In the intricate world of healthcare, the journey of a patient from diagnosis to treatment is meticulously documented, not just in clinical notes, but in a universal language of codes. For the patient undergoing a colostomy—a life-altering procedure that creates a new pathway for waste elimination—this coding is far more than an administrative formality. It is the definitive, data-driven story of their surgical encounter. The International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) provides the lexicon for this story, demanding a level of precision that directly impacts hospital reimbursement, public health data, and the quality of patient care records. This article delves deep into the art and science of ICD-10-PCS coding for colostomy procedures. We will move beyond simple code lookup and embark on a detailed exploration of how to accurately translate the nuanced actions of a surgeon into the structured, seven-character codes that define the procedure. Whether you are a seasoned medical coder, a healthcare administration student, or a clinical professional seeking to understand the downstream effects of your documentation, this guide aims to be your definitive resource, ensuring that every character in the code tells the true and complete story of the colostomy.
ICD-10-PCS code for colostomy procedures
2. Understanding the Colostomy: A Clinical Foundation for Coders
Before a single character of an ICD-10-PCS code can be assigned, a foundational understanding of the procedure itself is paramount. Coding in a vacuum, without clinical context, is a direct path to error.
What is a Colostomy and Why is it Performed?
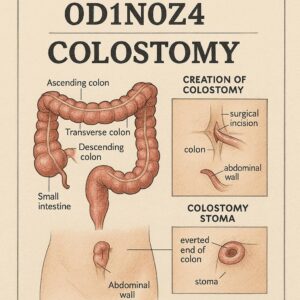
A colostomy is a surgical procedure that brings a portion of the large intestine (the colon) through the abdominal wall to create a stoma. This stoma serves as a new anus, through which stool and gas exit the body into a removable, external pouching system (ostomy bag). The need for a colostomy arises when a portion of the colon or rectum must be bypassed or rested due to disease, injury, or congenital defect.
Common indications include:
-
Colorectal Cancer: Often requires resection of a tumor, and a colostomy may be created to allow the downstream anastomosis (surgical connection) to heal.
-
Diverticulitis: Severe inflammation or perforation of diverticula (small pouches in the colon wall) may necessitate a temporary colostomy to divert stool away from the diseased area.
-
Inflammatory Bowel Disease (IBD): In cases of severe Crohn’s disease or ulcerative colitis that do not respond to medication, a colostomy may be part of the treatment.
-
Bowel Obstruction: A colostomy can relieve a blockage that cannot be resolved otherwise.
-
Trauma: Severe injury to the abdomen or rectum may require a colostomy to allow healing.
-
Fecal Incontinence: When other treatments fail, a colostomy can provide a solution for uncontrolled bowel movements.
Anatomical Landmarks: The Colon Segments
The specific part of the colon used for the stoma is critical for accurate coding and has direct implications for the patient’s outcome, as stool consistency varies along the colon’s length.
-
Ascending Colon: The first part of the colon, rising on the right side of the abdomen. Output is typically liquid.
-
Transverse Colon: The longest and most mobile part of the colon, running across the upper abdomen. Output is often pasty or semi-formed. This is a common site for temporary colostomies.
-
Descending Colon: Travels down the left side of the abdomen. Output is more formed.
-
Sigmoid Colon: The S-shaped final segment leading to the rectum. Output is typically solid, similar to normal stool. This is the most common site for permanent colostomies.
Temporary vs. Permanent Colostomies
This distinction, while crucial for patient counseling, is generally not directly specified in the ICD-10-PCS code. The code reflects the anatomical and procedural reality of the surgery. A “temporary” colostomy is often a loop colostomy (where a loop of colon is brought out) that is intended to be reversed later. A “permanent” colostomy is often an end colostomy (where the cut end of the colon is brought out), typically after a total proctocolectomy (removal of the colon and rectum). The permanence is inferred from the root operation and the body parts involved, not by a specific character in the code.
3. Deconstructing ICD-10-PCS: The Building Blocks of Precision
ICD-10-PCS is a multi-axial system where each character has a specific meaning, independent of the others. This structure allows for immense specificity.
The Seven-Character Alphanumeric System
Each ICD-10-PCS code is composed of seven characters, each representing an aspect of the procedure:
-
Character 1: Section – The broad category (e.g., Medical and Surgical).
-
Character 2: Body System – The general physiological system (e.g., Gastrointestinal System).
-
Character 3: Root Operation – The objective of the procedure (e.g., Bypass, Resection).
-
Character 4: Body Part – The specific anatomical site (e.g., Transverse Colon).
