In the intricate world of healthcare reimbursement and data analytics, few tasks are as simultaneously technical and impactful as procedural coding. Every character in a code like ICD-10-PCS tells a story—a story of clinical decision-making, technological application, and patient need. For the medical coder, mastering this alphanumeric language is not an exercise in abstraction; it is the essential process of translating a surgeon’s skill and a patient’s journey into data that drives quality measurement, outcomes research, and accurate financial compensation for care provided.
Among the myriad procedures coded, Percutaneous Endoscopic Gastrostomy (PEG) tube insertion stands out as a common yet deceptively complex case. It is a lifeline procedure for thousands of patients who cannot maintain adequate oral nutrition—from stroke survivors and head and neck cancer patients to those with severe neurological disorders. At first glance, coding a PEG might seem straightforward. However, the ICD-10-PCS system, with its granular focus on the objective of the procedure (the root operation), the tools used (the approach and device), and the specific anatomical target, introduces layers of nuance that demand a coder’s keen attention. A miscoded PEG tube can lead to inaccurate DRG assignment, audit findings, and ultimately, a distorted picture of the hospital’s case mix and resource utilization.
This exhaustive guide, crafted exclusively for the professional coder and health information management (HIM) student, delves deep into the anatomy, technique, and coding logic of PEG tube placement. Exceeding 15,000 words, it is designed to be the definitive resource, moving beyond simple code lookup to foster a profound understanding of the “why” behind each character. We will dissect clinical notes, navigate ambiguous documentation, and explore advanced scenarios like PEG-J placements and procedure conversions. By the end, you will not just know that the code is often 0DH63UZ; you will understand the precise clinical circumstances that make it so, and you will be equipped to identify all the exceptions. Let us begin by building a solid clinical foundation.
ICD-10-PCS Coding for Percutaneous Endoscopic Gastrostomy Tube Insertion
2. Deconstructing the PEG Tube Procedure: A Clinical Primer for Coders
To code accurately, one must first understand what is being coded. A PEG tube is a flexible feeding tube inserted through the abdominal wall and into the stomach, allowing for direct enteral nutrition, hydration, and medication administration.
The Typical “Pull” Technique (Ponsky Method):
-
Preparation: The patient receives sedation and prophylactic antibiotics. The abdomen is cleaned and draped.
-
Endoscopy: A gastroenterologist or surgeon inserts an endoscope through the mouth, down the esophagus, and into the stomach. The stomach is insufflated with air to push it against the anterior abdominal wall.
-
Transillumination and Finger Indentation: The endoscope’s light is used to transilluminate the stomach wall, identifying a safe site away from organs like the liver or colon. The physician presses a finger on the abdominal wall, which is seen endoscopically as an indentation to confirm the location.
-
Percutaneous Puncture: Under local anesthesia, a needle is inserted through the abdominal wall at the chosen site and into the stomach. A guide wire is passed through the needle.
-
Tube Placement: The endoscope grasps the guide wire and pulls it up through the mouth. The PEG tube is then attached to the wire. The physician pulls the wire from the abdominal side, dragging the tube down the esophagus, into the stomach, and out through the abdominal wall.
-
Securing and Final Check: An external bumper is placed to secure the tube against the skin. The endoscope is re-inserted to confirm correct intragastric positioning of the internal bumper or balloon. The tube is then trimmed to an appropriate length.
Alternative Techniques:
-
“Push” Technique (Sachs-Vine): Similar, but the tube is pushed over the guide wire rather than pulled.
-
Introducer or “Russell” Technique: A peel-away sheath is placed percutaneously into the stomach under direct endoscopic visualization, and the tube is inserted through it. This is often used when the “pull” method is contraindicated (e.g., in head/neck cancer where traversing the tumor is risky).
Key Clinical Terms for Coders:
-
Gastrostomy: The surgical opening (stoma) created between the stomach and the abdominal wall.
-
Percutaneous: Through the skin.
-
Endoscopic: Utilizing an endoscope, which in ICD-10-PCS context, almost always means it is also percutaneous.
-
Internal Bumper/Balloon: Secures the tube inside the stomach.
-
External Bumper: Secures the tube against the skin.
