So, you’re sitting in your consultation room, and you’ve just spent the last twenty minutes with a patient. You’ve listened to their symptoms, performed an examination, and reviewed their history. The conclusion is clear: this patient needs to see a specialist. Maybe it’s a cardiologist for that persistent heart murmur, a dermatologist for a suspicious mole, or an orthopedist for a chronic knee injury.
The medical decision is made. But then comes the administrative part that every healthcare provider, medical assistant, and coder knows all too well: the paperwork. Specifically, you need to generate a referral. And at the heart of that referral lies a critical piece of information: the diagnosis code.
You might be tempted to search for a single, magic bullet—an “icd 10 code for referral to specialist“—that you can slap on the form to make the process quick and easy.
Let’s clear this up right now: There is no specific ICD-10 code that means “referral to specialist.” The ICD-10 code set doesn’t work that way. It is a diagnostic tool, not a procedural one. Using a code that way would be like using a hammer to screw in a lightbulb—it’s the wrong tool for the job.
But don’t worry! This guide is here to help you navigate this exact situation. We’re going to break down what an ICD-10 code actually is, why it’s essential for referrals, and exactly how to choose the right one to ensure your patient gets the care they need without unnecessary administrative delays. Think of this as your friendly, comprehensive roadmap to mastering the art and science of the specialist referral.
We’ll cover everything from the “why” behind the coding to practical examples, common pitfalls, and answers to the most frequently asked questions. By the end of this article, you’ll feel confident that you’re not just filling out a form, but you’re telling a clear, accurate story about your patient’s health—a story that the specialist, the insurance company, and the billing department all need to hear.
Let’s dive in and demystify the process together.
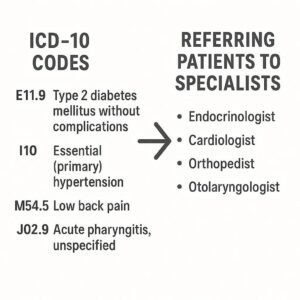
ICD-10 Codes and Referring Patients to Specialists
Table of Contents
ToggleWhat is an ICD-10 Code, Really? (And Why It Matters for Referrals)
Before we get into the specifics of referrals, it’s helpful to take a step back and understand what these codes actually are. ICD-10 stands for the International Classification of Diseases, 10th Revision. It’s a system of alphanumeric codes used by healthcare providers worldwide to classify and code all diagnoses, symptoms, and procedures.
Think of it as the universal language of medicine. When you write a diagnosis in English, like “Type 2 Diabetes Mellitus,” the corresponding ICD-10 code, E11. 9, translates that phrase into a standardized code that every insurance company, government health program, and hospital in the country (and many around the world) can understand instantly.
The Core Purpose: Diagnosis, Not Action
This is the most important concept to grasp. An ICD-10 code’s sole job is to answer the question: “What is wrong with the patient?” or “Why is the patient seeking care right now?”
It is not designed to answer:
-
“What procedure did the doctor perform?” (That’s CPT/ HCPCS codes).
-
“Where is the patient being sent?” (That’s a referral form).
-
“What type of doctor is the patient seeing?” (That’s provider data).
Therefore, the idea of an “icd 10 code for referral to specialist” is a misunderstanding of the code set’s function. The code describes the reason for the referral, not the referral itself.
Why the Right Code is Crucial for a Referral
When you send a patient to a specialist, that ICD-10 code serves several vital purposes:
-
Communicating the “Why”: It tells the specialist, in their own language, why you are sending the patient. It provides the clinical justification for the consult. For example, sending a patient to a gastroenterologist with the code R10. 9 (Unspecified abdominal pain) tells a very different story than sending them with K50. 90 (Crohn’s disease, unspecified). The specialist can then prepare for the visit accordingly.
-
Justifying Medical Necessity for Insurance: This is the big one. Insurance companies require proof that a specialist visit is “medically necessary.” The diagnosis code you provide is that proof. If the diagnosis doesn’t reasonably align with the specialist’s scope of practice, the insurance company may deny the claim.
-
Example: A referral to a cardiologist with the diagnosis code J02. 9 (Acute pharyngitis, unspecified) will almost certainly be denied. It doesn’t make medical sense. However, a referral to a cardiologist with I10 (Essential (primary) hypertension) is perfectly logical.
-
-
Ensuring Proper Payment: The specialist’s office will use your diagnosis code to guide their own coding and billing. An accurate initial code helps ensure that the services they provide are appropriately linked to a covered diagnosis, leading to correct reimbursement.
-
Tracking Public Health Data: On a larger scale, aggregated ICD-10 data helps public health officials track disease patterns, allocate resources, and conduct research.
