Navigating the world of durable medical equipment (DME) billing often feels like learning a foreign language. You might be a supplier trying to get a claim paid, a therapist writing a letter of medical necessity, or a wheelchair user seeking to understand your benefits. Whatever your role, you are likely here because you know that an anti-tipper is not just a piece of metal. It is a critical safety device that prevents a backward tip-over, which can lead to catastrophic injury.
Finding the correct code can be confusing. You type in “anti-tipper,” but the code description doesn’t always match that exact phrase. This exhaustive guide removes the guesswork. We will dive deep into the specific HCPCS codes, dissect the billing rules, and provide you with the clinical language needed to justify this equipment. This is not a superficial overview. We are going to examine the structure of the codes, the modifiers that unlock payment, and the strategic documentation that turns a denial into an approval.
Consider this your masterclass on coding for wheelchair safety accessories. We will leave no question unanswered.
Understanding HCPCS Level II: The Language of DME
Before we target a specific code, we need a solid foundation in HCPCS Level II. This is the coding system that powers the DME benefit under Medicare and many commercial insurers.
What is HCPCS Level II?
The Healthcare Common Procedure Coding System (HCPCS) is a standardized code set. Level I codes are the CPT codes you know for physician procedures. Level II codes, however, specifically identify products, supplies, and services not covered by CPT codes. This includes ambulance rides, prosthetics, and, crucially for us, durable medical equipment like wheelchairs and their accessories.
The Centers for Medicare & Medicaid Services (CMS) created this system to bring order to a chaotic billing landscape. Without it, every supplier would use a different name for an anti-tipper, and insurers would have no standard way to process claims.
The Anatomy of a HCPCS Code
A HCPCS Level II code is always one letter followed by four numbers. The letter defines the broad category. You will see codes starting with “E” for DME, “K” for temporary items assigned by the Pricing, Data Analysis, and Coding (PDAC) contractor, and “L” for orthotics and prosthetics.
When we discuss wheelchairs and their parts, we are firmly in the “E” series. Understanding this structure helps you instantly recognize that a code like E0971 belongs to the DME family. It signals to payers that this is a piece of hardware, not a service.
Why Accessories Have Their Own Codes
A standard wheelchair base code, like K0001 for a standard lightweight chair, includes a very specific package of components. It includes the frame, armrests, footrests, and wheels. It does not, however, include every possible safety option. CMS separates certain components into “accessories” coded with “E” numbers.
They do this because not every patient needs an anti-tipper. It would inflate the cost of the base chair for everyone if it were bundled in. By unbundling the code, CMS creates a system where you can bill for the anti-tipper separately, but only when it is medically necessary for that specific patient.
The Primary HCPCS Code for Anti-Tippers: E0971
You asked for the specific code, and here it is. When you search for “hcpcs code for anti tippers,” the direct match, as defined by the PDAC, is E0971. Let’s break down what this code truly represents.
Full Description and Scope of E0971
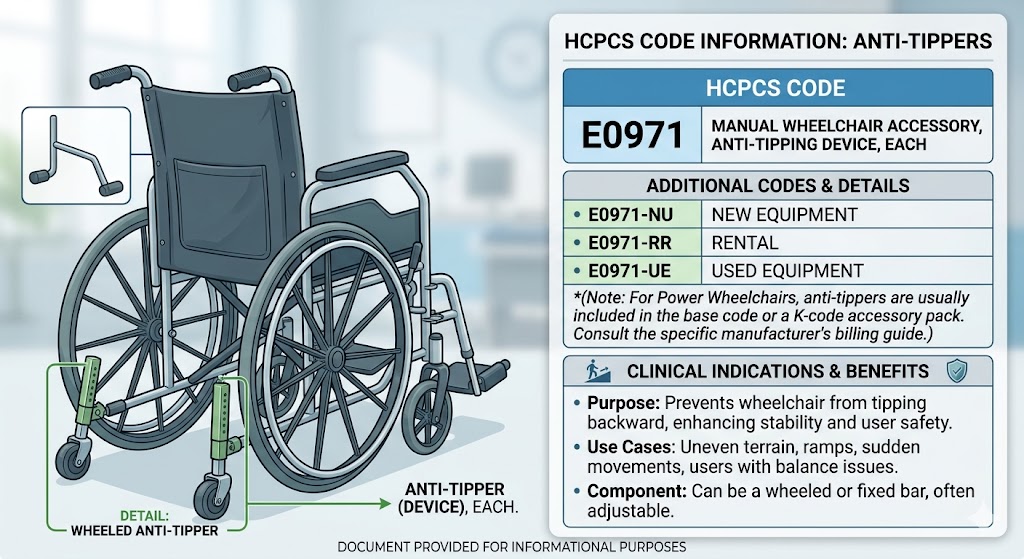
The official short description for E0971 is “Anti-tipping device, wheelchair.” It sounds simple, but in the world of DME billing, every word matters. This code specifically refers to an add-on accessory designed to limit the backward travel of a manual wheelchair’s center of gravity.
This device typically consists of a pair of small wheels or posts attached to a bar that extends rearward from the wheelchair frame, often near the camber tube or rear axles. When the chair begins to tip backward, these small wheels contact the ground, creating a physical stop that prevents a full tip-over.