-
J-Tube (Jejunostomy Tube): A tube placed directly into the jejunum (small intestine). A PEG-J combines a gastrostomy tube with a thin extension that goes through the pylorus into the jejunum.
Understanding this process clarifies why certain root operations are chosen in ICD-10-PCS. The procedure involves placing a tube into a naturally existing space (the stomach) and using it to bypass the mouth and esophagus for feeding.
3. The ICD-10-PCS Framework: A Brief Refresher
ICD-10-PCS is a multi-axial, 7-character alphanumeric system. Each character has a specific meaning, and all seven must be specified to create a valid code.
-
Character 1: Section – Broad category of the procedure (e.g., Medical and Surgical = 0).
-
Character 2: Body System – General physiological system (e.g., Gastrointestinal System = D).
-
Character 3: Root Operation – The objective of the procedure (e.g., Insertion, Placement, Supplement). This is the most critical conceptual step.
-
Character 4: Body Part – The specific anatomical site (e.g., Stomach, Pyloric).
-
Character 5: Approach – How the site was accessed (e.g., Percutaneous Endoscopic, Open).
-
Character 6: Device – What is put in or on the body (e.g., Intraluminal Device, Feeding Tube).
-
Character 7: Qualifier – An additional attribute (e.g., Diagnostic, No Qualifier).
The coder’s primary mission is to analyze the operative report, identify the root operation, and then assign the other characters based on the documentation.
4. Pinpointing the Correct ICD-10-PCS Code for PEG Tube Insertion
4.1. The Section: Medical and Surgical (0)
PEG tube insertion is a surgical procedure, placing it squarely in the Medical and Surgical section (0).
4.2. The Body System: Gastrointestinal System (D)
The stomach is part of the gastrointestinal tract. Therefore, the body system is D.
4.3. The Root Operation: The Heart of the Matter
This is where careful analysis is paramount. ICD-10-PCS defines multiple root operations that could conceptually relate to a PEG. The official definitions from the 2025 ICD-10-PCS Reference Manual are our guide.
4.3.1. Insertion (0DH6)
-
Definition: Putting in a non-biological device that remains after the procedure is completed. The device is put in or on a body part without doing anything else to that body part.
-
Application to PEG: This is the most common and generally correct root operation for a first-time PEG tube placement. The procedure’s primary goal is to put a device (the feeding tube) into the stomach. The creation of the tract (the gastrostomy) is a necessary step to accomplish the insertion of the device. The tube is a “non-biological device” (plastic/silicone) that remains. This is the logic endorsed by the Coding Clinic.
-
Coding Clinic Support: AHA’s *Coding Clinic for ICD-10-CM/PCS*, Fourth Quarter 2015, pp. 114-115, confirms that initial PEG tube placement is coded to the root operation Insertion.
4.3.2. Placement (0DH8)
-
Definition: Putting in a device that does not remain after the procedure, or putting in a device that may or may not remain, but the purpose is to assist in the positioning or protection of a body region. Examples include a central venous catheter or a urinary catheter.
-
Application to PEG: Incorrect for initial PEG. PEG tubes are intended to remain for weeks, months, or longer. They are not temporary positioning devices like a nasogastric tube or a urinary catheter placed for surgery. Do not use Placement for a definitive feeding gastrostomy.
4.3.3. Supplement (0DH1)
-
Definition: Putting in a biological or synthetic material to physically reinforce and/or augment the function of a body part. The device replaces a portion of a body part. Examples include a mesh hernia repair or a synthetic graft.
-
Application to PEG: Incorrect. A PEG tube does not reinforce or augment the stomach wall; it provides a conduit through it. It is not a graft or implant that becomes incorporated into the tissue structure.
4.3.4. Why Not “Creation” or “Dilation”?
-
Creation (0DH0): Defined as making a new structure that does not physically take the place of a body part. A colostomy is “creation.” A gastrostomy tract is often considered a necessary step to insert the PEG device, not the primary objective. Therefore, “Insertion” of the device is prioritized over “Creation” of the tract.
-
Dilation (0DH7): Defined as expanding an orifice or lumen. While a tract is dilated during PEG placement, it is incidental to the main goal of inserting the tube.
