In the intricate ecosystem of the human body following surgery or trauma, the Jackson-Pratt (JP) drain is a humble yet vital device. This simple closed-suction system, with its perforated tube and collapsible bulb, plays a critical role in preventing the accumulation of serum, blood, or pus, thereby facilitating healing and preventing infection. For the clinical team, it’s a tool of paramount importance. For the inpatient medical coder, however, it represents a labyrinth of procedural classification challenges within the ICD-10-PCS system. The act of placing, managing, or removing this drain is not captured by a single, straightforward code. Instead, it demands a nuanced understanding of root operations, body part specificity, and the procedural context—a puzzle where a misinterpretation can lead to significant reimbursement and compliance implications. This article serves as a detailed map through this labyrinth. We will deconstruct the JP drain from a coder’s perspective, explore the foundational principles of ICD-10-PCS that govern its classification, and provide a step-by-step guide to accurate coding for every phase of its lifecycle, from insertion to removal, including the management of complications. By mastering the minutiae of this common device, coders can ensure precision, support clinical documentation integrity, and uphold the financial integrity of their healthcare organizations.
ICD-10-PCS code for Jackson-Pratt drains
Chapter 1: Deconstructing the Device: What is a Jackson-Pratt Drain?
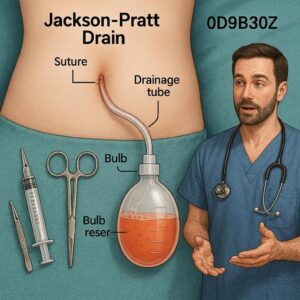
Before assigning a code, a coder must understand the “what” and “why” of a device. The Jackson-Pratt drain is a closed-wound drainage system, distinct from open systems like Penrose drains. Its primary components are:
-
A Perforated Silicone Tube: One end of this tube is placed inside the surgical site or wound cavity. It has multiple perforations (holes) to allow fluid to enter.
-
A Connector Tube: This connects the perforated tube to the bulb.
-
A Collapsible Plastic Bulb (Reservoir): This bulb is compressed (evacuated of air) before use and creates negative pressure (suction) when released. This suction draws fluid from the wound bed, through the tube, and into the bulb.
The clinical indications for a JP drain are numerous and directly influence the body part character of the ICD-10-PCS code. Common reasons for placement include:
-
Preventing Seroma/Hematoma: After procedures like mastectomies, abdominoplasties, or large flap surgeries, the body can produce excess serum or blood that collects in dead space.
-
Draining Established Collections: For an abscess, hematoma, or infected fluid collection identified via imaging.
-
Controlling Output from Anastomoses: In gastrointestinal or vascular surgery, a drain may be placed near a new connection to monitor for and control any potential leak.
-
Managing High-Output Wounds: In cases of fistulas or complex wounds with significant exudate.
This understanding is crucial. A drain placed in the breast tissue post-mastectomy is fundamentally different, from a coding perspective, than one placed in the pelvic cavity after a proctectomy.
Chapter 2: The Foundation of ICD-10-PCS: A Brief Primer for the Procedural Coder
ICD-10-PCS is a multi-axial system where each character in a 7-character code has a specific meaning. For procedures related to devices like JP drains, the first three characters (the Section, Body System, and Root Operation) are the most critical.
-
Character 1: Section: This identifies the general type of procedure. For JP drains, the two relevant sections are:
-
0: Medical and Surgical
-
2: Placement
-
-
Character 2: Body System: This refers to the general physiological system (e.g., Hepatobiliary System, Skin and Breast, Musculoskeletal System).
-
Character 3: Root Operation: This is the objective of the procedure—the definitive, overarching goal. Understanding the root operation is the single most important step in accurate JP drain coding. We will explore the relevant ones in detail in the next chapter.
-
Characters 4-7: These specify the Body Part, Approach, Device, and Qualifier, adding layers of specificity.
Chapter 3: Coding the Placement of a JP Drain (The “Root Operation” Conundrum)
This is the core of the challenge. There is no “JP Drain Placement” code. The correct code depends entirely on the intent of the procedure as documented by the physician.
Option 1: The Medical and Surgical Section (Section 0)
Within this section, two root operations are primary candidates.
-
Root Operation: Insertion
-
Definition: Putting in a non-biological appliance that remains in the body after the procedure is complete. The device is being put in, but the act of putting it in is not the therapeutic goal itself.
-
Application to JP Drain: This is used when the drain is placed prophylactically—to prevent a potential fluid collection. The device is the focus. For example, placing a JP drain in the breast bed during a mastectomy to prevent a seroma.