The code E0971 applies to devices that are:
- Attached to a manual wheelchair base.
- Designed to prevent rearward instability.
- A separate add-on component, not integral to the chair’s original frame design.
Clinical Scenarios Requiring E0971
You cannot simply order an E0971 for every chair. The patient’s medical record must demonstrate a clinical need. When is an anti-tipper medically necessary?
- Amputation: A patient with a lower limb amputation has a center of gravity that shifts significantly backward. The missing weight of the leg makes the chair inherently prone to tipping backward. An anti-tipper is virtually standard care here.
- Neurological Conditions: Patients with conditions causing uncontrolled or extensor spasticity can suddenly throw their body backward. This force can easily lift the front casters and rotate the chair past its balance point. An anti-tipper provides a defined hard stop.
- New Wheelchair Users: Someone learning to perform a “wheelie” to navigate curbs needs a safety net. While training, the anti-tipper prevents a learning error from becoming an emergency room visit.
- Pediatric Users: Children may not have the cognitive awareness of danger or the trunk control to maintain a safe center of gravity. Their active, unpredictable movements often justify this code.
What E0971 Does Not Cover
It is just as important to know the limits of this code. E0971 specifically excludes certain related, but distinct, devices.
- Power Wheelchair Anti-Tippers: This code is strictly for manual wheelchairs. Adding an anti-tipper to a complex rehab power chair falls under a completely different coding pathway, which we will discuss shortly.
- One-Sided Devices: An anti-tipper is a bilateral assembly. A one-sided support or training wheel used for lateral stability is not E0971.
- Home-Made or Modified Devices: Billing E0971 requires the device to be a manufactured product that meets FDA standards, not a bolt-on part fabricated in a workshop. The item must be a distinct commercial product.
The Secondary Code: E0981 for Power Wheelchairs
The coding landscape splits sharply when you introduce power mobility. You cannot use E0971 on a claim for a power wheelchair base. CMS, through the PDAC, designates a separate code for safety devices on power platforms.
Decoding E0981: What It Actually Means
The code E0981 has a specific definition that may surprise you if you are only thinking of mechanical anti-tippers. The official code descriptor is “Wheelchair accessory, power solid seatback, replacement only.” However, many suppliers and clinicians have historically associated this code with the anti-tipping mechanism integrated into the seat or base of a power chair.
This requires clarity. The mechanical rear anti-tip wheels on a power base are frequently part of the base code itself or billed under a different accessory code, depending on the manufacturer. The “seatback” code sometimes enters the conversation because a power recline system shifts the user’s center of gravity and often includes integrated rear stability.
Let’s be precise. If you need a retrofittable anti-tip wheel assembly for a power chair that is not part of the base, check the PDAC Coding Verification Review for that specific product. The primary code E0981 is for the seatback, but discussing stability in power chairs inevitably brings you here because the seatback and base stability are integrated systems. For a standard mechanical anti-tip bar on a power chair, you will often look to the miscellaneous code, K0108, which we will cover as a critical safety valve for non-standard equipment.
Important Distinctions Between E0971 and E0981
Let’s draw a hard line between these codes in a comparative table. This visual distinction can prevent a billing error that leads to a certain denial.
| Feature | E0971 | E0981 / Power Base Accessories |
|---|---|---|
| Applicable Base | Manual Wheelchair (K0001-K0009) | Power Wheelchair (Group 1-4) |
| Primary Function | Prevent rearward tip-over of manual chair | Power solid seatback; stability often integrated into base |
| Physical Form | Horizontal bar with small rear wheels | Solid shell seat back; mechanical anti-tip is a separate wheel or strut |
| Billing Pathway | Manual wheelchair accessory | Power wheelchair accessory (often requires different justifications) |
| Key Modifier | NU (New Equipment) or RR (Rental) | NU, RR, or specific power mobility modifiers |
This table clarifies that the term “anti-tipper” is context-dependent. The base code of the wheelchair drives the entire coding logic. Never mix manual and power accessories on the same line of thinking without verifying the base code first.
Medical Justification: The Key to Unlocking Payment
A code is just a number until you provide the narrative. Insurers like Medicare do not deny anti-tippers because the code is wrong. They deny them because the medical justification is weak or missing. You must connect the patient’s physical condition to the function of the code.
The “In the Home” Functional Assessment
Medicare’s coverage standard for DME requires that the equipment be necessary for the patient to perform activities of daily living (ADLs) inside their home. This is a critical hurdle. A clinical note stating the patient “lives in a split-level home with two steps to enter” does not justify an anti-tipper. Medicare does not cover equipment solely for use outside the home or for negotiating stairs.
Your documentation must describe a scenario inside the home that creates a tipping risk. For example:
“Patient requires an anti-tipping device (E0971) to safely navigate the raised threshold between the living room and kitchen. Due to recent bilateral transtibial amputation, the patient’s center of gravity is posterior to the drive wheels. During propulsion, the front casters lift off the ground when crossing the 1.5-inch threshold, creating a high risk of posterior tip-over without the bilateral anti-tip bars engaging to arrest the motion.”