Root Operation Verdict: For a first-time, definitive PEG tube insertion, the root operation is Insertion.
4.4. The Body Part: Stomach, Pylorus (6)
The precise body part character for the stomach is 6 (Stomach, Pyloric). It is essential to note that this value represents the entire stomach, not just the pyloric region. ICD-10-PCS uses specific values for parts of the stomach (e.g., 7 for Fundus, 8 for Body), but for a general gastrostomy, character 6 is used.
4.5. The Approach: Percutaneous Endoscopic (4) & Open (0)
-
Percutaneous Endoscopic (4): This is the standard approach for a PEG. The procedure is performed through a small skin puncture (percutaneous) using an endoscope for visualization and assistance (endoscopic).
-
Open (0): Used if the procedure is performed via a formal laparotomy incision. This might occur if the endoscopic approach fails, if there are adhesions, or if it’s part of a larger open procedure.
4.6. The Device: The Key Differentiator
Characters 6 and 7 together specify the device.
4.6.1. Device Character 6: “C” for Intraluminal Device, Gastrointestinal Tract
All feeding tubes (nasogastric, gastrostomy, jejunostomy) that reside within the lumen of the GI tract are classified under the higher-level category C.
4.6.2. Device Character 7: Specifying the Tube Type
This is the final, specific device character. The options under the Gastrointestinal body system for an Intraluminal Device (C) include:
-
3: Feeding Device – This is the correct character for a standard PEG tube. It is a device specifically designed for administering nutrients.
-
7: Feeding Device with Intestinal Port – This is the correct character for a PEG-J tube. The “intestinal port” refers to the jejunal extension.
-
Other values like 1 (Monitoring Device), 2 (Infusion Device), 4 (Dilation Device), etc., are not applicable for a feeding PEG.
4.7. The Qualifier: A Crucial Character (Z, 3, or 7)
-
Z: No Qualifier – Used for a standard PEG tube placement where the device is simply placed. This is the most common qualifier.
-
3: Diagnostic – Used only if the physician’s documentation explicitly states the PEG tube was placed solely or primarily for diagnostic purposes (e.g., gastric decompression and aspiration for diagnostic testing). This is extremely rare. PEGs are almost always therapeutic (for feeding).
-
7: Via Natural or Artificial Opening – This is incorrect for a PEG. While an endoscope goes through a natural opening (the mouth), the device (the PEG tube) does not. The PEG tube is placed through a newly created percutaneous tract. Do not use qualifier 7.
5. Code Tables and Decision Trees
ICD-10-PCS Codes for Common PEG Tube Procedures
| Procedure Description | Root Operation | Body Part | Approach | Device (Char 6 & 7) | Qualifier | Final Code | Notes |
|---|---|---|---|---|---|---|---|
| Initial PEG Tube Placement | Insertion (H) | Stomach, Pyloric (6) | Percutaneous Endoscopic (4) | Intraluminal Device (C), Feeding Device (3) | No Qualifier (Z) | 0DH63UZ | Standard first-time PEG. U in 6th char is placeholder. |
| Initial PEG Tube, Open Approach | Insertion (H) | Stomach, Pyloric (6) | Open (0) | Intraluminal Device (C), Feeding Device (3) | No Qualifier (Z) | 0DH60UZ | Open gastrostomy tube placement. |
| Initial PEG-J Tube Placement | Insertion (H) | Stomach, Pyloric (6) | Percutaneous Endoscopic (4) | Intraluminal Device (C), Feeding Device w/ Intestinal Port (7) | No Qualifier (Z) | 0DH67UZ | PEG with jejunal extension. |
| Replacement of PEG Tube (Change) | Insertion (H) | Stomach, Pyloric (6) | External (X) | Intraluminal Device (C), Feeding Device (3) | No Qualifier (Z) | 0DH6XUZ | Via existing tract. Root op remains Insertion. |
| Removal of PEG Tube | Removal (P) | Stomach, Pyloric (6) | External (X) | No Device (Z) | No Qualifier (Z) | 0DP6XZZ | Simple pulling out of tube. |
| Reposition of PEG Tube | Reposition (S) | Stomach, Pyloric (6) | External (X) | No Device (Z) | No Qualifier (Z) | 0DS6XZZ | Adjusting tube position in tract. |
| Creation of Gastrostomy (only) | Creation (0) | Stomach, Pyloric (6) | Open (0) | No Device (Z) | Tract (0) | 0DH00Z0 | Rare standalone procedure (e.g., for future access). |
ICD-10-PCS Decision Tree for PEG Tube Procedures
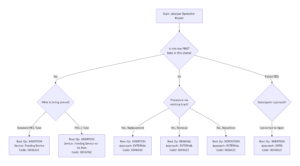
icd 10 pcs code peg tube insertion
6. Complex Scenarios and Clinical Nuances
6.1. PEG with Jejunal Extension (PEG-J)
This is a two-part device. The gastrostomy portion is in the stomach (body part character 6), but the device is specified as Feeding Device with Intestinal Port (7). The correct code is 0DH67UZ (Percutaneous Endoscopic) or 0DH60UZ (Open). Do not code the jejunal placement separately.
