If you are managing patients on blood thinners like warfarin (Coumadin), you know how vital regular PT/INR testing is. It’s the cornerstone of patient safety, ensuring the medication is working effectively without causing dangerous bleeding. But for those of us in the medical field, the clinical side is only half the story. The other half is making sure the crucial work we do is properly documented and reimbursed, especially by Medicare.
Navigating the world of medical coding can sometimes feel like learning a foreign language. You know what needs to be done for the patient, but translating that into the correct codes for a claim form can be a hurdle. One of the most common points of confusion revolves around a simple question: What is the correct PT/INR ICD-10 code for Medicare?
This guide is here to clear up that confusion. We’ll walk through everything you need to know, from the fundamental “why” behind the codes to the specific numbers you need to use. Whether you’re a seasoned billing specialist, a nurse managing a Coumadin clinic, or a physician trying to streamline your workflow, this article will provide a realistic, practical, and reliable roadmap.
We’ll keep things simple, friendly, and focused on what matters: getting your claims right so you can get back to focusing on your patients.
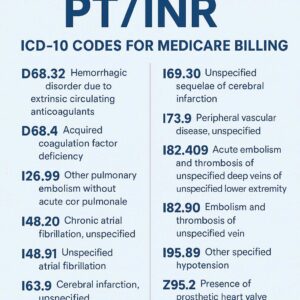
PT INR ICD-10 Codes for Medicare Billing
Understanding the Basics: What is PT/INR and Why Does Medicare Care?
Before we dive into the codes, let’s make sure we are all on the same page about what we are measuring and why Medicare has such specific rules about it.
The “Why” Behind the Test
PT stands for Prothrombin Time, and INR stands for International Normalized Ratio. In simple terms, this blood test measures how long it takes for your patient’s blood to clot. For patients taking warfarin, the goal is to slow down the clotting process just enough to prevent harmful clots (like those that cause strokes or pulmonary embolisms) but not so much that it causes spontaneous bleeding.
Think of it like driving a car. Warfarin is the brake pedal. The PT/INR test is your speedometer. You need to check the speedometer regularly to make sure the car isn’t going too fast (risking a clot) or too slow (risking a bleed). The “therapeutic range” is the ideal speed limit, and it varies depending on why the patient is on the medication in the first place.
Medicare’s Focus: Medical Necessity
Medicare is a federally funded program, and like any good insurance, it only wants to pay for services that are medically necessary. This is the single most important concept to understand for billing.
You cannot simply bill Medicare for a PT/INR test “because the patient is on warfarin.” You must prove, through your coding, that the test was necessary at that specific point in time. The ICD-10 code is the primary tool you use to tell that story. It answers Medicare’s questions:
-
Why is this patient on warfarin?
-
Why do they need their blood tested today?
If the story your codes tell is incomplete or confusing, Medicare will deny the claim. It’s not about being difficult; it’s about ensuring the appropriate use of taxpayer funds. Understanding this principle makes the specific code choices much more logical.
The Core of the Matter: The Primary ICD-10 Code for Long-Term Warfarin Use
For the vast majority of patients on long-term warfarin therapy, the “why” behind their need for monitoring is consistent. They have a chronic condition that requires anticoagulation. The code that captures this ongoing need is your go-to code for most follow-up PT/INR visits.
Z79.01: The Workhorse Code
The code you will use most frequently is Z79.01. Its full descriptor is: Long-term (current) use of anticoagulants.
This code is found in the ICD-10-CM chapter for “Factors influencing health status and contact with health services” (the Z codes). It is not a diagnosis of a disease itself, but rather a factor that impacts the patient’s health and necessitates medical care.
When to use Z79.01:
-
For a patient who is stable on warfarin and presents for a routine, scheduled PT/INR check.
-
The purpose of the visit is specifically to monitor the effects of the anticoagulant medication.
-
The patient has an underlying condition (like atrial fibrillation) that requires the warfarin, but the reason for today’s encounter is the medication management.