-
Code Structure:
0(Med/Surg) –H(Skin & Breast) –H(Insertion) – [Body Part, e.g.,9Right Breast] – [Approach] –J(Drainage Device) –Z(No Qualifier). -
Example Code:
0HH9XJZ– Insertion of Drainage Device into Right Breast, External Approach.
-
-
Root Operation: Drainage
-
Definition: Taking or letting out fluids and/or gases from a body part. The objective is the removal of the material, not the device. The device is merely the tool.
-
Application to JP Drain: This is used when the procedure’s primary goal is to evacuate an existing, identified fluid collection, such as an abscess or hematoma. The focus is on the “draining” action.
-
Code Structure:
0(Med/Surg) –9(Urinary System) –9(Drainage) – [Body Part, e.g.,KPerivesical Tissue] – [Approach] –Z(No Device) –Z(No Qualifier). -
Critical Note: For the Root Operation Drainage, the device (the JP drain) is not coded. The PCS Official Guidelines state that the device value “Z No Device” is used for drainage procedures, as the drainage is the objective, not the device left in place. This is a key distinction from Insertion.
-
Example Code:
099KXZZ– Drainage of Perivesical Tissue, External Approach.
-
Option 2: The Placement Section (Section 2)
-
Root Operation: Placement
-
Definition: Putting in a device that acts on a body region/orifice for the purpose of immobilizing, positioning, or moving body parts. The devices in this section are primarily things like traction apparatus, splints, and packs. The guidelines are very specific.
-
Application to JP Drain: The use of the Placement section for drains is a point of confusion. According to the ICD-10-PCS Official Coding Guidelines, “Procedures typically considered part of the operative package (e.g., insertion of a drain at the end of a procedure) are not coded separately.” However, if a drain is placed using the Placement section, it is generally for a packing or tamponade effect (e.g., to control bleeding by pressure), not for suction drainage. For a standard JP drain used for suction, the Medical and Surgical section is almost always the correct choice. Coders should be cautious and default to Section 0 unless the physician’s documentation explicitly supports a “placement” for immobilization/positioning, which is rare for a JP drain.
-
Case Study: Differentiating Root Operations
-
Scenario A: A patient undergoes a total abdominal hysterectomy. At the end of the procedure, the surgeon places a JP drain in the pelvic cavity and documents, “JP drain placed to pelvis for post-op drainage.” This is prophylactic. The correct root operation is Insertion.
-
Code:
0WHGXJZ– Insertion of Drainage Device into Peritoneal Cavity, External Approach.
-
-
Scenario B: A patient presents with a large, symptomatic post-operative pelvic hematoma identified on CT scan. The surgeon performs a procedure to place a JP drain into this hematoma. The documentation states, “Percutaneous drain placed for evacuation of pelvic hematoma.” The objective is to drain the existing collection. The correct root operation is Drainage.
-
Code:
0W9GXYZ– Drainage of Peritoneal Cavity, Percutaneous Approach.
-
Chapter 4: The Nuances of the Body Part and Approach
Once the correct root operation is determined, the next challenge is specifying the body part and approach.
Body Part: The coder must identify the specific anatomical cavity or tissue space where the tip of the drain resides.
-
Subcutaneous Tissue: For a drain placed in the fat layer under the skin (e.g., after a lumpectomy), the body part is the specific subcutaneous tissue (e.g., Right Axilla, Right Upper Arm).
-
Breast Tissue: For a drain placed within the breast parenchyma itself.
-
Body Cavities: This requires greater specificity.
-
Peritoneal Cavity: For a general pelvic or abdominal drain.
-
Retroperitoneum: For a drain behind the peritoneal lining.
-
Pleural Cavity: For a chest tube (though a chest tube is a different device, the same root operation logic applies).
-
Specific Organs/Spaces: Liver, Spleen, Perivesical Tissue, etc.
-
Approach: How the drain is placed.
-
Open (0): The drain is placed through a surgically created incision (e.g., placed under direct vision at the end of an open laparotomy).
-
Percutaneous (3): The drain is placed through a puncture or minor incision of the skin, without direct visualization of the target site. Often guided by ultrasound or CT.
-
Percutaneous Endoscopic (4): The drain is placed percutaneously with the use of an endoscope for visualization.
Chapter 5: Beyond Placement: Coding Subsequent Management and Care
A JP drain is not a “place it and forget it” device. Subsequent care during the hospitalization may be codeable.
-
Irrigation (Root Operation: Irrigation): If the drain becomes clogged and the physician must irrigate it with fluid to re-establish patency, this is a separate procedure.
-
Code Structure:
0(Med/Surg) –[Body System]–[Irrigation]–[Body Part]–[Approach]–Z–Z. -
Example:
0W9G4ZZ– Irrigation of Peritoneal Cavity, Percutaneous Endoscopic Approach.
