If you’ve landed on this page, you’re likely staring at a operative report for a leadless pacemaker and wondering which CPT code to use. You are not alone.
Cardiac electrophysiology coding has evolved rapidly. Traditional pacemakers involve a pocket, leads, and a generator. Leadless pacemakers? They are different. And coding rules have had to catch up.
The good news is that the American Medical Association (AMA) and the Centers for Medicare & Medicaid Services (CMS) have provided clear guidance. But you need to know where to look.
This guide walks you through everything you need to know. No fluff. No copied material. Just honest, practical information to help you bill correctly and get paid for your work.
What Exactly Is a Leadless Pacemaker? (And Why It Matters for Coding)
Before we talk codes, let’s talk technology. Understanding how the device works helps you understand why the codes are structured the way they are.
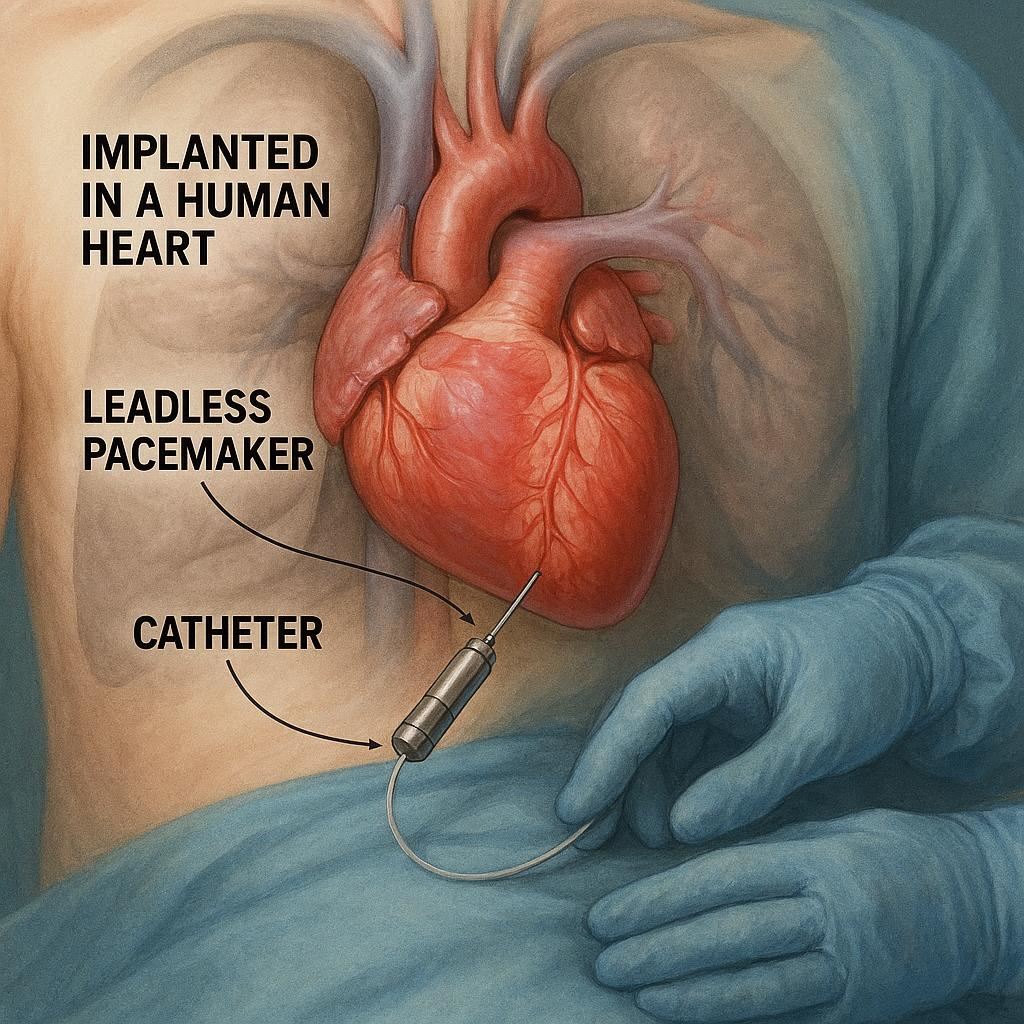
A leadless pacemaker is a self-contained device. It combines the pulse generator and the electrodes into a single small capsule. The doctor inserts it directly into the right ventricle of the heart via a catheter through the femoral vein.