Think of it as the “chronic management” code. It tells Medicare, “This patient is on this medication, and we are routinely checking to ensure the dose is correct.” It implies stability and routine monitoring.
| Code | Description | Typical Use Case |
|---|---|---|
| Z79.01 | Long-term (current) use of anticoagulants | Routine, scheduled PT/INR monitoring for a stable patient. |
| Z79.02 | Long-term (current) use of antithrombotics/antiplatelets | Use for patients on drugs like clopidogrel (Plavix), not warfarin. |
| Z79.1 | Long-term (current) use of non-steroidal anti-inflammatories (NSAIDs) | Use for patients on long-term NSAID therapy (e.g., for arthritis). |
Important Note: While Z79.01 is the primary code for the encounter, it is almost always used in conjunction with a code that describes the underlying condition that necessitates the anticoagulation. We’ll cover that in detail in the “Sequencing” section below.
When Routine Becomes Acute: Coding for Unstable Patients
What happens when a patient comes in for a check and their INR is sky-high or dangerously low? The purpose of the visit shifts from “routine monitoring” to “managing a problem.” This is a critical distinction, and your coding must reflect it.
In these cases, you move away from the Z79.01 code as the primary reason for the visit and instead use a code that describes the condition related to the abnormal finding.
T45.515A: The Code for Adverse Effects
One of the most critical codes to understand for unstable patients is T45.515A. This code stands for: Adverse effect of anticoagulants, initial encounter.
This is a heavy-hitter code, and it must be used correctly.
What it means:
“Adverse effect” in coding language doesn’t necessarily mean the patient is having a severe allergic reaction. In the context of anticoagulants, it refers to the expected pharmacological effects of the drug going awry. The medication is doing exactly what it’s supposed to do (thin the blood), but it’s doing it too much (high INR) or perhaps not enough (low INR leading to a clot). The effect has become “adverse” to the patient’s current state of health.
When to use T45.515A:
-
A patient on warfarin presents with a significantly elevated INR (e.g., above 4.0 or 5.0), putting them at risk of bleeding.
-
A patient on warfarin presents with a new, active bleed (like nosebleeds, gum bleeding, or blood in the urine) related to their therapy.
-
A patient on warfarin presents with a new thrombotic event (like a DVT or PE) because their INR was sub-therapeutic.
The “A” at the end of the code stands for “initial encounter.” This is used for the first time you are actively treating the adverse effect. For subsequent visits related to managing the fallout of that adverse effect (e.g., follow-up after a bleed), you would use T45.515D (subsequent encounter).
R79.1: The Code for Abnormal Coagulation Profile
Sometimes, the INR is out of range, but the patient isn’t actively bleeding or clotting. The finding is simply a lab abnormality that needs to be addressed. In this case, you might use R79.1, which stands for: Abnormal coagulation profile.
This is a “symptom” code. It tells the story that the lab result itself is abnormal, and that is the reason for this particular encounter or the need for a dosage adjustment.
When to use R79.1:
-
A patient comes in for a routine check (you would still use Z79.01 as the primary reason for the visit), and you discover their INR is slightly out of range (e.g., 1.8 or 3.8). You will adjust their dose.
-
While R79.1 can be used as an additional code to specify the abnormal finding, it’s often more appropriate to pair Z79.01 with the underlying condition code. Using R79.1 is most relevant when the abnormal result is the central focus.
A Simple Comparison:
| Patient Scenario | Primary ICD-10 Code (Reason for Encounter) | Secondary ICD-10 Code |
|---|---|---|
| Stable patient with atrial fibrillation here for monthly INR check. INR is 2.5. | Z79.01 (Anticoagulant use) | I48.91 (Atrial fibrillation) |
| Patient with mechanical heart valve here for check. INR is 5.5, no bleeding. | T45.515A (Adverse effect) | Z95.2 (Heart valve replacement) |
| Patient with history of PE here for check. INR is 1.2, and they have new chest pain. | T45.515A (Adverse effect – as it led to the PE) | Z86.71 (Personal history of PE) + I26.99 (PE – if confirmed) |
| Patient on warfarin for DVT. INR is 3.8, no bleeding. | Z79.01 (Monitoring) | Z86.71 (Personal history of DVT) |
Don’t Forget the “Why”: Coding the Underlying Condition
As hinted at above, your claim should almost never consist of just Z79.01. To build a complete and defensible story for Medicare, you need to connect the medication to the reason the patient is taking it. This is done by adding a diagnosis code for the underlying condition.
This is not just good practice; it’s often essential for proving medical necessity. Medicare wants to know that the warfarin use is justified.
