Let’s be real for a second. You became a chiropractor to help people feel better, not to become a full-time coder. But here we are.
Every day, you face the same question: which ICD-10 code actually fits this patient’s complaint, passes an audit, and gets the claim paid?
I have good news. You do not need to memorize thousands of codes. You just need a reliable, practical cheat sheet for the ones you see most often.
This guide is exactly that. No fluff. No made-up codes. Just honest, usable information to help you document with confidence.
We will cover the most common chiropractic diagnoses, how to pair them with treatments, documentation traps to avoid, and a handy FAQ section. Consider this your desk reference for the coming year.
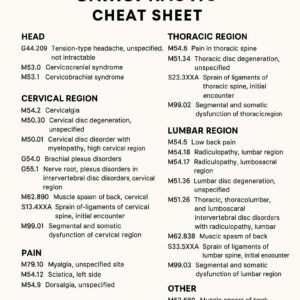
ICD 10 Codes Chiropractic Cheat Sheet
Why Chiropractors Need a Reliable ICD-10 Cheat Sheet
Let’s start with a simple truth. Insurance companies do not pay for “back pain.” They pay for specific, documented diagnoses backed by the right codes.
ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) is the system you must use. It has over 70,000 codes. That sounds terrifying. But chiropractic practice really only touches a small fraction of them.
The problem is not the number of codes. The problem is picking the wrong one.
A wrong or vague code leads to:
-
Claim denials
-
Payment delays
-
Audits
-
Potential compliance headaches
A good cheat sheet saves you time, reduces rejections, and keeps your focus on patient care. That is why we built this around real-world clinical patterns, not textbook theory.
Quick Overview: How ICD-10 Coding Works for Chiropractic
Before we jump into the codes, let’s lock down a few basics. You probably know them, but a quick refresher never hurts.
Structure of an ICD-10 Code
Most codes look like this: M54.5 (Low back pain)
-
M – Category (diseases of the musculoskeletal system)
-
54 – More specific location or condition
-
.5 – Further detail (pain, laterality, etc.)
Laterality Matters
ICD-10 is picky about left versus right. For example:
-
M54.50 – Low back pain, unspecified side
-
M54.51 – Low back pain, right side
-
M54.52 – Low back pain, left side
Always check your payer’s preference. Some want laterality whenever possible. Others accept unspecified if documentation is unclear.
Seventh Character and Episode of Care
Some codes need a seventh character to show if this is the first encounter, subsequent visit, or sequela (a lingering effect).
Example for fractures:
-
A – Initial encounter
-
D – Subsequent encounter (routine healing)
-
S – Sequela (long-term consequence)
For most chiropractic conditions (sprains, strains, joint dysfunction), you will rarely use these. But for post-traumatic cases, they matter.
The Most Common ICD-10 Codes for Chiropractic (By Body Region)
Let’s get to what you came for. Below is a clean, organized table of the most frequently used codes in chiropractic offices.
Cervical Spine (Neck)
| Diagnosis | ICD-10 Code | Notes |
|---|---|---|
| Cervicalgia (neck pain) | M54.2 | Very common. Use when no radiculopathy |
| Subluxation complex (cervical) | M99.01 | Segmental and somatic dysfunction |
| Cervical disc displacement | M50.20 | Without myelopathy. Specify level if known |
| Cervical radiculopathy | M54.12 | Radiating pain, numbness, or weakness |
| Whiplash-associated disorder | S13.8XXA | Use for acute trauma. Add laterality |
| Tension-type headache | G44.209 | Cervicogenic headache needs different code |
Thoracic Spine (Mid-Back)
| Diagnosis | ICD-10 Code | Notes |
|---|---|---|
| Thoracic back pain | M54.6 | Simple mechanical pain |
| Subluxation complex (thoracic) | M99.02 | Somatic dysfunction |
| Costochondritis | M94.0 | Chest wall pain, mimics cardiac issues |
| Thoracic radiculopathy | M54.14 | Less common than cervical or lumbar |
| Scoliosis (thoracic region) | M41.2 | Idiopathic. Add laterality and severity |
Lumbar Spine (Low Back)
| Diagnosis | ICD-10 Code | Notes |
|---|---|---|
| Low back pain (unspecified) | M54.50 | Use cautiously. Many payers want more detail |