In short, the ICD-10 code is the engine that drives the entire referral process. Without a valid, accurate, and specific code, the referral stalls.
The “Myth” of the Single Referral Code: Why It Doesn’t Exist
It’s a common thought. You’re busy, you have a stack of referrals to complete, and you wish there was just one code you could use for everything. But let’s explore why that’s impossible from a coding and compliance standpoint.
Z Codes: The Closest You’ll Get (But Still Not a Direct Match)
The ICD-10 system does have a section for “Factors influencing health status and contact with health services,” which are the Z codes (Z00-Z99). These codes are used when a person who is not currently sick encounters the health services for a specific purpose, such as a check-up, a screening, or to discuss a family history.
You might wonder if any of these Z codes fit the bill for a referral. Let’s look at a few:
-
Z01. 818 (Encounter for other specified special examinations): This might be used for a routine pre-employment physical, but it doesn’t capture the reason for a specialist referral.
-
Z02. 1 (Encounter for pre-employment examination): Again, very specific and not for a diagnostic referral.
-
Z71. 9 (Counseling, unspecified): This is too vague for a referral.
While you might use a Z code in conjunction with another diagnosis, it can never stand alone as the reason for a specialist referral. The specialist needs to know the suspected or confirmed condition, not just that the patient is there for a “check-up.”
The Danger of Using Vague or Incorrect Codes
What happens if you give in to the temptation to use a non-specific code just to get the referral out the door? The consequences can range from a minor annoyance to a major problem for your patient.
| Scenario | The Code Used | The Outcome |
|---|---|---|
| Patient with chronic cough | R05 (Cough) | The pulmonologist’s office accepts the referral. The patient waits two months for an appointment. When they arrive, the doctor has no idea if this is an allergic cough, an infectious cough, or a sign of something more serious like COPD. The patient may need to repeat many basic tests, delaying treatment. The insurance pays, but the care is less efficient. |
| Patient with a suspicious skin lesion | L98. 9 (Disorder of skin and subcutaneous tissue, unspecified) | The dermatologist’s scheduler sees the vague code. They call the patient to ask for more details. The patient is unsure. The scheduler puts the referral on hold to request more information from your office. This creates a back-and-forth that could take days or weeks. The patient’s anxiety grows. |
| Patient with intermittent chest pain | R07. 9 (Chest pain, unspecified) | The insurance company’s automated system reviews the claim. Chest pain can be a symptom of many things, including indigestion. Without a more specific link (like a history of hypertension or an abnormal EKG), the claim may be denied as not medically necessary for a cardiologist. The patient is left with a bill or a cancelled appointment. |
As you can see, using an incorrect or overly vague code creates friction. It slows down care, frustrates patients, and can even lead to financial headaches. The few seconds you save by not looking up the right code can cost you and your patient hours of administrative hassle later.
How to Choose the Right ICD-10 Code for a Specialist Referral
Now for the practical part. How do you actually choose the correct code? It’s a logical process that starts and ends with the patient in front of you. Follow this step-by-step guide.
Step 1: Identify the Primary Reason for the Referral
What is the single most important reason you are sending this patient to a specialist? This is your “primary diagnosis” or “principal diagnosis.” It should be the condition that demands the specialist’s attention.
-
Is it a confirmed diagnosis? For example, you’ve just diagnosed a patient with Rheumatoid Arthritis based on blood work and symptoms. You’re referring them to a rheumatologist for ongoing management. Your primary code is M06. 9 (Rheumatoid arthritis, unspecified).
-
Is it a suspected but unconfirmed diagnosis? You suspect a patient has Multiple Sclerosis based on their symptoms, but you need a neurologist to confirm it with an MRI and further testing. You cannot code for a disease they haven’t been diagnosed with. Instead, you code the symptoms.
-
Is it a sign or symptom? The patient presents with a problem, but the cause is unknown. You’re referring them to a specialist to find the cause.
Step 2: Be as Specific as the Medical Record Allows
ICD-10 is all about specificity. The more detail you have, the more specific your code can be. This is where your clinical documentation is key.
-
Laterality: Is it the left knee, the right knee, or both?
-
Acuity: Is it acute, chronic, intermittent, or recurrent?
-
Severity: Is it mild, moderate, or severe? (Sometimes coded separately).
-
Cause: Is it due to an external cause, like an injury?