This statement covers the environment (inside the home), the physical deficit (amputation), and the functional limitation (caster lift during threshold crossing). It makes the anti-tipper a safety necessity, not a convenience.
Linking ICD-10 Codes to E0971
You must also provide a diagnosis code that supports the medical necessity. Certain ICD-10 codes are far more compelling than others for anti-tippers.
Strong Justification Diagnosis Codes:
- Z89.511: Acquired absence of right leg below the knee
- Z89.512: Acquired absence of left leg below the knee
- G80.1: Spastic diplegic cerebral palsy
- G35: Multiple sclerosis (with documented trunk instability)
- I69.351: Hemiplegia and hemiparesis following cerebral infarction affecting right dominant side
Weak Justification Diagnosis Codes:
- M54.5: Low back pain (Does not inherently shift the center of gravity)
- E11.9: Type 2 diabetes mellitus without complications (Not a direct functional mobility deficit)
- R26.2: Difficulty walking (Too vague; does not describe a seated stability deficit)
Therapists and physicians, your selection of the ICD-10 code tells the reviewer’s story for them. Choose the code that most accurately reflects the instability condition, not just the primary diagnosis.
Modifiers and Submission Strategy for Clean Claims
You have the right code and a solid medical record. Now you must format the claim correctly. An improperly modified claim will bounce back even with perfect justification.
The Critical Modifiers: NU vs. RR
E0971 is almost always a purchase item. Anti-tippers are installed and permanently live on the patient’s chair. The appropriate modifier is NU for “New Equipment.” This signals that you are billing for a purchase, not a rental.
The RR modifier (Rental) is rarely appropriate for E0971. However, you might use it if a patient rents a standard wheelchair short-term after a surgery and the anti-tipper is part of that rented package. Know your payer’s specific preference. Some state Medicaid programs prefer rental for all pediatric equipment due to growth needs.
The KX Modifier: Your Promise of Compliance
The KX modifier is your most powerful tool. By appending KX to the claim line, you are certifying, under penalty of law, that you have a fully compliant detailed written order and medical record on file that meets all coverage criteria. You do not send this documentation with the claim. You hold it ready for an audit.
Do not use KX lightly. An auditor from a RAC (Recovery Audit Contractor) or UPIC (Unified Program Integrity Contractor) can demand this file. If the records do not support the claim, the recoupment of funds plus interest can be devastating. Before you add KX, triple-check that the date of the order predates the delivery date, that the physician signed the order, and that the clinical notes directly state the need for a rear anti-tipper.
The GA Modifier: The Liability Shield
Sometimes, you know the patient meets the clinical need in your professional opinion, but you cannot find a Local Coverage Determination (LCD) that clearly supports it. Or, you suspect the insurer might deem it not medically necessary. In this case, you issue an Advanced Beneficiary Notice of Noncoverage (ABN) to the patient. You then append the GA modifier.
The GA modifier tells the payer, “I have a signed ABN on file. If you deny this claim, do not hold the patient financially responsible; the burden falls on the supplier or patient as agreed in the ABN.” This protects the patient from a surprise bill and allows you to pursue the claim while managing expectations. Never skip the ABN if you have a clinical doubt. A denied claim without a GA modifier often leaves the supplier holding a debt they cannot collect from the patient.
The HCPCS Code for Anti-Tippers in Complex Rehab
Pediatric and complex rehab technology (CRT) chairs introduce another layer of coding. A standard E0971 may not fit an ultra-lightweight rigid frame or a tilt-in-space manual chair. The device might be an integrated component from the manufacturer, specially designed for that chassis.
Integrated Design vs. Add-On Accessories
Major manufacturers like TiLite, Quickie, and Ki Mobility often design their anti-tippers as an integral part of the rear frame or axles, not a universal clamp-on bar. Technically, when you order this as an option from the manufacturer during the initial chair build, it can sometimes be invoiced as part of the chair’s single billing code under a “same or similar” pricing structure, or it requires the E0971 code if it’s listed separately on the PDAC list.
The safest path is a PDAC Verification. Go to the PDAC product classification list. Look up the exact manufacturer and model of the anti-tipper. The PDAC will tell you which HCPCS code CMS assigns to that specific stock-keeping unit (SKU). If the PDAC says it’s E0971, bill it as E0971, even if it bolts specifically to a Quickie frame. The code follows the product classification, not just the generic term.
K0108: The “Miscellaneous” Safety Net
What happens when you have a custom-fabricated anti-tipping solution? A severely involved pediatric patient might need a spring-loaded or dampened anti-tipper that doesn’t exist in a catalog. There is no specific HCPCS code for an articulated anti-tipper.
This is where K0108 enters. The descriptor is “Wheelchair component or accessory, not otherwise specified.” This is the DME equivalent of an unlisted code. A K0108 claim triggers a manual review. Every single time. The claim will not auto-adjudicate. You must submit a detailed product description, a manufacturer’s invoice showing your cost, and a powerful narrative explaining why a standard E0971 would fail this patient.