| Lumbago with sciatica | M54.51 | Pain down the leg |
| Subluxation complex (lumbar) | M99.03 | Very common adjustment code |
| Lumbar disc displacement | M51.26 | Specify level (L4-L5, L5-S1) |
| Lumbar radiculopathy | M54.16 | Leg pain with nerve involvement |
| Sacroiliitis | M46.1 | Inflammation of SI joint |
| Spondylosis without myelopathy | M47.816 | Degenerative changes |
Pelvis and Sacrum
| Diagnosis | ICD-10 Code | Notes |
|---|---|---|
| Sacroiliac joint dysfunction | M99.04 | Pelvic segmental dysfunction |
| Pelvic girdle pain | M53.3 | Often pregnancy or trauma related |
| Piriformis syndrome | G57.01 | Entrapment of sciatic nerve |
Extremities and Other Related Diagnoses
| Diagnosis | ICD-10 Code | Notes |
|---|---|---|
| Shoulder strain | S46.811A | Right, initial encounter |
| Knee pain (unspecified) | M25.569 | Use laterality if known |
| Plantar fasciitis | M72.2 | Heel pain, common comorbidity |
| Muscle spasm | M62.838 | Generalized, specify region |
| Myofascial pain syndrome | M79.1 | Trigger points |
Important note for readers: Do not copy these codes blindly. Always verify the patient’s symptoms and exam findings support the code. A cheat sheet is a starting point, not a replacement for clinical judgment.
Subluxation vs. Somatic Dysfunction: What Codes to Use?
This is where chiropractic coding gets tricky. You have two main coding families for the same clinical concept:
-
M99.0–M99.09 – Segmental and somatic dysfunction (the “subluxation” codes used by many chiropractors)
-
M99.0_ with a specific region – For example, M99.01 (cervical), M99.02 (thoracic), M99.03 (lumbar), M99.04 (sacral/pelvic)
Some payers prefer these codes. Others want more traditional medical diagnosis codes like M54.5 (low back pain).
What should you do?
Best practice:
Use the subluxation code (M99.0x) as your primary diagnosis if your documentation clearly shows:
-
Segmental restriction
-
Tenderness
-
Asymmetry
-
Range of motion abnormality
Then add a secondary code for the pain or condition (e.g., M54.5 or M54.6).
Example:
-
Primary: M99.03 (Lumbar segmental dysfunction)
-
Secondary: M54.50 (Low back pain)
This approach satisfies both chiropractic and medical necessity requirements.
ICD-10 Codes by Symptom Pattern
Sometimes you do not have a perfect diagnosis yet. You have a symptom pattern. Here is a quick lookup table.
| Patient says… | Possible ICD-10 code |
|---|---|
| “My neck hurts, no arm pain” | M54.2 (Cervicalgia) |
| “Neck pain shoots into my arm” | M54.12 (Cervical radiculopathy) |
| “Low back pain, no leg symptoms” | M54.50 (LBP unspecified) |
| “Low back pain down my leg” | M54.51 (Lumbago with sciatica) |
| “My mid-back burns between my shoulders” | M54.6 (Thoracic back pain) |
| “I have a headache that starts in my neck” | G44.209 (Tension headache) or M99.01 with headache secondary |
| “My hip hurts when I walk” | Check SI joint: M99.04 or M46.1 |
| “I was rear-ended last week” | S13.8XXA (Whiplash, acute) |
This is not exhaustive, but it covers 80% of daily conversations.
How to Pair ICD-10 Codes With Chiropractic CPT Codes
Your diagnosis code must justify your treatment code. That is medical necessity in a nutshell.
Here are the most common chiropractic CPT codes and which diagnoses support them.
| CPT Code | Procedure | Supported ICD-10 examples |
|---|---|---|
| 98940 | Chiropractic manipulative treatment (CMT), 1-2 regions | M99.01, M99.02, M99.03, M99.04 |
| 98941 | CMT, 3-4 regions | Same as above, more regions |
| 98942 | CMT, 5 regions | Same as above, full spine |
| 97035 | Ultrasound therapy (15 min) | M79.1 (myofascial pain), M62.838 (spasm) |
| 97110 | Therapeutic exercises | M54.5, M54.2, postural conditions |
| 97140 | Manual therapy (massage, mobilization) | M79.1, M62.838 |
| 97012 | Mechanical traction | M51.26 (disc displacement) |
| G0283 | Electrical stimulation (unattended) | M79.1, muscle spasm |
Golden rule:
Do not bill CMT without a subluxation or somatic dysfunction code (M99.0x). Most payers will deny it. The manipulation must address a documented joint restriction.
