If you have ever sat in front of a billing screen wondering whether to type 93978 or 76770, you are not alone. Coding for an ultrasound of the aorta can feel surprisingly tricky.
The good news? It does not have to be a headache.
In this guide, we will walk through every major CPT code used for imaging the aorta. We will keep the language simple. We will skip the confusing medical jargon. And we will focus on real-world scenarios you face every day.
Whether you are a new medical coder, a sonographer, or a clinic manager, this article is for you.
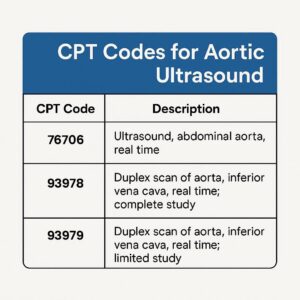
CPT Codes for Aortic Ultrasound US Aorta
Why Aorta Ultrasound Coding Gets Confusing
The aorta is a large blood vessel. But it sits right next to your abdominal organs. This creates a natural overlap.
Do you code for a vascular study? Or do you code for a complete abdominal exam?
The answer depends entirely on why the doctor ordered the test and what they looked at.
Payers like Medicare and private insurers look for specific documentation. If you pick the wrong code, the claim gets denied. Or worse, you trigger an audit.
Let us fix that confusion right now.
The Primary CPT Code for an Aorta Ultrasound
When most people ask for the cpt code for us aorta, they are usually looking for one of two codes: 93978 or 76770.
Here is the simple breakdown.
93978: Vascular Ultrasound of the Aorta
93978 is the code for a complete vascular study of the abdominal aorta. This includes real-time scanning with image documentation. The technologist also uses Doppler to check blood flow.
This code covers:
-
Imaging of the aorta from the diaphragm down to the iliac bifurcation.
-
Doppler waveform analysis.
-
Measurement of the aortic diameter.
Use 93978 when the order specifically asks for a vascular evaluation. Think: ruling out an aneurysm, checking for stenosis, or post-operative graft follow-up.
76770: Ultrasound, Abdominal, Real Time with Image Documentation; Complete
76770 is the code for a complete abdominal ultrasound. This includes the aorta, but it also covers the liver, gallbladder, pancreas, spleen, and kidneys.
Use 76770 when the doctor wants a full abdominal survey. The aorta is just one part of a larger picture.
Here is the golden rule:
-
Only aorta? Use 93978 (vascular).
-
Whole belly including aorta? Use 76770 (abdominal complete).
You cannot bill both for the same patient on the same day unless the doctor documents two separate and distinct exams. That almost never happens.
The Modifier Game: Limited or Follow-Up Studies
Not every aorta ultrasound takes 45 minutes. Sometimes you just need a quick look.
93979: Vascular Ultrasound of the Aorta (Limited)
93979 is the code for a limited vascular study of the aorta.
You use this code for:
-
Follow-up of a known small aneurysm (surveillance).
-
A quick re-check after an intervention.
-
A focused exam where you only look at one specific segment.
Documentation is critical here. The report must clearly state why a full study was not necessary. For example: “Limited study to reassess prior 3.2 cm infrarenal aneurysm. No change.”
76775: Ultrasound, Abdominal, Limited
76775 is the limited version of the abdominal ultrasound. You use this when the doctor only wants to look at one organ or a specific area. If they say “just check the aorta size,” you might lean toward 93979 instead.
Again, context matters.
| Scenario | Best CPT Code |
|---|---|
| New patient, rule out AAA, full vascular mapping | 93978 |
| Known AAA, 6-month follow-up, measure only | 93979 |
| Abdominal pain, check all organs including aorta | 76770 |
| Post-EVAR check of endograft | 93978 or 93979 (depends on scope) |
| Screening for AAA in a high-risk patient | G0389 (Medicare) or 76706 |
The Medicare Screening Exception: G0389 and 76706
We need to talk about screening.
Medicare offers a one-time screening ultrasound for abdominal aortic aneurysms (AAA). This is part of the “Welcome to Medicare” physical.
The code here is G0389 (sometimes crosswalked to 76706 in commercial payers).
This is a very specific code. You cannot use it for diagnostic purposes. You cannot use it for follow-up. It is only for the initial screening in a qualifying patient (men who smoked or family history).
If you use 93978 for a screening, Medicare will deny the claim. Always check the patient’s insurance and the reason for the visit first.
How to Choose Between Vascular and Abdominal Codes
This is the number one question I get from readers.
Let me give you a simple three-step checklist.
Step 1: Read the Order Carefully
Does the order say “Abdominal ultrasound” or “Aorta duplex”?
-
Abdominal ultrasound usually points to 76770 (complete) or 76775 (limited).
-
Aorta duplex or Aorta vascular study points to 93978 or 93979.
Step 2: Look at the Indication
The doctor writes the indication on the order form. This is gold.
-
“Abdominal pain, rule out cholelithiasis” → 76770 (even if they also measure the aorta).
-
“Known AAA, size check” → 93979.
-
“Pulsatile abdominal mass” → 93978.
-
“AAA screening” → G0389 or 76706.
Step 3: Check the Report for Key Phrases
If you are coding after the fact, search the report for these phrases:
Vascular language:
-
“Doppler waveforms obtained”
-
“Peak systolic velocity”
-
“Aneurysm diameter”
-
“Iliac arteries visualized”
Abdominal language:
-
“Liver is normal”
-
“Gallbladder without stones”
-
“Spleen size”
-
“Pancreas obscured by bowel gas”
You see the difference. One is about blood flow. The other is about solid organs.
Real-World Examples (Read These Carefully)
Let me walk you through five patient scenarios. This is where theory meets practice.