-
Character 5: Approach – The technique used to reach the site (e.g., Open, Percutaneous).
-
Character 6: Device – Any device that remains after the procedure (e.g., a stoma).
-
Character 7: Qualifier – Additional information about the procedure (e.g., the destination of a bypass).
The Medical and Surgical Section (0)
All colostomy procedures fall within the Medical and Surgical section, which is identified by the character 0 in the first position.
4. The Heart of the Matter: Identifying the Correct Root Operation
The third character, the Root Operation, is the most critical and often the most challenging component of ICD-10-PCS coding for colostomies. The intent of the procedure, as documented by the surgeon, dictates the root operation.
Bypass (1): Diverting the Flow of Contents
The root operation Bypass is defined as “altering the route of passage of the contents of a tubular body part.” This is the most common root operation for a classic colostomy creation.
-
Key Concept: The colostomy “bypasses” the downstream colon and rectum. The contents of the colon are rerouted from the stoma to the external environment.
-
PCS Guideline Reference: The official guidelines state that “procedures on a tubular body part… in which the contents of the tubular body part are diverted to an external opening are coded to the root operation Bypass.” The qualifier (7th character) is used to specify the destination, which, for an external stoma, is Cutaneous.
-
Example: A loop transverse colostomy created to divert stool away from an inflamed area in the descending colon is coded as a Bypass.
Excision (B): Cutting Out versus Cutting Off
The root operation Excision is defined as “cutting out or off, without replacement, a portion of a body part.” This is used when a stoma is created by cutting off a portion of the colon, but it is not the primary procedure for a standard colostomy.
-
Key Concept: The focus is on the removal of a portion of the colon, and the creation of the stoma is a consequence of that removal. It is often used for the creation of an “end colostomy” where the distal stump is oversewn and left in the abdomen (a Hartmann’s procedure).
-
Distinction from Resection: If the cut-off portion is only a component and not the entire body part, it is Excision. For example, cutting off the end of the colon to create a stoma, where the remaining colon is still largely intact, may be considered Excision.
Resection (T): Taking it All Out
The root operation Resection is defined as “cutting out or off, without replacement, all of a body part.” This is used when an entire specific segment of the colon is removed.
-
Key Concept: If the surgeon documents a “sigmoid colectomy” or “resection of the transverse colon,” the root operation is Resection. If an end colostomy is created from the proximal end as part of this procedure, the colostomy creation is inherent in the resection and is not coded separately. The stoma is the remaining end of the GI tract after the resection.
-
Example: A patient with rectal cancer undergoes an abdominoperineal resection (APR), where the sigmoid colon, rectum, and anus are removed. An end sigmoid colostomy is created. The correct code would be for the Resection of the sigmoid colon and rectum. The colostomy is not a separate bypass procedure; it is the natural result of the resection.
Drainage (9): The Role of Percutaneous Stomas
The root operation Drainage is defined as “taking or letting out fluids and/or gases from a body part.” This applies to a specific type of procedure: a percutaneous colostomy.
-
Key Concept: This is not a surgical colostomy. It is typically a radiologically guided procedure where a catheter is placed through the skin (percutaneous) into the colon to decompress a massive dilation (e.g., in toxic megacolon or an obstruction). The goal is purely to drain contents, not to permanently reroute the fecal stream.
-
Example: A tube cecostomy performed percutaneously to decompress the colon would be coded to Drainage.
Comparison Table: Root Operations for Colostomy-Related Procedures
| Root Operation | Definition | Clinical Example | Key Question to Ask |
|---|---|---|---|
| Bypass (1) | Altering the route of passage of contents. | Loop colostomy to divert stool from a distal obstruction or leak. | Is the colon intact, but we are rerouting its contents to a new outlet? |
| Excision (B) | Cutting out or off a portion of a body part. | Creation of an end colostomy (e.g., Hartmann’s procedure). | Are we cutting off a part of the colon to form the stoma, without removing the entire segment? |
| Resection (T) | Cutting out or off all of a body part. | Sigmoid colectomy with end colostomy. | Are we removing an entire segment of the colon, and the stoma is the new end? |
| Drainage (9) | Taking or letting out fluids and/or gases. | Percutaneous tube cecostomy for decompression. | Is this a minimally invasive procedure solely to drain the colon? |
5. Character by Character: Constructing the Complete Colostomy Code
With the root operation determined, we can now build the complete code.
-
Character 1: Section -> 0 (Medical and Surgical)
-
Character 2: Body System -> D (Gastrointestinal System)
-
Character 3: Root Operation -> 1 (Bypass), B (Excision), T (Resection), or 9 (Drainage) as determined above.
