In the intricate ecosystem of modern healthcare, data is the lifeblood that fuels clinical decisions, quality initiatives, epidemiological research, and financial sustainability. At the heart of this data stream lies the often-overlooked yet profoundly critical art and science of medical coding. For inpatient encounters, the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) serves as the definitive language for describing what was done to the patient. While pneumonia itself is a diagnosis (coded in ICD-10-CM), the procedures undertaken to diagnose and treat it—especially when it escalates beyond simple antibiotic therapy—demand precise, granular procedural coding.
A simple code for “thoracentesis” tells only a fraction of the story. Was it a diagnostic aspiration of a small effusion, or a therapeutic drainage of a large, infected empyema? Was it performed blindly or under imaging guidance? Did it require the placement of a temporary catheter or even a surgical window? Each variation carries different clinical resource utilization, risk, and cost. Misapplying a root operation, approach, or device qualifier can distort quality metrics, skew clinical data, and significantly impact a hospital’s reimbursement under Medicare’s Inpatient Prospective Payment System (IPPS) via Medicare Severity Diagnosis-Related Groups (MS-DRGs).
This comprehensive guide is designed to be the ultimate resource for the inpatient coder, auditor, educator, and clinical documentation integrity (CDI) specialist navigating the complex procedural landscape of pneumonia and its complications. We will move beyond the basics, dissecting complex clinical scenarios, unpacking the logic of root operations, and illuminating the direct link between precise documentation and accurate coding. Our journey will equip you not just to assign a code, but to understand its clinical and financial context, ensuring your work upholds the integrity of the patient record and supports the healthcare system’s data-driven mission.
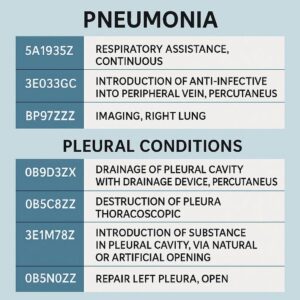
ICD-10-PCS Coding for Pneumonia and Pleural Conditions
2. Understanding the ICD-10-PCS Framework: A Quick Refresher
Before diving into the specifics of respiratory procedures, it is essential to reaffirm the foundational structure of ICD-10-PCS. Unlike its predecessor ICD-9-CM, which was a numeric system with limited space, ICD-10-PCS is an alphanumeric system composed of seven characters, each representing a specific aspect of the procedure.
-
1st Character: Section. Identifies the broad procedural category (e.g., Medical and Surgical, Obstetrics, Imaging). For pneumonia-related procedures, we are almost exclusively in Section 0: Medical and Surgical.
-
2nd Character: Body System. Identifies the general body system. For lungs and pleura, this is B: Respiratory System.
-
3rd Character: Root Operation. The core of the code. This defines the objective of the procedure (e.g., draining, cutting out, examining). This is the most critical decision point for coders.
-
4th Character: Body Part. Specifies the exact anatomical site (e.g., right pleural cavity, lingula of left lung).
-
5th Character: Approach. Describes the technique used to reach the operative site (e.g., open, percutaneous, via natural orifice).
-
6th Character: Device. Used only when a device remains in place after the procedure is concluded (e.g., a drainage catheter). For many procedures, this character is “Z” (No Device).
-
7th Character: Qualifier. Provides additional information, such as a diagnostic or therapeutic intent, or the type of substance involved (e.g., a sclerosant for pleurodesis).
3. The Respiratory System: Section 0, Body System B
Within the Medical and Surgical section (0), the Respiratory System (B) encompasses the lungs, bronchi, trachea, and pleura. For pneumonia complications, our focus will be primarily on the lung parenchyma and, more frequently, the pleural space.
Key Body Parts (4th Character):
-
Pleural Cavity: Right (0), Left (1), Bilateral (2).
-
Lung: Specific lobes (e.g., Upper Lobe, Right (3); Lower Lobe, Left (9)).
-
Bronchus: Main (D), Lobar (F, G, etc.).
4. Root Operations for Pneumonia and Pleural Conditions: A Deep Dive
This is the analytical core of procedural coding. Selecting the correct root operation requires a careful analysis of the physician’s intent and action as documented in the operative report or procedure note.