Let’s look at an example of how specificity increases with better information:
| Level of Specificity | Patient Presentation | Diagnosis Description | ICD-10 Code |
|---|---|---|---|
| Lowest (Vague) | “My knee hurts.” | Pain in joint, unspecified | M25. 50 |
| Good | “My left knee has been hurting for a few weeks.” | Pain in left knee | M25. 56 |
| Better | “My left knee has been hurting for a few weeks after I twisted it playing tennis.” | Pain in left knee, initial encounter | M25. 561 (and a separate external cause code for the tennis injury) |
| Best (Specific) | “I have chronic pain and stiffness in my left knee due to osteoarthritis, which was confirmed by an x-ray last year.” | Osteoarthritis of left knee | M17. 12 (Unilateral primary osteoarthritis, left knee) |
As you move down the table, the code becomes a more powerful tool for communication and justification.
Step 3: Code for Signs and Symptoms When a Diagnosis Isn’t Confirmed
This is a critical rule, especially for referrals. If you have a confirmed diagnosis, use it. If you don’t, you must code the signs and symptoms that you do know.
This is not a sign of failure; it’s a sign of good medicine. You are accurately reflecting the patient’s state at the time of the referral.
-
Scenario: A patient presents with chronic, watery diarrhea, abdominal cramping, and unintentional weight loss over the past three months. You suspect Inflammatory Bowel Disease (IBD), but you haven’t done a colonoscopy to confirm it.
-
Incorrect Coding: K51. 90 (Ulcerative colitis, unspecified). You have not diagnosed this. If the insurance company sees this, and the gastroenterologist finds something else, it could be flagged as a misrepresentation.
-
Correct Coding:
-
R19. 7 (Diarrhea, unspecified)
-
R10. 84 (Generalized abdominal pain)
-
R63. 4 (Abnormal weight loss)
-
These three codes paint an accurate picture of the patient’s condition and perfectly justify the need for a gastroenterology consult. The specialist will then perform their own evaluation to arrive at the final diagnosis.
Common Examples: Finding the Right Code for Your Referral
Let’s put this into practice with some common clinical scenarios. This table provides a quick reference for matching a patient’s story to the appropriate ICD-10 code for a referral.
| Patient Presentation / Reason for Referral | Specialist | Correct ICD-10-CM Code(s) | Code Description |
|---|---|---|---|
| Established patient with confirmed Type 2 Diabetes, poorly controlled. | Endocrinologist | E11. 9 | Type 2 diabetes mellitus without complications |
| Patient with a suspicious, changing mole on their back. | Dermatologist | D23. 5 | Other benign neoplasm of skin of trunk (if it looks benign) |
| C43. 5 | Malignant melanoma of skin of trunk (if you highly suspect melanoma) | ||
| R22. 2 | Localized swelling, mass and lump, trunk (if you’re unsure) | ||
| Patient with shortness of breath, wheezing, and a history of smoking. | Pulmonologist | R06. 02 | Shortness of breath |
| R06. 2 | Wheezing | ||
| Z87. 891 | Personal history of nicotine dependence | ||
| A child with inattention, hyperactivity, and difficulty in school. | Developmental Pediatrician / Psychiatrist | R41. 840 | Attention and concentration deficit |
| F90. 9 | Attention-deficit/hyperactivity disorder, unspecified type (if you feel confident in the diagnosis) | ||
| Patient with gradual, painless vision loss in the right eye. | Ophthalmologist | H54. 412 | Blindness, right eye, category 2 |
| Patient with sudden, severe headache (“worst of my life”). | Neurologist | R51 | Headache |
| G44. 1 | Vascular headache, not elsewhere classified (if migraine-like) | ||
| Patient with lower back pain radiating down the left leg. | Orthopedist / Neurosurgeon | M54. 16 | Radiculopathy, lumbar region |
| M54. 42 | Low back pain with sciatica, left side | ||
| A well-child check-up reveals a heart murmur. | Pediatric Cardiologist | R01. 1 | Cardiac murmur, unspecified |
| Patient with depression and anxiety not responding to initial treatment. | Psychiatrist | F32. A | Depression, unspecified |
| F41. 9 | Anxiety disorder, unspecified |
A Note for Readers: This table is for informational purposes and is not a substitute for professional medical coding advice. Always rely on your clinical judgment and the specific details documented in the patient’s chart.
The Role of “Medical Necessity” in Referrals
We’ve touched on this, but it’s worth diving deeper because it’s the linchpin of the entire referral process. “Medical necessity” is a term used by insurance companies (like Medicare, Medicaid, and private insurers) to determine if a health care service or product is reasonable and necessary for the diagnosis or treatment of an illness or injury.
The diagnosis code is the primary evidence you provide to prove medical necessity.