A successful K0108 narrative might read:
“Standard fixed anti-tip bars (E0971) are contraindicated for this patient due to severe extensor thrust spasticity. A rigid bar creates a sudden, jarring stop that triggers her seizure activity. We are providing a custom anti-tip system from [Supplier] featuring a progressive spring-resistance mechanism that gently decelerates the rearward tip, preventing both the fall and the myoclonic response. This technology is not classified under E0971, hence the K0108 submission.”
This level of detail is non-negotiable. Expect to defend a K0108 claim on appeal. Include video evidence of chair testing if your facility’s privacy policies allow it.
Detailed Look at Anti-Tipper Construction and Coding Impact
The physical build of an anti-tipper affects its clinical function, but does the material or design change the code? Generally, no. E0971 is E0971, whether the wheels are solid polyurethane or pneumatic. However, the construction matters for your justification.
Removable vs. Fixed Anti-Tippers
Most anti-tippers now feature a quick-release pin or a flip-back design. A user might remove them during transport or when learning advanced skills. A fixed, non-removable design (often seen on institutional chairs) may require less justification for “safety” but more justification for “accessibility.” If a fixed anti-tipper prevents the chair from fitting under a dining table, it creates a new functional barrier.
Your documentation should mention the type. “Bilateral removable anti-tip devices (E0971) were provided. These feature a flip-back mechanism to allow the patient to approach his workstation, a necessary activity for his employment, while providing posterior stability during propulsion.”
Desk-Length vs. Full-Length Arms
A standard anti-tipper extends far enough back to stop a full tip-over. Some manufacturers offer “desk-length” anti-tippers, which are shorter so they don’t hit the wall or a teacher’s desk when the student turns around. These shorter levers can still provide a safety stop but require a more aggressive angle of tip to engage.
Does a desk-length device require a different code? No, it still bills as E0971. But you must rationalize the deviation from standard. In a pediatric school setting, the note might say, “Desk-length anti-tippers (E0971) were chosen to allow tight-radius turning within the classroom layout while still arresting a posterior shift of the center of gravity during sit-to-stand transfers where the student often pushes backward into the chair.”
Anti-Tippers vs. Adaptive Stability Systems: Knowing the Difference
A common coding error is confusing an anti-tipper with a one-sided stabilizer. They serve different functions and, while they might both bill under the “miscellaneous” category for the latter, misunderstanding the distinction can lead to an audit failure.
The Purpose of an Anti-Tipper
An anti-tipper exists for a single reason: to prevent the wheelchair from flipping over backward. It is a safety device of last resort. It activates when the user has already lost control of their balance point. It is not designed for continuous ground contact.
The Function of Training Wheels or One-Sided Stabilizers
A one-sided stabilizer, often called a “fifth wheel” or “training wheel,” mounts to one side of the chair. It often maintains constant contact with the ground. Its purpose is to prevent a lateral tip-over, usually in sports chairs for users with hemiplegia or severe lateral trunk weakness. This device creates a wider footprint for lateral stability, not a stop for backward rotation.
A comparative analysis of these distinct accessories helps clarify their unique roles.
| Feature | Anti-Tipper (E0971) | Lateral Stabilizer (Unlisted/K0108) |
|---|---|---|
| Axis of Protection | Anterior-Posterior (Backward) | Medial-Lateral (Sideways) |
| Primary Patient | Amputees, extensor tone, learning wheelies | Hemiplegia, scoliosis with lateral lean, sports |
| Engagement | Only during a tip event | Often constant or during lateral weight shifts |
| Coding Pathway | E0971 (Specific Code) | K0108 (Miscellaneous, no specific code) |
| Mounting | Center or bilateral rear axle mounts | Unilateral side mount, often camber-tube mounted |
Miscoding a lateral stabilizer as E0971 is a red flag for auditors. The PDAC description is explicit. If the device prevents a sideways fall, it is not an anti-tipping device as defined by the E0971 code.
Navigating the Maze of Medicare LCDs and Policy Articles
No matter how well you understand the code, Medicare’s Local Coverage Determinations (LCDs) are the final authority. These documents, written by your regional DME Medicare Administrative Contractor (MAC), define the exact conditions under which they will pay for E0971.
Finding Your MAC’s Policy
Your first step is to identify your MAC. The two major DME MACs currently are Noridian and CGS Administrators. Go to their websites, locate the “Medical Policies” or “LCDs” section, and search for “Wheelchair Accessories” or directly for the E0971 code.
The LCD might state specific restrictions. For example, a policy might say, “An anti-tipping device (E0971) is covered when the patient’s condition is such that there is significant potential for the wheelchair to tip over backward during normal activities of daily living in the home.” That phrase “significant potential” is your target. Your records must explicitly state the potential.
The Dreaded “Convenience Item” Denial
The most common reason for denial of E0971 is the classification of the device as a “convenience item.” A reviewer might read a note that says “Anti-tippers provided for safety” and decide that all wheelchairs should be safe, and therefore the base chair should be safe enough, making the extra accessory just a convenience or a nice-to-have.