4.1. Drainage (0): The Primary Weapon Against Infection
Definition: Taking or letting out fluids and/or gases from a body part.
Key Application: This is the most common root operation for parapneumonic effusions and empyemas. The goal is to remove abnormal material (pus, infected fluid) to alleviate symptoms and treat infection.
-
Examples: Thoracentesis (with or without catheter placement), insertion of a chest tube (tube thoracostomy), open surgical drainage of an empyema cavity.
-
Coding Nuance: The approach (5th character) differentiates a percutaneous needle aspiration (3) from a percutaneous endoscopic drainage (4) via thoracoscopy, or an open thoracotomy (0). If a drainage catheter is left in place (like a pigtail catheter), the 6th character (Device) would specify “Drainage Device.”
4.2. Extirpation (C): Removing Matter from Within
Definition: Taking or cutting out solid matter, such as a blood clot, foreign body, or necrotic tissue, from a body part.
Key Application: Crucial for decortication. When an empyema forms a thick, fibrous rind (peel) that entraps the lung, the surgeon must extirpate (peel off) this necrotic tissue from the visceral and parietal pleura to allow the lung to re-expand. The body part is still the Pleural Cavity, but the action is removing solid matter, not just fluid.
-
Why not Drainage? Drainage is for fluid/gas. The empyema peel is solid, organized fibrin and necrotic tissue. The Official Coding Guidelines explicitly state that removal of a fibrin deposit is coded to Extirpation.
-
Why not Resection? Resection involves cutting out/off the entire body part. In decortication, the pleural cavity is not removed; the abnormal material within it is.
4.3. Resection (T): Taking Out All of a Body Part
Definition: Cutting out or off, without replacement, all of a body part.
Key Application: This is used for lung tissue itself. In rare, severe cases of necrotizing pneumonia or a lung abscess that destroys a lobe, a lobectomy or pneumonectomy may be required. Here, the entire anatomical body part (e.g., right lower lobe) is removed.
-
Distinction from Extirpation: Resection removes the organ/structure itself. Extirpation removes abnormal material from within the organ/structure.
4.4. Inspection (J): The Scope Examination
Definition: Visually and/or manually exploring a body part.
Key Application: Diagnostic bronchoscopy or thoracoscopy. When a patient with non-resolving pneumonia undergoes a bronchoscopy to obtain washings or biopsies to identify the causative organism or rule out malignancy, the primary purpose is visual examination and sampling. The sampling (biopsy) is inherent to the Inspection root operation when performed during the same procedure.
4.5. Bypass (1): Re-routing Around a Problem
Definition: Altering the route of passage of the contents of a tubular body part.
Key Application: Rare in infectious contexts, but could be considered if a chronic bronchopleural fistula is surgically managed by redirecting airflow. More common for malignant obstructions.
4.6. Supplement (U): Putting in a Pleural Sclerosant
Definition: Putting in or on a biological or synthetic material that physically reinforces and/or augments the function of a body part.
Key Application: Chemical Pleurodesis. For recurrent malignant effusions (which can complicate pneumonia in immunocompromised patients) or persistent benign effusions, a sclerosing agent (like talc or doxycycline) is instilled into the pleural space. The intent is not to drain but to cause inflammation and adhesion between the visceral and parietal pleura (supplementing the space), thereby preventing fluid re-accumulation. This is often performed during a thoracoscopy.
5. The Crucial Nuance of the 7th Character: Qualifiers for Devices and Substances
The 7th character is where specific substances are identified. For Supplement (pleurodesis), this character specifies the agent used (e.g., Talc (0), Other Agent (7)). For Drainage procedures, a common qualifier is “Diagnostic” (X) versus “Therapeutic” (default, Z). A diagnostic thoracentesis, where the sole goal is to obtain a fluid sample for lab analysis, would use qualifier X.