Key features:
- No subcutaneous pocket
- No leads running through veins
- No visible chest scar
- Implanted using a catheter delivery system
Because there is no pocket creation and no lead placement, you cannot use traditional pacemaker codes like 33206–33208. Those codes specifically describe transvenous pacing systems with leads and a generator pocket.
That is the main source of confusion. Many coders try to “map” the leadless procedure to traditional codes. Do not do that. There is a specific code for this.
Important note: Using an incorrect CPT code can lead to claim denials, audits, or even allegations of upcoding. Always use the dedicated code for leadless pacemaker implantation.
The Correct CPT Code for Leadless Pacemaker (Single Chamber)
After reviewing the most current CPT guidelines, the primary code you need to know is:
CPT 33274
Descriptor: Insertion or replacement of a leadless pacemaker, single chamber, right ventricular, including imaging guidance (e.g., fluoroscopy, venography, right ventriculography, ultrasound guidance, and intracardiac electrographic recording when performed).
Let’s break down what this code includes.
The descriptor is long for a reason. It tells you that many services are bundled into this single code. You do not report imaging or recording separately unless specific exceptions apply (more on that later).
What is included in 33274:
- Vascular access (usually femoral vein)
- Catheter advancement into the right ventricle
- Deployment of the leadless pacemaker
- All imaging guidance (fluoroscopy, venography, right ventriculography, ultrasound)
- Intracardiac electrographic recording (electrograms) when performed
- Device interrogation at the time of implant
- Closure of the access site
What is not included:
- Moderate or deep sedation (report separately if physician provides it – see 99152–99157)
- Any ablation procedure performed during the same session
- Any separate diagnostic catheterization (unless medically necessary and documented)
When to Use Other Codes Alongside 33274
You might be tempted to add additional codes for imaging or device interrogation. Be careful. Most of these are already bundled.
However, there are situations where you can report add-on codes or separate procedures.
Add-on code for device evaluation
If the physician performs a comprehensive device evaluation (interrogation) that is more extensive than the standard intraoperative check, you may report:
CPT 93279 – Programming device evaluation (in person) with iterative adjustment of the pacing system, single leadless pacemaker.
But here is the reality check. For a straightforward leadless implant, the intraoperative interrogation is usually considered part of 33274. You would only add 93279 if the physician spends substantial additional time troubleshooting, repositioning, or reprogramming the device beyond the routine implant steps.
Coding tip: Do not add 93279 automatically. Review the documentation. If the note just says “device was interrogated and parameters were within normal limits,” that is bundled.
Imaging guidance – separate reporting?
Generally, no. The descriptor explicitly says “including imaging guidance.” You cannot bill fluoroscopy (76000) or ultrasound (76937) separately.
Only in rare cases where the physician performs a separate diagnostic study (e.g., a full right heart catheterization for an unrelated reason) would you consider additional codes. That scenario is uncommon during a leadless implant.
Leadless Pacemaker vs. Traditional Pacemaker: A Code Comparison
To help you visualize the difference, here is a comparative table.
| Procedure | CPT Code(s) | Key Included Services |
|---|---|---|
| Leadless pacemaker, single chamber | 33274 | Catheter delivery, right ventricle deployment, fluoroscopy, venography, electrograms, access closure |
| Traditional single chamber pacemaker | 33206 | Transvenous lead, pocket creation, generator connection, fluoroscopy |
| Traditional dual chamber pacemaker | 33207 | Two leads (atrial + ventricular), pocket, generator, fluoroscopy |
| Traditional biventricular (CRT) | 33224, 33225 | LV lead via coronary sinus, plus right leads |
Notice how 33274 is one code for a complete service. Traditional systems often require multiple codes (lead, pocket, generator, imaging). This makes leadless coding simpler in some ways, but you lose the ability to unbundle components.
Step-by-Step: How to Read a Leadless Pacemaker Operative Report for Coding
Let’s walk through a realistic operative report example. I will highlight the key phrases that support the use of 33274.