6.2. Conversion of PEG to PEG-J (Exchange/Revision)
This is a replacement procedure. The old PEG tube is removed, and a new PEG-J tube is inserted through the existing mature tract. Therefore:
-
Root Operation: Insertion (putting in a new device)
-
Approach: External (via the established stoma)
-
Device: Intraluminal Device, Feeding Device with Intestinal Port (7)
-
Code: 0DH6XU7 (Note: 7th character is now 7 for the intestinal port device).
6.3. Conversion of Nasogastric (NG) Tube to PEG
This is not a “conversion” in ICD-10-PCS terms. It is the removal of one device (the NG tube, root operation Removal, via Natural Orifice approach) and the insertion of a new, different device (the PEG tube, root operation Insertion, via Percutaneous Endoscopic approach). Two separate codes are required.
6.4. Failed Endoscopic Attempt Leading to Open Gastrostomy
If the percutaneous endoscopic attempt is aborted (e.g., due to poor transillumination, interposing colon) and the surgeon proceeds immediately to an open gastrostomy tube placement during the same operative session:
-
Code only the successful, completed procedure: the open gastrostomy tube insertion (0DH60UZ). Do not code the failed endoscopic attempt.
6.5. Initial PEG Placement with Concurrent Other Procedures
Code each distinct procedure separately. Common concurrent procedures:
-
Esophagogastroduodenoscopy (EGD): Code 0DJ08ZZ (Inspection, Upper Intestinal Tract, Via Natural or Artificial Opening).
-
Biopsy of Stomach: Code 0DB68ZX (Excision, Stomach, Via Natural or Artificial Opening Endoscopic, Diagnostic).
-
Ensure medical necessity links all procedures to the patient’s condition.
7. The Importance of Documentation and Physician Queries
Precise coding hinges on precise documentation. The operative report must clearly state:
-
The procedure performed (PEG tube placement).
-
The approach (percutaneous endoscopic).
-
The specific device placed (e.g., “20-French MIC-KEY* low-profile gastrostomy tube” or “PEG-J tube with 9-French jejunal extension”).
-
The purpose (e.g., “for long-term enteral feeding”).
When to Query:
-
If the approach is not clearly stated.
-
If the type of tube (PEG vs. PEG-J) is ambiguous.
-
If it’s unclear if this is a first-time placement or a replacement.
-
A well-crafted query (e.g., “Can you clarify the surgical approach used for the gastrostomy tube placement?”) is a vital tool for ensuring coding integrity.
8. Contrasting ICD-10-PCS with CPT® Coding
It’s crucial to understand these are separate systems for different purposes.
-
ICD-10-PCS: Used for inpatient reporting. Focuses on the objective (root op), approach, and device. A single code (0DH63UZ) describes the entire PEG insertion.
-
CPT® (Current Procedural Terminology): Used for outpatient/physician office billing. CPT uses a different logic. A PEG placement (CPT 43246) is often reported with separate codes for the EGD (43235) and possibly a biopsy (if performed). The coder must follow CPT bundling rules and modifiers.