Here are the most common underlying conditions that require anticoagulation and their corresponding ICD-10 codes:
Common Associated Diagnoses
-
Atrial Fibrillation and Flutter: This is perhaps the most common reason for long-term anticoagulation in the elderly.
-
I48.91: Unspecified atrial fibrillation
-
I48.21: Chronic persistent atrial fibrillation
-
I48.3: Typical atrial flutter
-
I48.4: Atypical atrial flutter
-
-
Venous Thromboembolism (VTE): This category covers clots in the veins.
-
I26.99: Pulmonary embolism (PE) without acute cor pulmonale (a clot in the lung)
-
I82.409: Acute deep vein thrombosis (DVT) of unspecified proximal lower extremity (a clot in a deep vein, usually the leg)
-
-
History of VTE: Once a patient has had a clot, they may be on lifelong therapy to prevent another one.
-
Z86.71: Personal history of venous thrombosis and embolism
-
-
Mechanical Heart Valves: These prosthetic valves significantly increase the risk of clots forming on them.
-
Z95.2: Presence of prosthetic heart valve
-
Z95.3: Presence of xenogenic heart valve (tissue valve) – Note: tissue valves often don’t require long-term anticoagulation, but sometimes do in the initial period or if other risk factors are present.
-
-
Other Hypercoagulable States: Some patients have genetic or acquired conditions that make their blood more likely to clot.
-
D68.59: Other primary thrombophilia (e.g., Factor V Leiden mutation)
-
D68.69: Other thrombophilia (e.g., Antiphospholipid syndrome)
-
Putting It All Together: Proper Code Sequencing
Now that we have our main characters—the medication code (Z79.01), the adverse effect codes (T45.515A, R79.1), and the underlying condition codes (I48.91, etc.)—we need to put them in the correct order. Code sequencing is the grammar of medical billing; it tells the story in the right order.
The general rule is: Code the reason for the encounter first. Then, list any other relevant codes that apply to the patient’s overall health.
Let’s look at some realistic patient scenarios.
Real-World Case Studies
Case Study 1: The Stable Patient
-
Patient: Martha, an 82-year-old woman with chronic atrial fibrillation.
-
Encounter: She comes to your clinic for her scheduled 4-week INR check. She feels well, has no complaints, and her INR is 2.3.
-
The Story: The reason for today’s visit is to monitor her long-term anticoagulant medication. Her underlying condition is atrial fibrillation.
-
Correct Coding:
-
Z79.01 (Long-term (current) use of anticoagulants)
-
I48.91 (Atrial fibrillation)
-
Case Study 2: The Slightly Unstable Patient
-
Patient: David, a 68-year-old man with a mechanical aortic heart valve.
-
Encounter: He comes for a routine INR check. He feels fine, but his INR result is 3.9. There are no signs of bleeding.
-
The Story: The reason for the visit was routine monitoring, but the encounter resulted in the finding of an elevated INR (an abnormal coagulation profile) requiring a dose adjustment. The adverse effect isn’t severe enough to warrant the T45 code.
-
Correct Coding:
-
Z79.01 (Long-term (current) use of anticoagulants)
-
R79.1 (Abnormal coagulation profile)
-
Z95.2 (Presence of prosthetic heart valve)
-
Case Study 3: The Patient with an Adverse Effect
-
Patient: Eleanor, a 75-year-old with a history of PE, now on warfarin.
-
Encounter: She calls because she has noticed significant bruising and her gums are bleeding when she brushes her teeth. You bring her in for an urgent check, and her INR is 6.1.
-
The Story: The reason for this urgent encounter is the adverse effect of her anticoagulant medication (over-anticoagulation leading to bleeding tendency). Her history of PE explains why she is on the drug.
-
Correct Coding:
-
T45.515A (Adverse effect of anticoagulants, initial encounter)
-
Z86.71 (Personal history of venous thrombosis and embolism)
-
Note: You might also code the specific manifestation, like R04.0 (Epistaxis) for nosebleeds or K92.2 (Gastrointestinal hemorrhage) if that were the case, but for gum bleeding, R79.1 for the abnormal coagulation profile is often sufficient as a secondary code to T45.515A.