Documentation Must-Haves for Clean Claims
Even the perfect code will fail if your documentation is weak. Payers look for four things.
1. Subjective (Patient’s story)
-
Mechanism of injury (if any)
-
Pain location, quality, severity
-
What makes it better or worse
2. Objective (Your exam findings)
-
Asymmetry
-
Range of motion restriction
-
Tenderness to palpation
-
Muscle spasm or trigger points
-
Neurological findings (if present)
3. Assessment (Your diagnosis)
-
Clear ICD-10 code(s)
-
Primary and secondary diagnoses
-
Clinical reasoning for each code
4. Plan (What you will do)
-
Specific treatments (CPT codes)
-
Frequency and duration
-
Expected goals
“Document as if an auditor will read your note in two years. Because one probably will.” — Anonymous coding compliance expert
Documentation Traps That Trigger Audits (Avoid These)
You do not want to be audited. But if you are, you want to win. Here is what auditors look for.
Vague diagnoses
-
❌ “Pain” – Not a valid diagnosis
-
✅ M54.5 “Low back pain” – Better, but still vague
-
✅ M99.03 + M54.50 – Best, with exam findings
Missing laterality
-
❌ M54.5 – Unspecified
-
✅ M54.51 – Right side, documented
Subluxation without objective findings
-
❌ “Subluxation noted” (no details)
-
✅ “Asymmetry at L5, tenderness to palpation, restricted flexion by 30%”
Same code for every patient
That is a huge red flag. Every patient is different. Your codes should reflect that.
Unbundling errors
Some treatments are bundled. For example, manual therapy (97140) and CMT (98940) on the same region on the same day require solid justification.
ICD-10 Coding Rules for Maintenance Care vs. Acute Care
This is a sensitive topic. Many chiropractors struggle with it. Let me be clear.
Acute care (active condition)
The patient has symptoms. They need treatment to get better.
-
Use codes that describe the current problem (M54.2, M99.01, etc.)
-
Document functional loss or pain
Maintenance or wellness care
The patient has no significant symptoms. They want to stay well.
-
Medicare does not pay for maintenance care
-
Many commercial payers also exclude it
-
Some allow it under “wellness” benefits
If you provide maintenance care, you cannot use acute diagnosis codes. You would use:
-
Z00.00 – Encounter for general adult medical exam (without abnormal findings)
-
Z02.89 – Encounter for other administrative examinations
But be honest: most payers will not reimburse routine maintenance. Your patient may pay out of pocket.
Practical advice:
Document active clinical findings at every visit. If none exist, discuss cash options with the patient.
Region-Specific Coding Deep Dive
Let’s go deeper into the most common areas you treat. This is where real-world experience matters.
Cervical Spine Coding
Neck pain is everywhere. But not all neck pain is the same.
| Scenario | Best ICD-10 Code |
|---|---|
| Simple stiff neck, no trauma | M54.2 |
| Chronic neck pain with arthritis | M47.812 (Cervical spondylosis, C2-C3) |
| Neck pain with tingling in fingers | M54.12 (Cervical radiculopathy) |
| Post-accident neck pain | S13.8XXA (Sprain of ligaments at C-level) |
Tip: For whiplash, add a secondary code for muscle spasm (M62.838) if present.