-
Character 4: Body Part -> This specifies the exact segment of colon where the procedure originated.
-
Ascending Colon -> C
-
Transverse Colon -> D
-
Descending Colon -> E
-
Sigmoid Colon -> F
-
Note: For a Bypass, this is the body part whose contents are being rerouted.
-
-
Character 5: Approach -> How the surgeon accessed the colon.
-
Open -> 0 (Through an incision)
-
Percutaneous -> 3 (Through the skin, e.g., for Drainage)
-
Percutaneous Endoscopic -> 4 (e.g., a laparoscopic-assisted colostomy)
-
Via Natural or Artificial Opening -> 7 (Rare for colostomy creation)
-
Via Natural or Artificial Opening Endoscopic -> 8 (Rare for colostomy creation)
-
-
Character 6: Device -> For a colostomy, this is almost always the 4 (
Synthetic Substitute) or 7 (Autologous Tissue Substitute) used to create the permanent opening (stoma). In ICD-10-PCS, the stoma itself is classified as a “device.”-
4 is used if the stoma is matured (sutured) to the skin without the use of the patient’s own tissue in a way that qualifies as “replacement.”
-
7 is used if a flap of the patient’s own skin or other tissue is used in the creation of the stoma. 4 is far more common.
-
Note: For a takedown (reversal) of a colostomy, the device character would be Z (No Device), as the stoma is being removed.
-
-
Character 7: Qualifier -> Provides essential context.
-
For a Bypass, the qualifier specifies the destination. For an external colostomy, this is always X (
Cutaneous). -
For an Excision or Resection that results in a colostomy, the qualifier is often X (
Cutaneous) to indicate the terminus is the skin. -
For a Drainage procedure, the qualifier is typically Z (No Qualifier).
-
6. Coding Scenarios: From Operative Report to Final Code
Let’s apply this knowledge to realistic operative reports.
Scenario 1: Loop Transverse Colostomy for Diverticulitis
-
Operative Note: “The patient was taken to the OR for a laparoscopic-assisted loop transverse colostomy for a diverticular abscess with a persistent colonic leak. The transverse colon was identified laparoscopically. A small incision was made, and a loop of transverse colon was exteriorized. The colon was opened and matured to the skin with interrupted sutures to create a stoma.”
-
Code Breakdown:
-
Root Operation: The colon is intact; we are rerouting its contents to a new, external opening. This is a Bypass (1).
-
Body Part: The procedure is on the Transverse Colon (D).
-
Approach: Laparoscopic-assisted means the primary access was via a scope. This is Percutaneous Endoscopic (4).
-
Device: The stoma was matured to the skin. This is a Synthetic Substitute (4).
-
Qualifier: The destination is the skin, so Cutaneous (X).
-
-
Final ICD-10-PCS Code: 0D1D4ZX
Scenario 2: End Sigmoid Colostomy with Resection for Rectal Cancer
-
Operative Note: “The patient underwent a low anterior resection for rectal cancer. The sigmoid colon and upper rectum were mobilized and resected. The distal rectum was stapled closed. The proximal end of the sigmoid colon was brought out through a separate incision in the left lower quadrant and matured as an end colostomy.”
-
Code Breakdown:
-
Root Operation: The surgeon resected (removed) the sigmoid colon and rectum. This is a Resection (T). Do not code a separate Bypass. The colostomy is the natural endpoint of the resected tract.
-
Body Part: We need to code the resection of all involved body parts. This requires multiple codes.
-
Code 1: Resection of Sigmoid Colon (F).
-
Code 2: Resection of Rectum (L).
-
-
Approach: Likely Open (0) or Percutaneous Endoscopic (4), depending on the technique. Let’s assume Open.
-
Device: For a Resection, the device character is Z (No Device), as we are removing, not putting in a device.
-
Qualifier: The qualifier for a Resection of the GI tract that terminates at the skin is X (Cutaneous).
-
-
Final ICD-10-PCS Codes: 0DTF0ZX (Resection of Sigmoid Colon, Open, Cutaneous) and 0DTL0ZX (Resection of Rectum, Open, Cutaneous).
Scenario 3: Take-Down (Reversal) of a Colostomy
-
Operative Note: “The patient was taken for a colostomy takedown. The stoma was circumscribed and dissected free from the abdominal wall. The loop of transverse colon was identified. The stoma was resected, and a functional end-to-end anastomosis was performed to restore bowel continuity.”
-
Code Breakdown:
-
Root Operation: We are taking down the stoma (the “device”) and reconnecting the bowel. The root operation is Bypass (1) again, but this time we are reversing the previous bypass.