How Insurance Companies Use the ICD-10 Code
When a specialist’s office submits a claim for an initial consultation, they will include the diagnosis code from your referral. The insurance company’s computer system cross-references this code against their internal policies. The question the system asks is: “Is it standard and accepted medical practice for a [Type of Specialist] to see a patient with [Diagnosis Code]?”
For example, it is standard practice for a cardiologist to see a patient with I10 (Hypertension). Therefore, the visit is considered medically necessary.
It is not standard practice for a cardiologist to see a patient with L60. 0 (Ingrown nail). That claim would likely be denied.
If the Insurance Denies the Referral
What happens if your referral is denied for lack of medical necessity? It’s not necessarily the end of the road. Here’s what you can do:
-
Review the Denial Letter: It will state the specific reason for the denial. It might say “Diagnosis code does not support the requested service.”
-
Check Your Documentation: Was the code you used as specific as it could be? Did you include all relevant secondary codes (like symptoms or history) that might paint a fuller picture?
-
Gather More Information: Perhaps the denial triggers a need for more clinical data. You might need to send the results of an in-office test (like an EKG) that supports the need for the cardiology consult.
-
File an Appeal: You have the right to appeal the decision. This usually involves writing a letter of medical necessity, explaining in narrative form why the patient needs to see this specialist, based on their unique history and your clinical findings. You are essentially translating the ICD-10 codes back into plain English to tell the full story.
The Referral Process: A Step-by-Step Workflow
Understanding where the ICD-10 code fits into the bigger picture can help everyone in the office appreciate its importance. Here’s a typical workflow for a patient referral.
-
The Clinical Encounter: You see the patient, take a history, perform an exam, and make the decision to refer.
-
Documentation: You document your findings, your differential diagnosis, and your plan to refer in the patient’s medical record. This note is the source of truth for everything that follows.
-
Code Selection: Based on your documentation, you (or your coding staff) select the most accurate and specific ICD-10 code(s) that represent the reason for the referral. This is the most critical step.
-
Completing the Referral Form: You fill out the referral or prior authorization form. This form will include:
-
Patient demographics
-
Referring provider information
-
Specialist information
-
The ICD-10 code(s) you selected
-
Any relevant clinical information (like recent test results)
-
-
Prior Authorization (if required): The form is sent to the insurance company for approval. They review the diagnosis code and the requested service. If approved, they issue an authorization number.
-
Scheduling the Appointment: The specialist’s office receives the referral, often with the authorization number. They use the ICD-10 code to help schedule the patient appropriately (e.g., a patient with “chest pain” might be scheduled sooner than one with “skin tag”).
-
The Specialist Visit: The specialist sees the patient, reviews the history, and performs their own exam. Your ICD-10 code(s) guide their initial thought process.
-
Specialist’s Diagnosis and Billing: The specialist makes their own diagnosis and assigns their own, potentially more specific, ICD-10 code(s). They then bill the insurance company for the visit, linking their services to the diagnosis code that justifies them.
As you can see, the ICD-10 code is the common thread running through the entire process, from your initial exam all the way to the final payment.
Common Coding Mistakes to Avoid When Referring
Even experienced professionals can slip up. Here are some of the most common errors made during the referral coding process, and how to avoid them.
-
Mistake #1: Coding from a Superbill or Drop-Down Menu Without Thought. It’s easy to just pick a common code from a list. But that code might not be the most accurate for this specific patient. Always verify the code against your documentation.
-
How to Avoid: Use your documentation as your guide. Look up the code based on what you wrote, not the other way around.
-
-
Mistake #2: Using “Unspecified” Codes When More Information is Available. Using M54. 9 (Dorsalgia, unspecified) for a patient with clear, documented low back pain that gets worse when they sit (M54. 5 – Low back pain) is a missed opportunity for specificity. It makes the data less useful and can sometimes raise questions with payers.
-
How to Avoid: Ask yourself: “Do I know more than this code says?” If you know the location, the laterality, or the cause, look for a code that reflects it.
-
-
Mistake #3: Coding a Confirmed Diagnosis for a Rule-Out Scenario. As we discussed earlier, this is a major no-no. You cannot code for a condition that hasn’t been formally diagnosed.
-
How to Avoid: Remember the golden rule: code what you know, not what you suspect. Code the signs and symptoms.
-
-
Mistake #4: Not Linking the Correct Diagnosis to the Referral. In a patient with multiple chronic conditions, you might list several codes on a referral. However, you need to make it clear which code is the primary reason for this specific referral.
-
How to Avoid: On most referral forms, there is a field for “Primary Diagnosis” or “Reason for Referral.” Place the most relevant code there. The other codes are considered secondary or comorbid conditions.