To defeat this, you must use the term “medically necessary safety device” but immediately follow it with the specific biomechanical reason. Don’t just say it’s for safety. Say:
“This is not a convenience item; it is a medically necessary safety accessory. Without the E0971, the patient’s significant posterior weight shift, measured at 2.5 inches posterior to the wheel hub center, will inevitably cause the chair to tip during the mandatory sit-to-stand pivot transfer from the wheelchair to the bed, a daily activity necessary for toileting and sleeping.”
This language transforms the anti-tipper from a generic safety feature into a prescribed biomechanical intervention.
The HCPCS Code for Anti-Tippers in Different Payers
Medicare’s rules serve as a template, but you cannot assume every commercial insurer follows them exactly. A Blue Cross Blue Shield plan or a state Medicaid agency can have stricter rules.
Commercial Insurance Nuances
A commercial plan might have a blanket exclusion for “accessories that do not directly treat a disease.” You might be fighting a definitional battle where they see the wheelchair as the treatment, and the anti-tipper as an optional part. In these cases, your insurance verification call is critical. Ask the provider relations representative: “Does the client’s specific plan document list any exclusions for wheelchair safety accessories under code E0971?” Get a reference number for the call.
If they say there is no exclusion, your prior authorization submission becomes a trial. The letter of medical necessity must be airtight, focusing on cost offset. A sentence like this can shift an internal reviewer’s perspective:
“Providing the E0971 anti-tip device (cost)isalow−costinterventiondesignedtopreventaposteriortip−overthatwould,withhighprobability,resultinatraumaticbraininjury,hipfracture,orcervicalstrain,conditionsrequiringemergencyservicescostingcost and significant rehabilitation expenses.”
Commercial payers respond to financial logic within a clinical framework. Show them the cost of not providing the code.
State Medicaid and EPSDT
For patients under 21, Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) mandate changes the game. If a pediatric patient needs an anti-tipper to correct or ameliorate a condition, a state Medicaid program must cover it, even if their standard adult DME policy would not. EPSDT often acts as a backstop when standard coverage criteria fail.
In a pediatric Medicaid appeal for E0971, reference the EPSDT mandate. State: “The requested anti-tipping device (E0971) is medically necessary to ameliorate the risk of posterior tip-over resulting from the patient’s spastic diplegic cerebral palsy, enabling safe independent mobility within the home. Coverage is required under the EPSDT benefit to ensure this child reaches his maximum functional potential.” This elevates the request from a simple DME claim to a statutory requirement.
Step-by-Step Guide: From Order to Claim Submission
Theory without process is just a philosophy. Here is a systematic workflow to move an anti-tipper from a clinical recommendation to a paid claim.
Step 1: The Specialty Evaluation
A licensed clinician (often a physical or occupational therapist) performs a mobility evaluation. They document the exact physical condition that causes a rearward instability. They do not just check a box for “anti-tipper.” They describe the tipping risk during specific functional tasks like reaching overhead, weight shifting, or propelling over a transition strip. This evaluation creates the clinical narrative.
Step 2: The Detailed Written Order (DWO)
The treating physician reviews the therapist’s evaluation and writes the order. The DWO must list the specific item: “E0971: Anti-tipping device, wheelchair.” Medicare requires the order to be dated within 45 days after the face-to-face encounter. The physician must sign and date it. A non-specific order that says “wheelchair and accessories” is invalid. It must list E0971 explicitly.
Step 3: The Product Verification
Before you deliver, log into the PDAC website. Download the DME Coding System (DMECS) file for E0971. Print the page showing that the specific model you are providing (e.g., “JAY Zip Anti-Tipper”) has a verified E0971 classification. Attach this to your internal file. This document is your shield against a “wrong code” audit accusation.
Step 4: The Home Assessment and Delivery
The ATP (Assistive Technology Professional) delivers the chair with the anti-tippers installed. They adjust the height so the small wheels are approximately 1.5 to 2 inches off the ground, allowing the chair to partially rotate over small obstacles without engaging, but engaging before the center of mass passes the rear axle. The ATP documents the setup. “Anti-tippers set at 1.5″ clearance. Patient demonstrated safe propulsion and transfer with devices engaged.”
Step 5: The Claim Assembly
You now build the electronic claim.
- Box 24D (CPT/HCPCS): E0971
- Modifier: NU (and KX, if criteria met; GA, if ABN signed)
- Diagnosis Pointer: Points to the ICD-10 code for amputation, spasticity, etc.
- Charge: Your usual and customary fee.
Press submit, and archive the comprehensive file with the DWO, clinical notes, PDAC verification, and delivery slip. The file is ready for the audit that may come in three years.
The Crucial Role of the Therapist’s Functional Narrative
A physician’s prescription often reads, “E0971, medically necessary.” That line, by itself, is a denial waiting to happen. A physical or occupational therapist must craft a detailed functional narrative to support the code. This narrative is the difference between a 5-minute review denial and a smooth approval.
Documenting Center of Gravity and Reach
A therapist can use standardized tests or observational analysis to document instability. The Functional Reach Test, modified for a seated position, provides an objective number. “Patient’s seated functional forward reach is limited to 4 inches; backward reach of 2 inches causes anterior caster lift. Center of gravity is significantly posterior due to a bilateral above-knee amputation.”