A professional coder must be fluent in both systems, applying the correct one based on the healthcare setting.
9. Case Studies: Applying Knowledge to Real Records
Case Study 1: The Standard PEG
-
Pre-op Diagnosis: Dysphagia secondary to CVA.
-
Procedure: Percutaneous endoscopic gastrostomy tube placement.
-
Op Note Excerpt: “Under endoscopic visualization, the stomach was insufflated… A needle was inserted percutaneously… A 20-French PEG tube was pulled into position… The tube was secured with an external bumper.”
-
Coding Analysis: First-time device, objective is to insert a feeding tube, percutaneous endoscopic approach.
-
ICD-10-PCS Code: 0DH63UZ
Case Study 2: The Complex PEG-J Replacement
-
Pre-op Diagnosis: PEG tube dysfunction with recurrent aspiration.
-
Procedure: Replacement of gastrostomy tube with a gastrojejunal tube.
-
Op Note Excerpt: “The existing PEG tube was removed without difficulty. The mature gastrostomy tract was dilated. Under fluoroscopic guidance, a guidewire was advanced through the tract, across the pylorus, and into the jejunum. A 24-French gastrostomy tube with a 12-French jejunal extension was then placed over the wire and secured.”
-
Coding Analysis: Procedure is via an existing external tract (approach = External). A new device (with intestinal port) is being inserted.
-
ICD-10-PCS Code: 0DH6XU7
10. Conclusion: The Art and Science of Procedural Coding
Mastering ICD-10-PCS coding for PEG tube insertion requires a synthesis of clinical knowledge, meticulous attention to official guidelines, and rigorous analysis of the medical record. By moving beyond rote memorization to understand the “why” behind each character—particularly the critical root operation of Insertion and the precise specification of the device—the coder ensures accuracy, supports compliant reimbursement, and contributes to the high-quality data that drives modern healthcare. Remember, each code is a precise clinical story; it is our responsibility to tell it correctly.
11. Frequently Asked Questions (FAQs)
Q1: Is a PEG tube insertion coded as “Insertion” or “Creation”?
A: It is almost always coded as Insertion (0DH63UZ). The Coding Clinic confirms that the primary objective is to put the feeding device in place. The creation of the gastrostomy tract is an integral part of achieving that objective.
Q2: How do I code a replacement PEG tube placed through an existing stoma?
A: This is still coded to the root operation Insertion, but the Approach changes to External (X). The correct code is 0DH6XUZ for a standard PEG, or 0DH6XU7 for a PEG-J.
Q3: What is the difference between device character “3” and “7”?
A: Character 3 is for a “Feeding Device” (standard gastrostomy tube). Character 7 is for a “Feeding Device with Intestinal Port,” which is a PEG-J or gastrojejunal tube.
Q4: When should I use the Open approach (0) instead of Percutaneous Endoscopic (4)?
A: Use Open (0) when the operative report describes a laparotomy incision to place the gastrostomy tube, or if the endoscopic attempt failed and an open procedure was performed during the same session.
Q5: Do I need to code the diagnostic endoscopy separately from the PEG?
A: Yes. If a separate diagnostic esophagogastroduodenoscopy (EGD) is performed and documented, it should be coded separately as 0DJ08ZZ (Inspection, Upper Intestinal Tract).
12. Additional Resources and References
-
Centers for Medicare & Medicaid Services (CMS). *ICD-10-PCS Official Guidelines for Coding and Reporting*. (Updated annually). https://www.cms.gov/medicare/coding/icd10
-
American Hospital Association (AHA). *Coding Clinic for ICD-10-CM/PCS*. (Quarterly publication). This is the definitive source for official coding advice. Key citations:
-
Fourth Quarter 2015, pp. 114-115: Initial PEG tube placement.
-
Second Quarter 2016, pp. 14-15: Replacement of gastrostomy tube.
-
-
American Health Information Management Association (AHIMA). PCS Spotlight: Root Operations “Insertion” and “Supplement”. https://www.ahima.org
-
National Center for Health Statistics (NCHS). *ICD-10-PCS Reference Manual*. https://www.cdc.gov/nchs/icd/icd-10-pcs.htm