-
-
Mistake #5: Forgetting to Update Codes for Chronic Conditions. If you are referring a patient for ongoing management of a chronic condition, make sure you are using the most current and accurate code for that condition, reflecting any changes in status or new complications.
-
How to Avoid: When a patient with a chronic condition returns for a follow-up, take a moment to review if their diagnosis code still accurately reflects their health status. Has their diabetic retinopathy progressed? Has their CKD stage changed? Use the updated code.
-
Frequently Asked Questions (FAQ)
Here are answers to some of the most common questions about ICD-10 codes and specialist referrals.
Q: Is there a specific ICD-10 code for “referral to specialist”?
A: No, there is not. ICD-10 codes are for diagnoses, symptoms, and reasons for encounter. They describe why the patient needs the specialist, not the act of referring itself.
Q: What is the best ICD-10 code to use if I don’t know what’s wrong with the patient yet?
A: In that situation, you should code the most specific sign or symptom you have identified. For example, if a patient has abdominal pain of unknown origin, use R10. 9 (Unspecified abdominal pain). This accurately reflects that the reason for the visit is a symptom in need of investigation.
Q: Can I use a Z-code for a specialist referral?
A: You can use a Z-code in addition to a symptom or diagnosis code, but it should almost never be the primary reason. For example, you might refer a patient with a strong family history of breast cancer (Z80. 3) for a genetic counseling and high-risk screening consult. The primary reason is the family history, so Z80. 3 would be appropriate. However, if the patient also has a lump, the lump code would be primary.
Q: What happens if I use the wrong ICD-10 code on a referral?
A: Several things can happen. The specialist’s office might call for clarification, delaying the appointment. The insurance company could deny the prior authorization, requiring you to resubmit with a correct code. In rare cases, if the code is fraudulent or grossly negligent, it could lead to compliance issues.
Q: How specific does my ICD-10 code need to be for a referral?
A: It needs to be as specific as your documentation allows. If your note says “left knee pain,” use the code for left knee pain (M25. 562), not the general code for knee pain. If your note says “suspected contact dermatitis due to poison ivy,” you would code the rash (L25. 9 – Unspecified contact dermatitis) and the external cause (poison ivy).
Q: Who is responsible for choosing the correct ICD-10 code on a referral?
A: Ultimately, the diagnosing or referring provider is responsible for the accuracy of the diagnosis code, as it is derived from their clinical judgment and documentation. However, in many practices, a medical coder or billing specialist will assign the code based on the provider’s notes.
Q: My patient needs to see a specialist, but they don’t have any symptoms right now. They just want a “check-up.” Is that a valid referral?
A: A “check-up” with a specialist is rarely considered medically necessary by insurance companies. There would need to be a specific risk factor or historical reason. For example, a patient with a personal history of colon polyps might be referred to a gastroenterologist for a surveillance colonoscopy. The code would be Z86. 010 (Personal history of colonic polyps). A referral to a cardiologist for a “heart check-up” in a patient with no symptoms and no risk factors would likely be denied.
Additional Resource
For the most up-to-date and authoritative information on ICD-10-CM coding, including official guidelines and coding updates, the best resource is the website of the Centers for Medicare & Medicaid Services (CMS) . You can also find valuable tools and references from the American Academy of Professional Coders (AAPC) .
-
CMS ICD-10 Website: [Insert link to official CMS ICD-10 page here – e.g., https://www.cms.gov/medicare/coding-billing/icd-10-codes]
-
AAPC Website: [Insert link to AAPC here – e.g., https://www.aapc.com/]
(Note: As a web writer, I cannot insert live links, but I can provide the suggested anchor text and destination.)
Conclusion
Navigating the world of medical referrals can feel like learning a new language. While there is no magic “icd 10 code for referral to specialist,” mastering the logic behind diagnosis coding transforms a daunting task into a straightforward process. The key takeaway is this: your ICD-10 code tells the story of why your patient needs specialized care.
By focusing on accurate, specific documentation and coding for confirmed diagnoses or, when appropriate, the presenting signs and symptoms, you provide a vital link in the chain of communication. This ensures the specialist understands the clinical picture, the insurance company recognizes the medical necessity, and most importantly, your patient receives timely and appropriate care. Remember, you are not just filling out a form; you are advocating for your patient’s health with every code you choose.
Disclaimer: This article is for informational purposes only and does not constitute medical, legal, or professional coding advice. Medical coding guidelines and insurance policies are subject to change. Always consult with a qualified professional and refer to official coding manuals and payer-specific guidelines for your particular situation.