-
Body Part: The body part is the Transverse Colon (D).
-
Approach: Open (0).
-
Device: We are removing the stoma. Therefore, the device is Z (No Device).
-
Qualifier: The destination is no longer the skin, but another part of the GI tract. In this case, it’s the Colon (7).
-
-
Final ICD-10-PCS Code: 0D1D0Z7 (Bypass, Transverse Colon, Open, No Device, to Colon).
Scenario 4: Percutaneous Colostomy for Decompression
-
Operative Note: “Under fluoroscopic guidance, a needle was introduced percutaneously into the cecum. A guidewire was placed, the tract was dilated, and a 12-French locking pigtail catheter was placed for decompression of the dilated colon.”
-
Code Breakdown:
-
Root Operation: The goal is to let out gas and fluid. This is Drainage (9).
-
Body Part: The procedure is on the Cecum (B).
-
Approach: Percutaneous (3).
-
Device: A drainage catheter is placed. This is a Drainage Device (0).
-
Qualifier: Z (No Qualifier).
-
-
Final ICD-10-PCS Code: 0D9B3ZZ
7. Common Pitfalls and Expert Tips for Accuracy
-
Pitfall 1: Assuming all colostomies are Bypass. Always read the operative report. If a resection is performed, the root operation is Resection.
-
Pitfall 2: Confusing Excision and Resection. If the entire anatomical body part (e.g., the entire sigmoid colon) is removed, it’s Resection. If only a portion is cut off to form the stoma, and the rest of the segment remains, it may be Excision.
-
Pitfall 3: Misidentifying the Approach. A laparoscopic-assisted procedure is “Percutaneous Endoscopic,” not “Open.”
-
Pitfall 4: Forgetting the Device Character for a Takedown. When taking down a colostomy, the device is “Z” (No Device), not “4” (Synthetic Substitute).
-
Tip: Query the Physician. If the documentation is unclear regarding the intent (bypass vs. resection) or the specific colon segment, a query is the best practice to ensure accuracy.
8. The Broader Impact: Why Accurate Colostomy Coding Matters
Accurate ICD-10-PCS coding is not an abstract exercise; it has tangible consequences.
-
Reimbursement and Revenue Cycle: MS-DRGs (Medicare Severity-Diagnosis Related Groups) are heavily influenced by procedure codes. An inaccurate code can place the patient in an incorrect DRG, leading to significant underpayment or denial of claims.
-
Healthcare Data Analytics and Public Health: These codes are aggregated to understand surgical trends, outcomes, and the prevalence of conditions requiring colostomies. Inaccurate data skews this research and can impact public health planning and funding.
-
Compliance and Audit Risk: Incorrect coding is a compliance risk that can lead to audits, fines, and reputational damage for healthcare providers.
9. Conclusion
Mastering ICD-10-PCS coding for colostomy procedures requires a symbiotic understanding of clinical medicine and coding principles. The journey from operative report to final code hinges on accurately identifying the surgeon’s intent, captured by the root operation. By meticulously building the code character by character—paying close attention to the body part, approach, and the crucial role of the device and qualifier—coders can ensure the patient’s record is a precise and reliable data point. This precision safeguards the financial health of the institution and, most importantly, contributes to the integrity of the healthcare data ecosystem.
10. Frequently Asked Questions (FAQs)
Q1: How do I code a Hartmann’s procedure?
A Hartmann’s procedure involves the resection of a portion of the colon (often sigmoid) with the creation of an end colostomy and closure of the rectal stump. You would code the Resection of the specific colon segment (e.g., 0DTF0ZX for Resection of Sigmoid Colon). The colostomy is inherent and not coded separately.
Q2: What is the difference between a colostomy and an ileostomy in ICD-10-PCS?
The body system (Character 2) and body part (Character 4) are different. An ileostomy involves the small intestine (Body System: D, but body parts like J for Ileum). The root operation logic (Bypass, Resection) remains the same.
Q3: Why is the stoma considered a “device” in ICD-10-PCS?
ICD-10-PCS defines a device broadly as “materials implanted or incorporated into the body for therapeutic, prosthetic, or diagnostic purposes.” The surgically created stoma, which is an artificial opening, fits this definition as it is incorporated to serve a therapeutic function.
Q4: How do I code a colostomy that is created during trauma surgery for a colon injury?
It depends on the action taken. If the colon is injured and a loop colostomy is created to divert stool without resecting the injured segment, it is a Bypass. If the injured segment is resected and an end colostomy is created, it is a Resection.