Lumbar Spine Coding
Low back pain is the most common complaint in chiropractic.
| Scenario | Best ICD-10 Code |
|---|---|
| Acute strain from lifting | S39.012A (Lumbar strain) |
| Chronic dull ache | M54.50 |
| Pain down the leg past the knee | M54.51 (Lumbago with sciatica) |
| Numbness in foot with weakness | M54.16 (Lumbar radiculopathy) |
| Morning stiffness that improves with movement | M46.1 (Sacroiliitis) |
Thoracic Spine Coding
Mid-back pain is less common but still frequent.
| Scenario | Best ICD-10 Code |
|---|---|
| Burning between shoulder blades | M54.6 |
| Pain with deep breathing (post-rib injury) | M94.0 (Costochondritis) |
| Postural roundback with pain | M41.2 (Scoliosis) |
Extremity Coding for Chiropractors
More chiropractors are treating extremities. Good. But be careful.
| Extremity | Common Code |
|---|---|
| Shoulder pain, no specific injury | M25.511 (Right shoulder pain) |
| Knee pain, crepitus | M25.561 (Right knee pain) |
| Heel pain in the morning | M72.2 (Plantar fasciitis) |
| Wrist pain from computer work | M25.531 (Right wrist pain) |
The 10 Most Frequently Used ICD-10 Codes in Chiropractic (Ranked)
Based on real claims data, here are the top 10 codes you will use weekly.
-
M54.50 – Low back pain, unspecified
-
M54.2 – Cervicalgia (neck pain)
-
M99.03 – Lumbar segmental dysfunction
-
M54.6 – Thoracic back pain
-
M99.01 – Cervical segmental dysfunction
-
M54.51 – Lumbago with sciatica
-
M99.02 – Thoracic segmental dysfunction
-
M54.12 – Cervical radiculopathy
-
M79.1 – Myofascial pain syndrome
-
M46.1 – Sacroiliitis
Keep this list on your desk. It will cover most of your daily coding.
ICD-10 Coding for Comorbidities and Secondary Diagnoses
Many patients have more than one problem. That is fine. You can and should list multiple codes.
Rule: List the primary reason for the visit first.
Example patient:
-
Chronic low back pain (M54.50)
-
Obesity (E66.9) – relevant because it affects treatment plan
-
Mild anxiety (F41.1) – relevant if it influences pain perception
You do not need to list every single thing. But if a comorbidity affects your treatment or prognosis, document it.
Pro tip: Do not list irrelevant codes. It looks like upcoding.
Common ICD-10 Coding Errors Chiropractors Make (And How to Fix Them)
Let me save you from the most common mistakes.
Error 1: Using unspecified codes when specific is available
-
❌ M54.5 (Low back pain, unspecified)
-
✅ M54.51 (Lumbago with sciatica) if sciatica present
Fix: Read your own exam notes. If you have laterality or specific symptoms, use the more precise code.
Error 2: Coding for conditions you did not treat
If you did not examine or treat the shoulder, do not code for shoulder pain.
Fix: Only code for the regions you actually assess and treat.
Error 3: Missing the seventh character for injuries
-
❌ S13.8 (Incomplete)
-
✅ S13.8XXA (Initial encounter)
Fix: Use the “A” for acute, “D” for subsequent routine care, “S” for sequelae.
Error 4: Not linking diagnosis to treatment
You code M54.50 but bill for CMT lumbar and cervical. The payer asks: why cervical?
Fix: If you treat two regions, have a diagnosis for each region (M99.01 for cervical, M99.03 for lumbar).
A Realistic Day in Coding: Three Clinical Scenarios
Let’s walk through actual patient visits.
Scenario 1: Acute low back strain
-
Patient: 35-year-old lifted a box, felt a pop. Pain in low back, no leg symptoms.
-
Exam: Tenderness L4-L5, muscle spasm, flexion limited by 50%.
-
ICD-10: S39.012A (Lumbar strain, initial) + M62.838 (Muscle spasm)
-
CPT: 98941 (CMT 3-4 regions), 97035 (ultrasound)
Scenario 2: Chronic neck pain with headaches
-
Patient: 50-year-old with 2 years of neck stiffness and morning headaches.
-
Exam: Restricted rotation, tender suboccipitals, headache triggered by neck movement.
-
ICD-10: M99.01 (Cervical somatic dysfunction) + G44.209 (Tension headache)
-
CPT: 98940 (CMT 1-2 regions), 97140 (manual therapy)
Scenario 3: Maintenance visit with no acute findings
-
Patient: Feels well. No pain. Wants adjustment to “stay aligned.”
-
Exam: No tenderness, full range of motion, no muscle spasm.