-
-
Replacement (Root Operation: Replacement): If one JP drain is removed and a new one is placed in the same tract during the same episode, this is a replacement. If the old drain is removed and a new one is placed in a different location, that constitutes a new “Insertion” or “Drainage” procedure.
-
Monitoring: The routine assessment, stripping of the tube, or emptying of the bulb by nursing staff is considered part of the daily patient care and is not coded as a separate procedure.
Chapter 6: Coding the Removal of a JP Drain
The removal of a JP drain is typically straightforward.
-
Root Operation: Removal
-
Definition: Taking out a device from a body part.
-
Application: This covers the simple pulling out of the drain, whether at the bedside or in an operating room.
-
Code Structure:
0(Med/Surg) –[Body System]–P(Removal) –[Body Part]–X(External) –J(Drainage Device) –Z. -
Example:
0WPGXJZ– Removal of Drainage Device from Peritoneal Cavity, External Approach.
-
Bundling Note: If the drain is removed during the same operative session in which it was placed (e.g., a short-term drain placed and removed during a single surgery), the removal is not coded separately. It is considered part of the procedure.
Chapter 7: Tackling Complications and Related Procedures
JP drains can be a source of complications, each requiring specific coding.
-
Occluded/Malfunctioning Drain: Code the intervention to fix it (e.g., Irrigation as described above). If it must be replaced, code the Removal of the old drain and the Replacement (or new Insertion) of the new one.
-
Drain Site Infection: This requires two codes:
-
An ICD-10-CM diagnosis code for the infection (e.g.,
T81.4XXA– Infection following a procedure, initial encounter, plus a code from B95-B97 to identify the organism). -
A procedure code if an intervention is performed, such as Incision and Drainage (Root Operation: Drainage) of the infected site.
-
-
Accidental Dislodgement: If the drain falls out prematurely and needs to be reinserted, the reinsertion is coded as a new Insertion or Drainage procedure.
Chapter 8: The Auditor’s Eye: Common Errors and Best Practices
After reviewing thousands of records, auditors consistently find the same errors with JP drain coding.
Top 5 JP Drain Coding Errors and Their Solutions
| Common Error | Why It’s Wrong | The Correct Approach |
|---|---|---|
| 1. Always using “Insertion” | Fails to capture the intent of the procedure. If the goal was to drain an existing abscess, “Drainage” is the correct root operation. | Analyze the physician’s documentation. Look for keywords: “for post-op drainage” (Insertion) vs. “to drain the abscess” (Drainage). |
| 2. Coding the device for Drainage | The ICD-10-PCS guidelines explicitly state that no device is coded for the root operation Drainage. | For Drainage, always use Device character ‘Z’ (No Device). The device is the method, not the objective. |
| 3. Using an incorrect body part | Coding “Abdominal Wall” when the drain tip is in the “Peritoneal Cavity” lacks specificity and can impact DRG assignment. | Review the operative report and imaging reports. Identify the precise anatomical cavity or tissue space where the drain resides. |
| 4. Coding routine management | Coding nursing actions like emptying the drain bulb is not a billable procedure. | Only code physician-performed procedures that meet the definition of a root operation (Irrigation, Replacement, Removal). |
| 5. Missing the separate procedure | Failing to code an Irrigation or Replacement performed on a different day during the same admission. | Review the entire record. Look for progress notes or procedure notes that indicate a separate, distinct intervention on the drain. |
The Coder’s Checklist:
-
Read the Op Note/Procedure Note: What is the indication for the drain?
-
Determine the Root Operation: Is it Insertion (prophylactic) or Drainage (therapeutic for an existing collection)?
-
Identify the Body Part: Where is the tip of the drain located? Be specific.
-
Identify the Approach: Open, Percutaneous, or Percutaneous Endoscopic?
-
Assign the Device:
Jfor Drainage Device for Insertion and Removal;Zfor Drainage. -
Check for Subsequent Procedures: Was the drain irrigated, replaced, or removed during the stay?
Chapter 9: Real-World Scenarios and Coding Exercises
Let’s apply our knowledge to complex, real-world cases.
Scenario 1: Post-Mastectomy with JP Drain Placement
-
Documentation: “The patient underwent a right simple mastectomy for breast cancer. Hemostasis was achieved. Two JP drains were placed: one in the axillary tail and one in the inferior breast flap. The skin was closed.”
-
Coding Analysis:
-
Indication: Prophylactic, to prevent seroma after tissue removal.
-
Root Operation: Insertion.
-
Body Parts: The axillary tail drain is in the Right Axilla Subcutaneous Tissue and Fascia. The inferior flap drain is in the Right Breast Subcutaneous Tissue and Fascia.
-
Approach: Open (performed as part of the open mastectomy).
