If you have ever looked at a Medicare Summary Notice (MSN) or spoken to a medical biller, you know that healthcare runs on codes. It is a language of its own. For something as common as checking your cholesterol—medically known as a lipid panel—there is a specific set of rules that dictates whether Medicare will pay for it and how the doctor must justify it.
This guide is designed to cut through the confusion. We are going to look specifically at the ICD-10 code for lipid panel Medicare requirements. Whether you are a healthcare provider trying to clean up your billing process, a medical coder, or a patient trying to understand a bill, this article will break down the logic, the codes, and the “why” behind the paperwork.
We will keep things simple. No complex medical jargon for the sake of it. Just clear, honest information about how to document cholesterol testing for the millions of Americans covered by Medicare.
ICD-10 Codes for Lipid Panels and Medicare
What is a Lipid Panel and Why Does Medicare Care?
Before we dive into the codes, let’s look at the test itself. A lipid panel is a blood test that measures your cholesterol levels. It usually includes:
-
Total Cholesterol: The overall amount of cholesterol in your blood.
-
LDL Cholesterol (Low-Density Lipoprotein): Often called the “bad” cholesterol because it can build up in the walls of your arteries.
-
HDL Cholesterol (High-Density Lipoprotein): Known as the “good” cholesterol, as it helps carry away LDL.
-
Triglycerides: A type of fat in the blood that stores excess energy from your diet.
Medicare cares about this test because cardiovascular disease is one of the leading health issues in the United States. By monitoring these numbers, doctors can help prevent heart attacks and strokes. However, because Medicare is a federal program, it needs a reason to justify the cost of the test.
This is where the ICD-10 code comes in. The ICD-10 code is the “diagnosis code.” It tells Medicare, “This is the reason we are running this test.”
The Primary ICD-10 Code for Lipid Panel Medicare Reimbursement
When we talk about the most common scenario for a cholesterol test, we are usually talking about screening. This is a preventive measure to check for risk factors before a person has a major cardiac event.
For a routine screening lipid panel, specifically for Medicare patients, the most frequently used diagnosis code is:
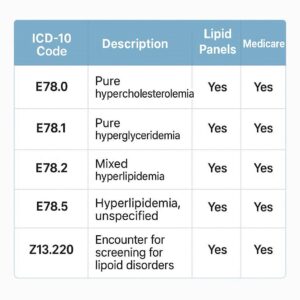
Z13.220 – Encounter for screening for lipoid disorders
This is the workhorse code. It tells the payer (Medicare) that the purpose of the visit or the test was to proactively look for lipid disorders (like high cholesterol) in a patient who does not currently have symptoms.
Why this code matters for Medicare:
Medicare Part B (Medical Insurance) covers cardiovascular screening blood tests. This includes testing cholesterol, lipid, and triglyceride levels. They cover these tests every five years. By using the code Z13.220, you are aligning the claim with Medicare’s preventive services benefits.
Important Note for Readers:
A “screening” code like Z13.220 implies the patient is asymptomatic. If the patient already has a diagnosis related to cholesterol, you generally should not use a screening code. Using the wrong code can lead to a denial, as Medicare will assume you are billing for a routine test that isn’t medically necessary at that frequency.
When It’s Not Just a Screening: Using Specific Diagnosis Codes
While Z13.220 is great for routine checks, it is not the only code used. In fact, once a patient has been diagnosed with a cholesterol problem, the game changes. You move from “screening” to “monitoring” or “treatment.”
If a doctor is monitoring a patient’s cholesterol to see if medication (like statins) is working, or if the patient has a history of high cholesterol, you need a more specific code.
Here are the common diagnosis codes used for lipid panels beyond the initial screening:
-
E78.00 – Pure hypercholesterolemia, unspecified: This is used when the patient has high cholesterol, but the specific type isn’t documented in detail.
-
E78.1 – Pure hyperglyceridemia: Used when the primary issue is high triglycerides.
-
E78.2 – Mixed hyperlipidemia: This is a very common code. It is used when a patient has both elevated cholesterol and elevated triglycerides.
-
E78.4 – Other hyperlipidemia: A catch-all for other specified lipid disorders.
-
E78.5 – Hyperlipidemia, unspecified: If the doctor simply writes “hyperlipidemia” in the chart without specifying, this is the code to use. However, coders should always aim for specificity when possible.
-
Z86.39 – Personal history of other endocrine, nutritional and metabolic disease: This can be used for a patient with a history of high cholesterol that has since resolved with lifestyle changes, but the doctor still wants to keep an eye on it.