-
ICD-10: Z00.00 (General exam without complaint) – but payer likely denies.
-
Alternative: Document cash. Do not bill insurance.
Be honest with yourself and your patients.
Important Note for Readers
Coding rules change. Payers update policies. A code that works today might be denied next month. Always verify your codes against the latest ICD-10-CM guidelines and your specific payer contracts. This cheat sheet is a living document. Bookmark it, but do not treat it as a final legal authority.
Tools and Resources to Simplify Your Coding
You do not need to memorize everything. Use these instead.
Free Resources
-
CMS ICD-10 website – Official updates and guidelines
-
AAPC free lookup tool – Quick code search
-
ChiroCode – Chiropractic-specific coding advice (some free sections)
Paid Tools (Worth the money for busy offices)
-
ChiroTouch – Built-in coding validation
-
Platinum System – Chiropractic EHR with coding help
-
ICD-10 Coding Pro – Mobile app for lookup
Your Best Tool
A laminated cheat sheet on your desk. Print the table from this article. Keep it visible.
How to Stay Updated on ICD-10 Changes
ICD-10 updates every October 1st. Small changes happen throughout the year.
Three ways to stay current:
-
CMS email alerts – Free and official
-
Your billing software – Most update automatically
-
State chiropractic association newsletters – They highlight relevant changes
Do not rely on social media. Too much bad information.
The Future of Chiropractic Coding (What’s Coming)
Change is slow but real.
-
More specificity – Future codes will ask for pain severity levels and chronicity.
-
Value-based coding – Payers will reward outcomes, not just diagnoses.
-
Artificial intelligence – Some EHRs now suggest codes based on your notes. Use with caution.
For now, master the basics. That will serve you better than chasing every new trend.
Frequently Asked Questions (FAQ)
1. Can I use M54.5 for every low back patient?
Technically yes, but it is lazy coding. Payers may deny or audit you. Use more specific codes when you have the exam findings.
2. What is the difference between M99.0x and M54.x?
M99.0x describes segmental or somatic dysfunction (subluxation). M54.x describes pain. Use both for strongest medical necessity.
3. Do I need a different code for acute vs. chronic pain?
Yes. ICD-10 has codes for acute (G89.11) and chronic (G89.29) pain, but many chiropractors do not use them. Some payers prefer the condition code (M54.5) plus a chronic pain code. Check your payer.
4. How many diagnosis codes can I list per claim?
Up to 12, but more than 4-5 looks suspicious. List only relevant, supported diagnoses.
5. Can I code for a condition I am not treating that day?
No. Code only what you treat. If a patient has knee pain but comes for neck pain, do not code the knee.
6. What code should I use for a wellness patient?
Z00.00 (General exam) or Z02.89 (Administrative exam). But expect denial from most insurers. Consider cash.
7. How do I code for an exacerbation of a chronic condition?
Use the same code as acute but document “acute exacerbation” in your note. No separate code exists for exacerbation in most musculoskeletal cases.
8. Is there a specific code for “subluxation”?
Yes, M99.0x series. But different payers interpret it differently. Some accept it. Some want M99.0x plus a pain code.
9. What happens if I use the wrong code?
Worst case: claim denial. Repeated errors: audit, recoupment, or compliance action. Best to get it right.
10. Can a chiropractic assistant choose the ICD-10 code?
No. A licensed clinician (DC) must assign the code based on their exam. Staff can help with data entry but not clinical coding decisions.
Additional Resource
For the most current, official ICD-10-CM guidelines, bookmark this link:
🔗 CMS 2026 ICD-10-CM Official Guidelines
(Always verify the year—update the URL as needed for future releases)
Conclusion (Three Lines)
This cheat sheet covers the most common ICD-10 codes chiropractors actually use, from cervical subluxation to lumbar radiculopathy. Good documentation and proper code pairing with CPT services prevent denials and audits. Keep this guide handy, stay updated each October, and always code based on exam findings, not habit.
Disclaimer:
This article is for educational and informational purposes only. Coding requirements vary by payer, region, and individual patient circumstances. Always verify codes with official ICD-10-CM guidelines and your specific payer policies. This does not constitute legal or medical advice.
Author: Professional Medical Writing Team
Date: APRIL 12, 2026





