Coders must have a detailed anatomical understanding.
-
Misidentifying the Approach for Endovascular Procedures: A common mistake is to code an endovascular embolization as an “Open” approach. Access is via a percutaneous puncture of the femoral artery, making the approach Percutaneous (3). The passage of the catheter through the body to the brain site is inherent in the procedure definition.
-
Coding the Repair and Not the Objective: Do not code the craniotomy (cutting the skull) as the primary procedure. The craniotomy is the approach for the root operation (Extirpation). The root operation defines the procedure’s objective.
-
Overlooking Combined Procedures: A patient may undergo pre-operative embolization followed by surgical resection during the same inpatient stay. Both procedures should be coded. The embolization would be coded as an Occlusion, and the resection would be coded as an Extirpation.
9. The Role of Documentation and Physician Queries
The coder is entirely dependent on the clarity and completeness of the physician’s operative report. Vague terms like “AVM was treated” are insufficient. The documentation must clearly state:
-
The specific anatomical location of the AVM (e.g., “right frontal lobe”).
-
The intent and nature of the procedure (e.g., “the AVM nidus was completely resected” or “a biopsy of the lesion was taken”).
-
The surgical approach (e.g., “a standard pterional craniotomy was performed”).
-
Any devices used and left in place (e.g., “the aneurysm clip was applied…”).
If the documentation is unclear, ambiguous, or conflicting, the coder’s duty is to initiate a physician query. This is a formal process of seeking clarification from the provider to ensure the codes assigned accurately reflect the patient’s clinical picture and the care provided.
10. Conclusion: Summarizing the Content of the Article in Three Lines
Accurate ICD-10-PCS coding for a bleeding AVM hinges on a deep understanding of both the clinical pathology and the logical structure of the coding system. The critical decision point is the selection of the root operation, where Extirpation is typically used for curative resection and Occlusion for endovascular embolization. Mastery requires meticulous attention to the operative report, precise anatomical knowledge, and a disciplined, step-by-step approach to building all seven characters of the code.
11. Frequently Asked Questions (FAQs)
Q1: What is the ICD-10-PCS code for clipping a feeding artery aneurysm associated with an AVM?
A1: This is a different procedure. Clipping an aneurysm involves placing a clip around the neck of the aneurysm to exclude it from circulation. The root operation is Restriction (V) – Partially closing an orifice or the lumen of a tubular body part. The device is an Intraluminal Device (6) (the clip). The code would be built from the Occlusion/Restriction table for the specific artery (e.g., 00V60ZZ for Restriction of Right Internal Carotid Artery, Open Approach).
Q2: How do I code an AVM resection that uses neuromonitoring or intraoperative MRI?
A2: Neuromonitoring and intraoperative imaging are considered integral components of the primary surgical procedure and are not coded separately. The code for the root operation (e.g., Extirpation) encompasses all the techniques used to perform that procedure safely and effectively.
Q3: The surgeon documented “debulking of the AVM.” What root operation do I use?
A3: “Debulking” typically implies a partial removal. In this case, the root operation Excision (cutting out a portion of a body part) is likely more appropriate than Extirpation. However, a query may be necessary to confirm if the intent was to remove the entire solid matter (the nidus) but it was described as “debulking,” or if a deliberate, less-than-total removal was performed.
Q4: What is the diagnosis code for a ruptured AVM?
A4: While this article focuses on PCS, the corresponding ICD-10-CM diagnosis code would be I60.8 – Other subarachnoid hemorrhage. You would also assign a code from category Q28.2 – Arteriovenous malformation of cerebral vessels to specify the underlying cause. Always follow the ICD-10-CM Official Guidelines for Coding and Reporting regarding sequencing.
Date: November 20, 2025
Author: Jonathan Reed, CCS, CDIP
Disclaimer: This article is intended for educational purposes and to illustrate professional coding concepts. It is not a substitute for the official ICD-10-PCS guidelines, coding manuals, or clinical documentation. Coders must always rely on the most current year’s official resources and the specific patient medical record to assign codes.