Comparison: Screening vs. Monitoring Codes
To make this clearer, let’s look at the difference in a simple table.
| Scenario | What is happening? | Correct Code Type | Example Code |
|---|---|---|---|
| Initial Screening | Patient is 65, generally healthy. No history of high cholesterol. Doctor orders a panel as part of a wellness visit. | Screening (Z-Code) | Z13.220 |
| Monitoring Treatment | Patient was diagnosed with high cholesterol last year. Doctor prescribes Lipitor. Now, the doctor orders a new panel to see if the meds are working. | Diagnosis (E-Code) | E78.00 or E78.2 |
| Family History | Patient has normal levels, but both parents had heart disease. Doctor wants a baseline. | Screening (Z-Code) | Z13.220 (often linked with family history code Z84.89) |
| Post-Heart Attack | Patient had a heart attack 6 months ago. Doctor orders a lipid panel to ensure LDL is low enough to prevent another event. | Diagnosis (E-Code) or History (Z-Code) | E78.2 or Z86.39 |
The Connection to “Medical Necessity”
In the world of Medicare, “medical necessity” is everything. An ICD-10 code is not just a formality; it is the justification for the procedure code (the CPT code for the lab test itself).
For a lipid panel, the CPT code is usually something like 80061 (Lipid panel) or 82465 (Cholesterol test).
When the claim is submitted, Medicare’s systems check the diagnosis code (ICD-10) against the procedure code (CPT). If the diagnosis code doesn’t support the need for the test, the claim will be denied.
-
Good Pairing: CPT 80061 + ICD-10 E78.2 (Mixed hyperlipidemia). This makes sense. The patient has a known disease, and the doctor is checking on it.
-
Bad Pairing: CPT 80061 + ICD-10 Z13.220 submitted two years in a row. Medicare’s rules say screening is covered every five years. This claim will likely be denied as “duplicate” or “not medically necessary” because it is too soon for another screening.
Common Reasons for Denial
-
Frequency: Billing a screening lipid panel (Z13.220) too often (more than once every 5 years for a standard risk patient).
-
Mismatch: Using a screening code (Z13.220) for a patient who is already on cholesterol medication. This should be coded with the specific E-code for the condition being treated.
-
Unspecific Code: Using E78.5 (Hyperlipidemia, unspecified) when the medical record clearly shows the patient has mixed hyperlipidemia. Medicare prefers the most specific code available.
A Closer Look at Medicare Coverage Guidelines
Medicare’s coverage for cardiovascular screenings is defined under Section 1861(ww) of the Social Security Act. It is designed to help doctors detect conditions early.
What Medicare covers:
-
A screening lipid panel.
-
Once every 5 years.
-
No deductible or coinsurance for the test itself if the doctor accepts assignment (though you may pay for the doctor visit).
What this means for coding:
When you use Z13.220, you are signaling to Medicare that this is a preventive service meeting the 5-year rule. The system will check when the last test was done.
If the patient has a diagnosis like E78.2, the frequency rules change. There is no 5-year limit for monitoring an active condition. A doctor can order a lipid panel every few months if medically necessary to manage the disease. The ICD-10 code (the diagnosis) justifies the frequency.
How to Code for Patients with Multiple Conditions
It is very common for Medicare patients to have multiple health issues. Diabetes and high cholesterol often go hand in hand. So, how do you code that?
Let’s say a patient with Type 2 Diabetes comes in for a check-up. The doctor orders a lipid panel.
-
The patient has diabetes (E11.9).
-
The doctor also knows the patient has high cholesterol (E78.2).
In this case, you would typically list both diagnosis codes on the claim. The “primary” diagnosis might be the diabetes (E11.9) because that is the main reason for the visit, but the lab order for the lipid panel is supported by the secondary diagnosis of hyperlipidemia (E78.2).
Alternatively, if the patient is there specifically to review their cholesterol medication, the hyperlipidemia code (E78.2) would be listed first.
Real-World Scenarios for ICD-10 and Lipid Panels
Let’s walk through three typical patient visits to see how the coding works in practice.
Scenario A: The “Welcome to Medicare” Visit
Mr. Jones just turned 65 and enrolled in Medicare. He has his “Welcome to Medicare” preventive visit. He has no history of high cholesterol. His doctor orders a standard lipid panel.
-
Diagnosis: No current illness, just a preventive screening.
-
ICD-10 Code: Z13.220 (Encounter for screening for lipoid disorders)
-
Result: Covered under Medicare preventive services.
Scenario B: The Established Patient on Statins
Mrs. Smith has been taking Atorvastatin for three years for high cholesterol. She comes in for her semi-annual medication management appointment. The doctor orders a lipid panel to see if her LDL is controlled.
-
Diagnosis: Patient is currently being treated for a lipid disorder.
-
ICD-10 Code: E78.2 (Mixed hyperlipidemia) – based on her history.
-
Result: Covered as medically necessary for disease management. No 5-year rule applies.
Scenario C: The Post-Hospitalization Follow-up
Mr. Davis was hospitalized for a mild heart attack (I21.4) three months ago. He sees his cardiologist for a follow-up. The cardiologist orders a lipid panel to ensure his cholesterol is at a safe target level.