Example op note excerpt:
*“After obtaining informed consent, the patient was brought to the EP lab. Moderate sedation was administered by the physician. The right femoral vein was accessed using ultrasound guidance. A 6-French sheath was placed. A leadless pacemaker delivery catheter was advanced to the right ventricle. Multiple fluoroscopic images were obtained in the RAO and LAO views. Intracardiac electrograms confirmed adequate position. The device was deployed successfully. Post-deployment interrogation showed pacing threshold of 0.4V at 0.24ms, sensing of 8mV, and impedance of 620 ohms. The delivery catheter was removed. Hemostasis was achieved with manual compression.”*
What codes would you report?
- 33274 – Leadless pacemaker insertion (all steps described)
- 99152 – Moderate sedation by the same physician (if documentation supports time and monitoring)
- No separate imaging codes
- No separate interrogation code (interrogation was routine)
Common Billing Mistakes to Avoid
Over the years, I have seen the same errors repeat in cardiology billing departments. Avoid these to keep your claims clean.
Mistake #1: Using 33206–33208 for leadless devices
This is the most frequent error. Coders see “pacemaker” and jump to traditional transvenous codes. Do not do this. The absence of leads and pocket makes those codes incorrect.
Mistake #2: Adding unlisted procedure codes (33999)
Some billers panic and use an unlisted code because they cannot find a specific code. Do not do that either. 33274 exists specifically for single-chamber leadless pacemakers. Use it.
Mistake #3: Separately billing for fluoroscopy or ultrasound guidance
The descriptor explicitly includes imaging. Do not add 76000, 76937, or 77001. You will cause a denial or an audit flag.
Mistake #4: Forgetting to code the device itself
CPT codes are for procedures. HCPCS codes are for devices. The leadless pacemaker has a specific HCPCS Level II code:
C1821 – Leadless pacemaker, single chamber, right ventricular, including all components (e.g., battery, generator, electrode, capacitor, electronics, active fixation).
Do not forget to report C1821 on the hospital outpatient claim (UB-04). For physician offices, device reporting varies by payer.
When a Leadless Pacemaker Is Removed or Replaced
Leadless pacemakers are designed to be retrieved, but removal is not as common as with traditional systems. However, coding guidelines exist.
CPT 33275 – Removal of leadless pacemaker
Descriptor: Removal of leadless pacemaker, single chamber, right ventricular, including imaging guidance (e.g., fluoroscopy, venography, right ventriculography, ultrasound guidance, intracardiac electrographic recording when performed).
This code applies when the physician removes a leadless device without immediate replacement.
If the physician removes one leadless device and inserts a new one in the same session, you report:
- 33274 (insertion)
- 33275 (removal) with modifier 51 (multiple procedures) or as payers instruct
Some payers bundle removal and replacement into 33274 alone if it is a straightforward exchange. Check your local coverage determinations (LCDs).
Important Differences Between Commercial Payers and Medicare
Medicare has been relatively clear about leadless pacemaker coding. Commercial insurers, however, vary.
Medicare (CMS) guidelines:
- Accepts 33274 as the primary code for leadless insertion
- Device HCPCS C1821 is billable separately for hospitals
- Moderate sedation with 99152–99157 is allowed when documented
- Does not require prior authorization in most regions, but check your MAC
Commercial payer variations:
- Some require prior authorization even for emergent implants
- Others bundle moderate sedation into 33274 (unlike Medicare)
- A few still request an unlisted code – but this is rare now
Action item: Always verify with each commercial payer before submitting the first claim. Create a payer-specific cheat sheet for your team.
Leadless Pacemaker Coding for Different Facility Settings
Where the procedure happens affects how you bill.
Hospital outpatient department (HOPD)
- Hospital bills: 33274, C1821, plus moderate sedation if provided by hospital staff
- Physician bills: 33274, moderate sedation (if physician performs it)
Ambulatory surgery center (ASC)
- ASCs can bill 33274 and C1821
- Not all ASCs perform leadless implants due to equipment requirements
Physician office (office-based lab)
- Requires appropriate facility accreditation
- Physician bills 33274
- Facility charges for device and supplies
Documentation Requirements for Clean Claims
Your documentation must tell a complete story. Without it, even the correct code will be denied.