-
Codes:
-
0JH8XJZ– Insertion of Drainage Device into Right Axilla Subcutaneous Tissue and Fascia, Open Approach. -
0JH6XJZ– Insertion of Drainage Device into Right Breast Subcutaneous Tissue and Fascia, Open Approach.
-
-
Scenario 2: Percutaneous Drainage of an Abdominal Abscess
-
Documentation: “Under CT-guidance, a trocar was advanced percutaneously into the large, localized fluid collection in the left upper quadrant, adjacent to the spleen. 200cc of purulent material was aspirated. A JP drain was then advanced over a wire into the collection, and secured to the skin.”
-
Coding Analysis:
-
Indication: Therapeutic drainage of an established abscess.
-
Root Operation: Drainage.
-
Body Part: The abscess is in the Peritoneal Cavity (specifically, the left subphrenic space, which rolls up to the Peritoneal Cavity).
-
Approach: Percutaneous.
-
Device:
Z(No Device) for Drainage. -
Code:
0W9G3ZZ– Drainage of Peritoneal Cavity, Percutaneous Approach.
-
Conclusion: Mastering the Minutiae for Macroscopic Accuracy
Accurate JP drain coding hinges on a disciplined, document-driven analysis of procedural intent. By meticulously differentiating between prophylactic Insertion and therapeutic Drainage, selecting the precise anatomical Body Part, and understanding the coding for subsequent management, coders transform a simple clinical tool into a precise data point. This precision ensures compliant billing, supports accurate quality metrics, and ultimately paints a truer picture of the patient’s clinical journey within the inpatient record.
Frequently Asked Questions (FAQs)
Q1: Can I use the Placement section (Section 2) to code a standard JP drain insertion?
A: Generally, no. The Placement section is intended for devices that act on a body region for immobilization, positioning, or moving. A JP drain’s primary function is suction and drainage, which is more accurately captured in the Medical and Surgical section under the root operations of Insertion or Drainage. Only use Placement if the documentation clearly indicates it was placed for a purpose like tamponade that aligns with the official definition.
Q2: If two JP drains are placed in the same body part during the same procedure, do I code both?
A: Yes. ICD-10-PCS coding is specific to the procedure. If the physician places two separate drains in two separate locations (even within the same general body area, like the subcutaneous tissue of the breast), and both are documented, you code both insertions. However, you must ensure the body part values are distinct (e.g., right upper arm vs. right axilla).
Q3: How do I code the removal of a JP drain that is performed during a subsequent, unrelated operating room procedure?
A: If the patient is in the operating room for a different procedure (e.g., a cholecystectomy) and the surgeon simply pulls out an existing JP drain at the beginning or end, this removal is typically not coded separately. It is considered a minor procedure incidental to the main operative session. However, if significant work is required to remove it (e.g., it’s stuck and requires dissection), it may be codeable. Always follow the ICD-10-PCS guideline that procedures that are “included in the operative package” are not coded separately.
Q4: The physician documented ‘JP drain placed to bulb suction.’ What does this mean for my code?
A: The phrase “to bulb suction” simply describes the type of drain and its mechanism of action. It does not change the root operation selection. You must still determine if the placement was prophylactic (Insertion) or to drain an existing collection (Drainage) based on the rest of the documentation.
Q5: What is the ICD-10-PCS code for ‘monitoring’ the JP drain output?
A: There is no code for monitoring drain output. The routine assessment of drain output, character of fluid, and emptying of the bulb are integral parts of nursing care and daily patient assessment. These are not considered reportable procedures in ICD-10-PCS.
Additional Resources
-
The Official ICD-10-PCS Guidelines for Coding and Reporting: The definitive source for rules and conventions. Updated annually by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS).
-
AHA Coding Clinic for ICD-10-CM/PCS: The authoritative publication for official advice and guidance on specific coding scenarios. Search its archives for “drain” or “insertion” for relevant quarterly issues.
-
American Health Information Management Association (AHIMA): Offers a wealth of educational resources, webinars, and practice briefs on procedural coding.
-
Your Facility’s Clinical Documentation Improvement (CDI) Specialist: Collaborate with your CDI team to ensure physician documentation is clear and supports accurate code assignment. They can help educate providers on using precise language like “placed for post-op drainage” vs. “placed to drain the subhepatic abscess.”
Date: November 29, 2025
Author: Surgical Coding Specialist
Disclaimer: This article is intended for educational purposes and to provide a framework for understanding complex medical coding concepts. It is not a substitute for the official ICD-10-PCS Guidelines, Coding Clinician documentation, or professional coding advice. The ultimate responsibility for accurate code assignment lies with the certified coder based on a complete review of the patient’s medical record and adherence to current official coding standards.