-
Diagnosis: History of heart attack, requiring aggressive lipid management.
-
ICD-10 Code: I21.4 (Non-ST elevation myocardial infarction) or Z86.39 (Personal history of metabolic disease) for the long-term management, along with E78.2 if his hyperlipidemia persists.
-
Result: Covered. This is standard post-cardiac event monitoring.
Helpful Lists: Do’s and Don’ts for Coders and Providers
To keep your claims clean and avoid headaches, here is a quick checklist.
Do’s for Accurate Coding
-
Do use Z13.220 for the initial baseline screening or routine 5-year checks on asymptomatic patients.
-
Do use the specific E78.- codes when a patient has an active diagnosis of a lipid disorder.
-
Do document everything. The medical record should support the code. If you use E78.2, the doctor’s note should mention both high cholesterol and high triglycerides.
-
Do check the patient’s history. Look back to see when their last lipid panel was done if you are billing a screening.
-
Do link the diagnosis code to the lab order in the patient’s chart.
Don’ts for Accurate Coding
-
Don’t use a screening code (Z13.220) for a patient on cholesterol medication. It is inaccurate and looks like you are trying to bypass the 5-year rule artificially.
-
Don’t use unspecified codes (E78.4, E78.5) if the doctor has specified the type of lipid disorder in the notes.
-
Don’t assume. If the doctor writes “hyperlipidemia,” code E78.5. But if they write “mixed hyperlipidemia,” use the more accurate E78.2.
-
Don’t ignore the “NCD” (National Coverage Determination). Medicare has specific rules about which tests are covered for which diagnoses.
Additional Resource: Where to Find Official Information
Navigating Medicare coding can feel like reading a map in a foreign language. While this guide provides a solid overview, the ultimate source of truth is the Centers for Medicare & Medicaid Services (CMS).
For the most up-to-date information on coverage, local coverage determinations (LCDs), and coding articles, you should visit the official CMS website.
[Click here to visit the official CMS.gov website for the latest Medicare National Coverage Determinations (NCDs)]
This resource allows you to search for specific policies, including those related to cardiovascular screening and lipid panels. It is the best way to ensure your billing practices are compliant with the latest federal guidelines.
Frequently Asked Questions (FAQ)
Here are answers to some of the most common questions about coding lipid panels for Medicare patients.
Q: Can I bill a lipid panel with a diagnosis of “Essential Hypertension” (I10)?
A: Yes, you can. Hypertension is a major risk factor for heart disease. Ordering a lipid panel for a patient with hypertension to assess their overall cardiovascular risk is considered medically necessary. However, it is important to note that if the patient is completely asymptomatic and the only reason is risk assessment due to hypertension, you would link the lab to the hypertension code (I10). Some payers may prefer a more direct metabolic code if available, but hypertension is a valid supporting diagnosis.
Q: What happens if I accidentally use the wrong ICD-10 code?
A: This depends on the error. If you use a code that doesn’t support medical necessity, Medicare will deny the claim. You will then have to resubmit it with a corrected code (an appeal or corrected claim). If it is a minor error, like using E78.5 instead of E78.2, the claim might still pay, but it is not best practice and could be flagged in an audit.
Q: Is Z13.220 the only code for screening?
A: For lipid disorders specifically, Z13.220 is the most direct and appropriate code. You might sometimes see Z13.89 (Encounter for screening for other disorder), but Z13.220 is preferred because it specifically names “lipoid disorders.”
Q: Does Medicare cover advanced lipid testing?
A: Standard lipid panels (CPT 80061) are covered. Advanced lipid testing (like LDL particle number) is usually considered not medically necessary for routine screening and is often denied by Medicare. It is typically only covered for specific, high-risk patients with documented medical necessity.
Q: My doctor wrote “R79.89” (Other specified abnormal findings of blood chemistry) for a lipid panel. Is that okay?
A: R79.89 is a “symptom” or “finding” code. It can be used if you are confirming an abnormal result found incidentally. However, it is not the best code for an initial screening or for managing a known condition. For standard purposes, stick to Z13.220 for screening and the E78 codes for diagnoses.
Conclusion
In summary, successful billing for cholesterol testing under Medicare hinges on understanding the distinction between prevention and treatment. The ICD-10 code for lipid panel Medicare claims is most commonly Z13.220 for routine screening once every five years. However, for patients actively managing a condition, the code shifts to the E78 series (such as E78.2 or E78.00), which reflects an active diagnosis and justifies more frequent monitoring. Always ensure your coding accurately reflects the patient’s medical record to support medical necessity.
Disclaimer
The information provided in this article is for general informational purposes only and does not constitute legal, billing, or medical advice. Coding and coverage guidelines are subject to change. While we strive to keep the information accurate and up-to-date, readers should consult with qualified professionals and review the official guidelines from the Centers for Medicare & Medicaid Services (CMS) and the American Medical Association (AMA) for the most current policies.