6. Approach: From Percutaneous to Open Thoracotomy
The approach (5th character) is vital for resource stratification. It follows a hierarchy of invasiveness:
-
0 Open: Large incision (e.g., thoracotomy for decortication).
-
3 Percutaneous: Puncture through the skin (e.g., needle thoracentesis, CT-guided drainage catheter).
-
4 Percutaneous Endoscopic: Using a scope inserted through a small percutaneous incision (e.g., video-assisted thoracoscopic surgery – VATS).
-
7 Via Natural or Artificial Opening: e.g., bronchoscopy through the mouth.
-
8 Via Natural/Artificial Opening Endoscopic: Standard.
7. Clinical Scenarios and Code Building: From Simple to Complex
Let’s apply this knowledge to real-world documentation.
Scenario 1: Simple Parapneumonic Effusion
-
Documentation: “Under ultrasound guidance, a 22-gauge needle was inserted into the right posterior pleural space. 150mL of straw-colored fluid was aspirated and sent for cell count, culture, and chemistries. The procedure was well-tolerated.”
-
Analysis: The goal is to take out fluid for diagnostic purposes. Root Operation: Drainage (0). Body Part: Right Pleural Cavity (0). Approach: Percutaneous (3). No device left. Qualifier: Diagnostic (X).
-
ICD-10-PCS Code: 0B9B3ZX (Drainage of Right Pleural Cavity, Percutaneous Approach, Diagnostic).
Scenario 2: Complex Empyema with Decortication
-
Documentation: “Patient taken for VATS for complex loculated empyema. Three port incisions made. Approximately 800mL of purulent fluid evacuated. A thick, fibrous peel was encountered, completely encasing the lower lobe. Careful and complete decortication was performed, stripping the peel from both the visceral and parietal pleura. The lung fully re-expanded. A 28Fr chest tube was placed through one of the port sites.”
-
Analysis: Two distinct procedures were performed.
-
Drainage of Empyema Fluid: Drainage (0) of Left Pleural Cavity (1), via Percutaneous Endoscopic (4) approach, with a Drainage Device (chest tube) left in place (6th char: Drainage Device). Therapeutic qualifier. Code: 0B9L4CZ.
-
Decortication: Removal of solid matter (the peel). Root Operation: Extirpation (C). Body Part: Left Pleural Cavity (1). Approach: Percutaneous Endoscopic (4). No device for this part. Code: 0B9L4CZ. (Note: This would be a second, separate PCS code).
-
-
Coding: Both codes are assigned.
Scenario 3: Non-Resolving Pneumonia with Bronchoscopy
-
Documentation: “Flexible bronchoscopy advanced to the left lower lobe bronchus. Thick purulent secretions were suctioned. Bronchoalveolar lavage (BAL) was performed in the lingula with 60mL saline. Biopsies were taken from an area of inflamed mucosa.”
-
Analysis: Primary goal is visual inspection and diagnostic sampling. Root Operation: Inspection (J). Body Part: Lung, Lingula (8). Approach: Via Natural/Artificial Opening Endoscopic (8). No device. Code: 0BJ98ZZ.
8. DRG Implications: How Your Code Choice Drives Reimbursement
Procedural coding directly determines the surgical hierarchy for DRG assignment. For respiratory conditions, the DRG grouper looks for Major Chest Procedures (DRGs 163-168) versus Other Respiratory System O.R. Procedures (DRGs 175-179). A VATS decortication (Extirpation) is weighted much more heavily than a simple chest tube (Drainage). Miscoding a decortication as a simple drainage could downcode the case from a higher-paying DRG (e.g., DRG 166 – Other Respiratory System O.R. Procedures with CC/MCC) to a lower-paying one (DRG 178 – Respiratory Infections & Inflammations with MCC), resulting in a significant financial loss for the hospital.