This data is gold. You are not asking the payer to trust a feeling. You are providing a measurement. “Seated functional reach: 4 inches. Caster lift occurs at 2 inches of backward displacement. E0971 required to create a safety boundary.” This translates the subjective instability into an objective deficit.
Creating a Training and Safety Plan
The narrative should also outline how the anti-tipper fits into a broader training plan, especially for new wheelchair users. This signals to the reviewer that the device is a therapeutic tool, not a permanent crutch in every case (though it often is permanent).
“The plan of care includes wheelchair skills training. The anti-tippers (E0971) will serve as a progressive safety tool. Initially, they will be in a fixed, down position for all propulsion. As the patient gains proficiency in weight shifting and trunk control, the therapist will adjust the anti-tippers to a flip-back position during supervised sessions to allow development of advanced skills, while remaining locked down for unsupervised home mobility.”
This demonstrates that the device is part of a professionally supervised treatment plan, dispelling the notion of a simple “gadget” dispensation.
Understanding the “Anti-Tipper” in a Tilting Wheelchair
A tilt-in-space manual wheelchair changes the mechanics of stability. When a patient reclines or tilts the entire seating system backward, the center of gravity shifts dramatically. Some tilt chairs have anti-tip bars built into the tilt mechanism. Some require an additional E0971 because the standard base still tips during transit, even if the seat is upright.
Does a Tilt Chair Need an Extra Code?
If the tilt chair’s manufacturer has integrated a stable extension into the rear frame that functions as an anti-tip device, billing a separate E0971 would be “unbundling,” which is illegal. The integrated device is part of the base code. However, many tilt-in-space chairs for adults still have a posterior footprint similar to a standard chair when the tilt is in the upright position. They can tip.
When do you need a separate E0971?
- The clinical note describes a tip risk specifically in the upright seating position.
- The manufacturer offers a clip-on anti-tipper as an optional accessory distinct from the tilt hardware.
- The PDAC product list for that manufacturer’s SKU explicitly lists a separate E0971 classification.
Always check the PDAC. If the tilt chair manufacturer bundled the anti-tip mechanism into the base code E1161 (for a manual tilt-in-space), billing E0971 on the same claim date is a clear overpayment.
Troubleshooting Denials and the Appeals Process
A denial for E0971 is not a dead end. It is an invitation to an appeal. Frame it that way. Each level of appeal is an opportunity to strengthen your argument and educate the reviewer.
Common Denial Reasons and Their Counters
Denial Reason: “The documentation does not support the medical necessity of this accessory.”
Counter: Resubmit with a redacted but specific excerpt from the therapy evaluation. Bold the section describing the physical finding causing the instability. Pair it with a peer-reviewed journal article (e.g., from Archives of Physical Medicine and Rehabilitation) discussing tip-over risks in that specific population, such as amputees.
Denial Reason: “E0971 is included in the allowance for the base wheelchair.”
Counter: This is a statutory error by the reviewer. You must cite the PDAC’s classification. Attach the DMECS printout showing E0971 is a distinct, separately billable code. Also, cite the CMS Program Integrity Manual, Chapter 5, regarding correct coding of separately payable items.
Denial Reason: “The anti-tipper is for the convenience of the caregiver/not needed in the home.”
Counter: This requires a very specific medical narrative. “The anti-tipper is not for caregiver convenience. The patient lives alone for 12 hours daily. She must perform all ADLs independently. A rearward tip during these unsupervised hours carries a high risk of injury with no one to assist. The device provides a necessary mechanical safety net to enable her independent home living.”
The Five Levels of Appeal
Know your path.
- Redetermination: Submit to the MAC within 120 days. This is a simple paper review.
- Reconsideration: Go to a Qualified Independent Contractor (QIC). This is a fresh pair of eyes.
- Administrative Law Judge (ALJ) Hearing: The amount must meet a threshold. This is a live hearing, often by phone. Present your clinical expert here.
- Medicare Appeals Council (Appeals Council): A review of the ALJ’s decision for legal errors.
- Federal District Court: The final step, rare for individual claims but part of the full due process.
Most E0971 denials win at the Reconsideration level if the documentation is solid. ALJs tend to be receptive to a clear clinical story of injury prevention, provided the “in the home” requirement is met.
The HCPCS Code for Anti-Tippers: A Global Perspective
While HCPCS governs the United States, the need for anti-tipper coding is universal. Looking briefly at how other systems handle it can illuminate our own process.
ISO Wheelchair Standards and Coding
The International Organization for Standardization (ISO) 9999 standard classifies assistive products. Under ISO 9999, wheelchairs and anti-tipping devices have numeric codes that differ from the HCPCS alpha-numeric system. The ISO system classifies it as a part of the wheelchair stability system rather than just a billing code. This approach—focusing on the function of the product rather than its billing allowance—reminds us that the HCPCS code is a payment mechanism, not a functional descriptor. A clinician should say “safety anti-tipper,” and the biller translates to E0971.
The Drive Toward Value-Based Care
The future of billing for items like E0971 will likely shift toward value-based models. Currently, it’s a fee-for-service code. In a future bundled payment, a provider might receive a single payment for a “mobility episode of care,” which includes the chair, accessories, and therapy. In that world, the E0971 code might vanish as a line item, consumed into the larger bundle. For now, however, it remains an indispensable distinct code for tracking the provision of this critical safety feature.