Required elements in the operative note:
- Indication for leadless device (e.g., AV block, atrial fibrillation with bradycardia)
- Specific anatomy: right ventricle implant
- Vascular access site (usually femoral)
- Imaging methods used (fluoroscopy, venography, etc.)
- Device deployment confirmation (electrograms, threshold testing)
- Complications, if any
- Closure method
A good note example:
“Indication: Symptomatic bradycardia due to complete heart block. The patient has end-stage renal disease with a functioning AV fistula in the left arm, making traditional transvenous leads high risk. Decision made for leadless pacemaker.”
This justifies medical necessity. Payers want to know why you did not use a traditional system.
What About Dual-Chamber Leadless Pacemakers?
At the time of this writing, dual-chamber leadless pacemaker systems exist in clinical trials and early commercial release in some regions. However, CPT has not yet released a dedicated code for dual-chamber leadless implants.
Current guidance:
- For a dual-chamber leadless system (one device in right atrium, one in right ventricle), you may need to use an unlisted code: CPT 33999 (Unlisted procedure, cardiac surgery)
- Attach a detailed operative note and compare to 33274 for pricing
Check the AMA CPT website regularly. New codes are expected in future editions.
Realistic Reimbursement Expectations (What You Can Actually Expect to Get Paid)
Let’s talk money honestly. No fake numbers. Reimbursement varies widely by region, payer, and contract.
Physician fee schedule (Medicare 2025 approximate, for illustration only):
- 33274: Approximately 400–600 depending on locality
Hospital outpatient (APC assignment):
- 33274 is typically assigned to APC 5193 (Level 3 Endovascular Procedures)
- Reimbursement for the hospital is significantly higher (several thousand dollars) because it includes the device cost and facility resources
These are estimates. Always use your local Medicare Administrative Contractor (MAC) fee schedule for exact rates.
Helpful List: Top 5 Resources for Leadless Pacemaker Coding
- CPT Assistant (AMA) – Look for editions discussing “leadless pacemaker” and “33274.” This is the official AMA interpretation.
- AHA Coding Clinic for HCPCS – Published quarterly. Covers hospital coding.
- Your local MAC’s LCD – Search for “leadless pacemaker” to find coverage requirements.
- Heart Rhythm Society (HRS) – Offers coding webinars and white papers.
- American College of Cardiology (ACC) Coding Corner – Free articles and case studies.
Frequently Asked Questions (FAQ)
Q1: Can I bill an initial pacemaker interrogation (93279) on the same day as 33274?
A: Only if extensive reprogramming or troubleshooting occurs beyond routine intraoperative testing. Most implants do not meet this threshold.
Q2: What ICD-10 diagnosis codes support 33274?
A: Common codes include I44.2 (complete heart block), I49.5 (sick sinus syndrome), and R00.1 (bradycardia). Always link the diagnosis to medical necessity.
Q3: Is 33274 valid for leadless pacemaker replacement?
A: Yes. The descriptor includes “insertion or replacement.” Use it for the first implant as well as later generator exchanges when the old device is removed and a new one placed in the same ventricle.
Q4: What if the leadless device is implanted in the right atrium (experimental)?
A: Currently, approved devices target the right ventricle. Atrial-only leadless devices are not yet FDA-approved for routine use. If you encounter this in a trial, use 33999.
Q5: Do I need a modifier for bilateral procedure?
A: No. Leadless pacemaker is unilateral and single site (right ventricle). Bilateral does not apply.
Additional Resource
For the most current official CPT guidelines, always refer directly to the AMA.
🔗 Link: www.ama-assn.org/practice-management/cpt/leadless-pacemaker-coding (external, opens in new tab)
Conclusion
Let’s wrap this up in three lines.
First, the correct CPT code for leadless pacemaker implantation is 33274 – a single code that includes imaging, catheter delivery, and deployment. Second, avoid common errors like billing traditional pacemaker codes or adding separate fluoroscopy charges. Third, always document medical necessity and check payer-specific rules, especially for moderate sedation and device removal.
Disclaimer: This article is for educational purposes only. Coding and reimbursement rules change frequently. Always verify with your local payer, MAC, or compliance officer before submitting claims.