-
Case Study 4: The New Start
-
Patient: James, a 60-year-old man newly diagnosed with a DVT in his leg.
-
Encounter: He is in the hospital, and you are initiating warfarin therapy. You will be checking his INR frequently to get him into a therapeutic range.
-
The Story: The reason for the encounter is the treatment of the acute DVT. The PT/INR monitoring is a part of that treatment.
-
Correct Coding (for a follow-up visit after discharge):
-
Z79.01 (Long-term (current) use of anticoagulants) – Once he is discharged and on the medication, this becomes the primary reason for monitoring visits.
-
Z86.71 (Personal history of venous thrombosis and embolism)
-
Billing Nuances for Different Settings
Where the test takes place can also influence the billing process. Let’s look at a few common scenarios.
In the Clinic/Office Setting
This is the most straightforward setting. You perform the blood draw via fingerstick, run the test on a point-of-care (POC) machine, and interpret the result, often adjusting the warfarin dose on the spot.
-
ICD-10 Codes: As described in the case studies above.
-
CPT Code: You would bill for the test itself. The most common code for POC PT/INR testing is 85610 (Prothrombin time).
-
Considerations: Some payers, including Medicare, may have specific rules about incident-to billing if a nurse or medical assistant performs the test under a physician’s supervision. Ensure your supervision meets the requirements.
Home INR Monitoring
Medicare covers home PT/INR monitoring for certain patients with mechanical heart valves or chronic atrial fibrillation who meet specific criteria. This allows the patient to test themselves at home.
-
ICD-10 Codes: The diagnosis coding remains the same. You are still monitoring a patient on long-term anticoagulants (Z79.01) for their underlying condition (e.g., I48.91). You must have the qualifying diagnosis on file.
-
CPT Code: This is billed differently, often using G0248 (Demonstration, prior to initiation of home INR monitoring, for patient with mechanical heart valve), G0249 (Provision of test materials and equipment for home INR monitoring), and G0250 (Physician review, interpretation, and patient management of home INR testing). These are specific Medicare G-codes.
Anticoagulation Clinic Management
If you work in a dedicated anticoagulation clinic, you are likely providing a higher level of management. In this case, you may be billing for a separate service in addition to the test.
-
ICD-10 Codes: Your diagnosis coding follows the same logic: Z79.01 + underlying condition code, or T45.515A for an adverse effect.
-
CPT Code: You would still bill 85610 for the test. Additionally, you might bill a separate Evaluation and Management (E/M) code (like 99212-99215) if the visit involves significant, medically necessary management beyond simply reporting the INR and adjusting the dose. This is a complex area, and you must ensure the documentation supports a separate, billable E/M service.
Common Billing Mistakes and How to Avoid Them
Even experienced billers can trip up on PT/INR claims. Here are some common pitfalls to watch out for.
-
Mistake #1: Using a V58.61 or similar old code. If you are still thinking in terms of ICD-9, you might be tempted to use outdated codes. The fix: Embrace Z79.01. It is the modern, accurate code for this situation.
-
Mistake #2: Only using the underlying condition code. Billing only I48.91 (atrial fibrillation) for a PT/INR check doesn’t tell the full story. It doesn’t explain why the test is being done today. The fix: Always include Z79.01 to connect the test to the medication management.
-
Mistake #3: Failing to distinguish between routine and acute. Using Z79.01 for a patient with a critical INR of 8.0 is a major error. It understates the severity of the encounter and could be seen as upcoding if you later bill a higher-level visit, but it’s clinically inaccurate. The fix: If the INR is dangerously out of range or the patient is symptomatic, switch to the adverse effect code T45.515A.
-
Mistake #4: Not documenting the dose change. For Medicare, the medical necessity of the test is often proven by the action you take. If the INR is out of range and you don’t adjust the dose, you need a very good reason documented (e.g., “Patient to hold dose tonight per protocol, will recheck in 2 days”). The fix: Always document your interpretation of the result and your plan of care, especially any changes to the warfarin dosage.