Product-Specific Coding: Popular Anti-Tipper Models and Their Codes
To make this practical, let’s look at specific products on the market. Remember, a manufacturer’s catalog name is not the code. Only the PDAC-assigned HCPCS is.
| Commercial Product Name | Manufacturer | PDAC-Assigned HCPCS | Key Feature |
|---|---|---|---|
| Flip-Back Anti-Tipper | Ki Mobility | E0971 | Lightweight, tool-free flip-back |
| User-Friendly Anti-Tip | Quickie (Sunrise) | E0971 | Receiver-mounted, adjustable height |
| Compact Anti-Tipper | TiLite (Permobil) | E0971 | Integrated design, hidden engagement |
| Zip Anti-Tipper | JAY (Sunrise) | E0971 | Quick-release, desk-length options available |
Always perform a fresh PDAC look-up before billing. Manufacturers frequently change model numbers and distribution rights, which can sometimes lead to a reclassification. A product verified as E0971 today might have a different verification on the date of delivery. Print the verification on the day you assemble the file.
Writing a Bulletproof Letter of Medical Necessity (LMN)
A structure for an LMN specifically targeting the E0971 code can save you hours.
Patient: [Name]
DOB: [Date]
Diagnosis: [ICD-10 Code and Description, e.g., Z89.511 Acquired absence of right leg below knee]
Requested Item: E0971 (Anti-tipping device, wheelchair)
Modifier: NU (New purchase)
Narrative:
“1. Patient Profile and Home Environment: Mr. Smith is a right transtibial amputee living alone in a single-level apartment. His home has a 1-inch threshold strip entering the bathroom. He is unable to ambulate functionally and relies on his manual wheelchair for all indoor ADLs.
- Physical Assessment: Due to the absence of the limb weight, the patient’s seated center of mass is shifted posteriorly relative to the drive wheel axle. During the seated assessment, a simple effort to lift his residual limb for a pressure relief resulted in immediate and uncontrollable front caster lift, requiring the assessing therapist to catch the chair.
- Medical Necessity: The anti-tipping device (E0971) provides a bilateral mechanical limit to this posterior rotation. Without it, the daily necessity of navigating the bathroom threshold and performing pressure-relief lifts carries a predictable and severe risk of falling backward, which could result in a head strike against the bathroom tile floor.
- Non-Device Alternatives: Altering his technique is not a viable solution due to the permanent absence of counter-balancing weight. A caregiver is not present in the home. The E0971 device is the only intervention that allows independent, safe mobility.
- Benefit vs. Risk: The risk of not providing this device is a traumatic head injury. The device is passive, requires no maintenance, and provides continuous safety protection.
Conclusion: The E0971 anti-tipping device is medically necessary for the patient to perform mobility-related ADLs safely within his home.”
This letter follows a logical chain: condition, deficit, task, risk, intervention. Each section builds on the last, leaving the reviewer with a single, obvious conclusion.
Common Billing Errors and How to Fix Them
Even the most experienced DME suppliers stumble. Here is a proactive guide to the common missteps.
Error 1: Billing the Code Without a Base Chair Code on the Same Day
If you bill E0971 on a standalone claim without the base wheelchair code (e.g., K0004), the claim may reject as a non-covered accessory. It needs a parent claim. Always bill the accessory on the same claim form as the base, or, if replacing the device later, use a claim line note explaining that the base chair was previously provided and paid.
Error 2: Using the Wrong Manufacturer’s Code
A supplier might bill the SKU for a manufacturer’s part number in the HCPCS field, such as putting “QK-ANTI1” in the box instead of E0971. The HCPCS field must contain E0971. The manufacturer part number goes in the narrative or a separate data field if the payer requests it.
Error 3: Assuming Group 2 Power Codes Apply
A biller might see “E0971” and attempt to bill it with a Group 3 power chair complex rehab code. The claim processor will flag a mismatch. Know your base wheelchair group and only pair accessories verified for that group. If the PDAC says an accessory is only for manual chairs, do not force it onto a power claim.
Error 4: The “Stat” Delivery
A therapist shouts, “He needs anti-tippers today or he’ll fall!” and you deliver without a physician’s order. You cannot bill. The order must predate delivery. In emergencies, get an immediate verbal order, document it, and have the physician sign within 30 days. But never deliver before a verbal or written order exists.
The Future of Anti-Tipper Technology and Coding Implications
DME codes, like E0971, change slowly. Technology does not. Looking ahead, we can anticipate how innovation might strain this coding framework.
Smart Anti-Tippers and Data Logging
Imagine an anti-tipper that contains an accelerometer and gyroscope. It counts how many times it engages. It connects via Bluetooth to a caregiver’s phone, alerting them that the user almost tipped over five times that day. This product is in development at several engineering universities.
How do you code it? It’s still primarily a safety device. It would likely bill as E0971, but its “smart” component would require a K0108 line for the sensor array. Or, CMS might issue a new code, perhaps an “A” series code for an emerging technology, which lasts for two years while they gather utilization data. Suppliers of future smart anti-tippers will need to pioneer these coding pathways.