Common ICD-10-PCS Codes for Pneumonia Procedures and DRG Impact
| Clinical Procedure | Root Operation | Example PCS Code | Typical DRG Family | Relative Weight/Complexity |
|---|---|---|---|---|
| Diagnostic Thoracentesis | Drainage (0) | 0B9B3ZX | 178, 179 (Medical) | Low |
| Chest Tube for Empyema | Drainage (0) | 0B9L3CZ | 166, 167 (Surgical) | Medium |
| VATS Decortication | Extirpation (C) | 0B9L4CZ | 163, 164 (Major Chest) | High |
| Open Lobectomy | Resection (T) | 0BTG0ZZ | 163, 164 (Major Chest) | Very High |
| Diagnostic Bronchoscopy | Inspection (J) | 0BJ98ZZ | 175, 176 (Surgical) | Low-Medium |
| VATS with Talc Pleurodesis | Supplement (U) | 0B9L4U0 | 166, 167 (Surgical) | Medium-High |
9. Common Pitfalls and Auditing Challenges
-
Confusing Drainage and Extirpation: This is the #1 audit finding. Coders must look for key terms: “fibrinous peel,” “rind,” “cortex,” “decortication.” These all point to Extirpation, not Drainage.
-
Missing the Second Procedure: In a combined VATS procedure (drainage + decortication + pleurodesis), failing to code all distinct root operations.
-
Incorrect Approach: Coding a VATS procedure as “Percutaneous” (3) instead of the more specific “Percutaneous Endoscopic” (4).
-
Overlooking the Qualifier: Not specifying a diagnostic intent (X) or the specific sclerosant (e.g., Talc (0)) for pleurodesis.
-
Body Part Laterality Errors: Confusing right (0) and left (1) pleural cavity.
10. The Future of Coding: AI, Automation, and Continued Education
The future of ICD-10-PCS coding lies in a synergy between human expertise and technology. Computer-assisted coding (CAC) and natural language processing (NLP) can flag key terms in operative reports, but the final clinical judgment—distinguishing between “drainage of pus” and “extirpation of fibrinous peel”—will remain the domain of the skilled coder. Continuous education, engagement with CDI specialists, and diligent review of AHA Coding Clinic advice are non-negotiable for maintaining accuracy in this evolving field.
11. Conclusion
Accurate ICD-10-PCS coding for pneumonia complications is a meticulous process that demands a deep understanding of surgical intent, anatomical nuance, and the PCS framework’s logic. By mastering root operations like Drainage, Extirpation, and Supplement, and carefully analyzing clinical documentation, coders ensure data integrity, support quality patient care metrics, and secure appropriate reimbursement for the complex resources used in treating these serious conditions.
12. Frequently Asked Questions (FAQs)
Q1: How do I code a “window thoracostomy” or “Eloesser flap” for chronic empyema?
A: This is an open surgical creation of a permanent opening in the chest wall to drain a chronic empyema cavity. It is coded to the root operation Drainage (0) of the Pleural Cavity, with an Open (0) approach. The creation of the skin flap is considered an integral part of the drainage procedure.
Q2: The surgeon documents “VATS with lysis of adhesions.” Is this coded separately?
A: Lysis of adhesions performed to access the pleural cavity or lung is not coded separately. It is considered a necessary integral part of the main procedure (e.g., the decortication or drainage).
Q3: What is the difference between a “drainage device” (6th character) and a “qualifier” for diagnostic aspiration?
A: The Device character (6th) is used only when a device (like a catheter) remains in the body after the procedure ends. The Qualifier (7th) for “Diagnostic” (X) describes the purpose of the procedure. You can have a diagnostic procedure where a temporary needle is used (no device) or a therapeutic drainage where a catheter is left (device).
Q4: How do I code a bedside “pigtail catheter” placement for an empyema?
A: This is Drainage (0) of the Pleural Cavity, via Percutaneous (3) approach, with a Drainage Device (6th char) left in place. The code is 0B9L3CZ.
Q5: Where can I find official guidance on ambiguous scenarios?
A: The AHA Coding Clinic for ICD-10-CM/PCS is the authoritative source. Always reference its quarterly advice for official interpretations.
Author: The Coding Integrity Team
Date: December 07, 2025
Disclaimer: This article is intended for educational and informational purposes for healthcare coding professionals. It is not a substitute for official coding guidelines, payer-specific policies, or clinical advice. Always consult the most current ICD-10-PCS code books, CMS guidelines, and AHA Coding Clinic for definitive coding direction.