-
Mistake #5: Forgetting the “7th character” for adverse effect codes. Codes in the T45 section require a 7th character. Using T45.515 is incomplete. The fix: Remember:
-
A = initial encounter (active treatment)
-
D = subsequent encounter (routine follow-up after the adverse effect has been treated)
-
S = sequela (for late effects, which is rare in this context)
-
The Future of Anticoagulation and Coding
The world of anticoagulation is changing. Newer medications like apixaban (Eliquis), rivaroxaban (Xarelto), and edoxaban (Savaysa) are often preferred over warfarin because they don’t require routine blood monitoring. These are the Direct Oral Anticoagulants (DOACs).
For patients on these medications, the coding landscape is different. You would use Z79.01? No. There are separate codes for DOACs.
-
Z79.01 is specifically for anticoagulants (historically and primarily referring to warfarin and heparin).
-
For DOACs, you use Z79.02 (Long-term (current) use of antithrombotics/antiplatelets).
Key Distinction: Z79.01 = Warfarin (needs monitoring). Z79.02 = DOACs and antiplatelets like Plavix (generally do not need routine INR monitoring).
This is an important distinction to make. Billing a PT/INR test with Z79.02 would be a red flag for Medicare, as it’s not medically necessary to routinely monitor a patient on a DOAC with this test. The codes are designed to reflect the different management requirements of these medications.
Conclusion: Mastering the Code for Successful Reimbursement
Successfully billing Medicare for PT/INR monitoring comes down to telling a clear, consistent, and accurate story with your codes. The journey from finger stick to claim payment is built on the foundation of medical necessity, and the ICD-10 code is your primary tool for demonstrating it.
-
For the stable patient on warfarin, Z79.01 is your trusted workhorse, supported by the code for their underlying condition.
-
When the numbers go awry, switch to the acute codes like T45.515A or R79.1 to accurately reflect the complexity of the encounter.
-
Never forget to document your clinical decision-making—the dose adjustment, the patient education, the follow-up plan—to support the story your codes are telling.
Mastering these few key codes and the logic behind their use will dramatically reduce your claim denials, ensure you are appropriately reimbursed for your valuable work, and, most importantly, allow you to focus on what truly matters: keeping your patients safe on their therapy.
Frequently Asked Questions (FAQ)
1. Can I use Z79.01 for a patient just starting warfarin?
Yes, once the patient is discharged from the hospital or the initial treatment phase is complete and they are on a maintenance regimen at home. For follow-up visits specifically for INR monitoring after the drug has been prescribed, Z79.01 is appropriate.
2. What is the difference between using R79.1 and T45.515A?
Think of it as a spectrum. R79.1 (Abnormal coagulation profile) is for an INR that is out of range but not dangerously so, and the patient is asymptomatic. T45.515A (Adverse effect) is for a more significant event—a critically high or low INR, or the presence of actual bleeding or clotting symptoms related to the drug.
3. Do I need to list the underlying condition code every time?
While not absolutely mandatory in every single case, it is best practice. It provides a complete clinical picture and justifies the long-term use of the anticoagulant. Most Medicare Administrative Contractors (MACs) expect to see it.
4. My patient is on warfarin for a condition that has resolved (e.g., a post-surgical DVT). What code do I use?
If the acute condition has resolved but the patient remains on warfarin to prevent a recurrence, you should use the “personal history” code, such as Z86.71 for personal history of venous thrombosis, along with Z79.01.
5. What CPT code do I use for the finger-stick PT/INR test?
The standard code is 85610 (Prothrombin time). Some payers may have specific HCPCS codes for point-of-care testing, so it’s always good to verify with your local Medicare contractor, but 85610 is widely accepted.
Additional Resource
For the most up-to-date information on Medicare coverage policies, it’s always best to consult the source. You can find your local Medicare Administrative Contractor’s (MAC) policies by visiting the CMS website. A great starting point is the CMS Coverage Database, where you can search for Local Coverage Determinations (LCDs) related to “Prothrombin Time” or “INR Monitoring” in your specific jurisdiction.
Disclaimer:
The information provided in this article is for general informational purposes only and does not constitute legal, billing, or medical advice. Coding and billing rules, especially those concerning Medicare, are complex and subject to change. While we strive to keep the information accurate and up-to-date, we make no representations or warranties of any kind, express or implied, about the completeness, accuracy, reliability, or suitability of this information. You should always consult with a qualified professional, such as a certified professional coder (CPC) or a healthcare attorney, for advice tailored to your specific situation. Reliance on any information provided in this article is solely at your own risk.