3D Printed Patient-Specific Devices
With additive manufacturing, a clinic might scan a patient’s custom wheelchair and 3D print an anti-tipper that exactly matches the camber angle and ride height. This device would not come from a catalog. It would have no PDAC verification. It would represent a fundamental shift toward “Point-of-Care” DME manufacturing. The path for billing would fall entirely to K0108 with extensive supporting documentation, as discussed. This future state demands that DME billing manuals evolve to address digital fabrication.
Educational Resources for Continued Learning
Become the local expert. Commit to building a library of primary sources.
- PDAC DMECS: Bookmark the Durable Medical Equipment Coding System portal. Regularly verify the classification of the products you buy. The database is dmecs.medicarenhic.com.
- Noridian DME MAC Wheelchair LCD: The Noridian website houses the current Article (often A55426 and A52504) covering wheelchair accessories. Print the “Medical Necessity – Anti-Tippers” section.
- RESNA Position Papers: The Rehabilitation Engineering and Assistive Technology Society of North America publishes papers on seating and mobility standards. Their work on wheelchair stability provides the clinical backbone for your justification.
- CMS Internet-Only Manual (IOM), Publication 100-02, Chapter 15: This chapter details the statutory requirements for DME. Section 110 specifically addresses the wheelchair benefit.
Spending an hour a month reviewing these resources keeps your knowledge sharp and your claim success rate high.
Final Review: The HCPCS Code for Anti-Tippers at a Glance
Before we conclude, let us distill the essential data into a final, rapid-reference summary for your desktop.
| Query | Answer |
|---|---|
| Primary Code | E0971 |
| Code Descriptor | Anti-tipping device, wheelchair |
| Applies To | Manual wheelchairs |
| Power Chair Code | E0981 (Solid seatback); K0108 for mechanical anti-tip |
| Key Modifier | NU (New), KX (Compliance met), GA (ABN signed) |
| Replacement Code | E0971 with RA modifier (Replacement) |
| Rental Code | E0971 with RR modifier (Rare, but possible) |
| Strongest ICD-10 Link | Z89.5xx (Amputation), G80.1 (CP), G35 (MS) |
Print this table. Tape it to the billing department monitor. It answers 90% of questions in ten seconds.
Conclusion
Securing funding for a wheelchair anti-tipper requires mastery of the E0971 HCPCS code, a clear clinical justification linking the patient’s physical condition to a risk of rearward tip-over, and a meticulous understanding of modifiers like NU and KX. The process shifts from a simple billing task to a professional act of patient safety advocacy when you document the precise biomechanical deficits that make the device medically necessary in the home. By distinguishing between manual and power wheelchair codes, crafting powerful letters of medical necessity, and anticipating denial reasons with evidence-based counter-arguments, you transform a simple accessory into a funded, life-protecting intervention.
Frequently Asked Questions (FAQ)
1. Can I bill E0971 for an anti-tipper on a power wheelchair?
No. The E0971 code is strictly for manual wheelchairs. Anti-tipping devices for power wheelchairs fall under the power wheelchair accessory coding, often requiring a K0108 miscellaneous code or being included in the complex rehab base price, unless a specific PDAC assignment says otherwise. Using E0971 on a power chair claim will likely result in a denial.
2. What is the correct modifier for a new E0971 anti-tipper purchase?
The correct modifier is NU, which stands for “New Equipment.” This indicates that the anti-tipper is being purchased for the patient’s permanent use. If you are providing a replacement, you would use the RA modifier. Only use the RR (Rental) modifier in very specific, time-limited rental scenarios.
3. My claim for E0971 was denied as “not medically necessary.” What do I do?
Start by reviewing the clinical documentation. The denial usually means the clinical notes did not explicitly describe why the patient is at risk of tipping backward within their home. Resubmit a Redetermination with a detailed functional narrative from the therapist, linking the patient’s specific diagnosis (like amputation or spastic hemiplegia) to a specific home mobility task that creates a dangerous rearward instability.
4. Does a child’s stroller-style wheelchair need a different code for an anti-tipper?
Generally, no. If the base device is classified and coded as a manual wheelchair (such as an E1161 for a tilt-in-space), the anti-tipper still bills as an E0971. However, for adaptive strollers, which are coded under a different category, you must check the PDAC coding verification for that specific stroller model, as the anti-tipper might be bundled into the stroller’s base code.
5. Is an anti-tipper covered if the patient needs it only for outdoor use?
Under Medicare, coverage is generally limited to equipment needed to perform activities of daily living inside the home. If the documentation clearly states the anti-tipper is for negotiating outdoor curbs and ramps only, Medicare will likely deny it. The justification must convincingly demonstrate a need for the safety device to perform a task within the patient’s residence.
Additional Resource
For authoritative verification of HCPCS codes and product assignments, the Pricing, Data Analysis, and Coding (PDAC) contractor’s DME Coding System (DMECS) is the definitive source. You can directly search for specific product models and their assigned codes here:
PDAC DMECS Product Classification Search