Example 1: The Screening
Patient: 66-year-old male, first Medicare visit. No symptoms. Family history of AAA.
Order: “AAA screening.”
What the tech does: Measures the infrarenal aorta. No Doppler. No other organs.
Correct code: G0389 (Medicare) or 76706 (commercial).
Why not 93978? Because this is a screening, not a diagnostic vascular study. Using 93978 here is incorrect.
Example 2: The Worried Patient
Patient: 58-year-old female. Complains of a “thumping feeling” in her belly. No known AAA.
Order: “Aorta duplex to rule out aneurysm.”
What the tech does: Images the entire abdominal aorta from diaphragm to bifurcation. Uses color Doppler. Measures diameter. Documents waveforms.
Correct code: 93978.
Why not 76770? The order specifically asked for a vascular study. The indication is vascular (aneurysm rule-out), not a general abdominal complaint.
Example 3: The Belly Pain
Patient: 45-year-old male. Right upper quadrant pain after fatty meals. Nausea.
Order: “Complete abdominal ultrasound.”
What the tech does: Images liver, gallbladder, pancreas, spleen, kidneys, and the aorta.
Correct code: 76770.
Why not 93978? The aorta was included, but it was not the focus. The exam was abdominal, not vascular. Billing 93978 here would be unbundling.
Example 4: The Follow-Up
Patient: 72-year-old male. Known 3.5 cm AAA. Last scan 6 months ago.
Order: “Limited aorta for aneurysm surveillance.”
What the tech does: Measures the same segment of the aorta. No full mapping. Limited documentation.
Correct code: 93979.
Why not 93978? The exam was limited. The documentation supports a limited study. A full vascular study would be overbilling.
Example 5: The Post-Op Check
Patient: 69-year-old female. Status post endovascular aneurysm repair (EVAR) one year ago.
Order: “EVAR surveillance: Complete aorta duplex with graft evaluation.”
What the tech does: Full aortic imaging. Duplex of the graft. Checks for endoleak. Measures aneurysm sac.
Correct code: 93978 (complete vascular study).
Why not 93979? Post-EVAR surveillance is typically a complete study. The graft requires full mapping. Limited studies are rare here unless specified.
Common Billing Mistakes (And How to Avoid Them)
Let me save you from the denials I see most often.
Mistake #1: Coding 93978 for Every Aorta Look
I get it. 93978 pays better. But if the report does not document a complete vascular study, you cannot use it.
Fix: Always match the code to the documentation. If the tech only measured the diameter and did not perform Doppler waveforms, use 93979.
Mistake #2: Adding 93978 to 76770
Some coders think, “Well, we did a full belly and a vascular study. Let’s bill both.”
Do not do this.
Payers consider the aorta part of the complete abdominal ultrasound. You cannot unbundle it unless the doctor documents a separate and distinct reason for the vascular study. That almost never happens on the same day.
Fix: Pick the primary code that matches the indication. If it is abdominal pain, use 76770. If it is a vascular concern, use 93978. Never both.
Mistake #3: Using G0389 for Diagnostic Work
G0389 is strictly for screening. If the patient has symptoms—pain, pulsatile mass, known aneurysm—you cannot use G0389.
Fix: Use 93978 or 93979 for symptomatic patients. Using a screening code for a diagnostic exam is fraud.
Mistake #4: Forgetting the Modifier for Multiple Procedures
Sometimes a patient needs a separate, unrelated ultrasound on the same day. For example, a carotid duplex (93880) and an aorta duplex (93978).
In this case, you append modifier -59 (Distinct Procedural Service) to the secondary code.
Fix: When in doubt, ask your billing manager. Unbundling rules are strict.
Documentation Requirements (What Your Report Must Include)
Your technologist’s report is the only thing that protects you in an audit.
For a complete vascular study of the aorta (93978), the report should include:
-
A statement of the indication (symptoms or reason).
-
The technique used (e.g., “Gray-scale and color Doppler imaging”).
-
Images of the aorta from the diaphragmatic hiatus to the iliac bifurcation.
-
Measurement of the maximum aortic diameter (anteroposterior and transverse).
-
Documentation of Doppler waveforms (if performed).
-
A comparison to prior studies (if available).
-
A clear impression or conclusion.
For a limited study (93979), the report must explain why a full study was not performed. For example:
*”Limited study performed for interval follow-up of known 3.2 cm infrarenal AAA. Only the known aneurysm segment was imaged per physician request.”*
If that sentence is missing, the code defaults to 93978. And if the documentation does not support 93978, you have a denial coming.
Private Payer vs. Medicare: What You Need to Know
Medicare follows the National Correct Coding Initiative (NCCI). Private payers usually follow similar rules, but not always.
Medicare:
-
Accepts 93978, 93979, 76770, 76775, and G0389.
-
Requires specific ICD-10 codes for medical necessity (see next section).
-
Does not allow 93978 and 76770 together on the same day.
UnitedHealthcare:
-
Follows similar rules but may require prior authorization for 93978.
-
Does not always recognize G0389. Use 76706 instead.
Blue Cross Blue Shield (varies by state):
-
Some plans consider 93978 a “specialty exam” requiring a higher copay.
-
Always verify local coverage determinations (LCDs).
Aetna:
-
Typically covers 93978 for AAA surveillance once every 12 months.
-
Requires documented growth or symptoms for more frequent studies.
Important note for readers: Never assume coverage. Always check the patient’s specific plan. A single prior authorization denial can cost your practice hundreds of dollars.
ICD-10 Codes That Support Medical Necessity
A CPT code without a diagnosis code is like a car without gas. It goes nowhere.
Here are the most common ICD-10 codes used with aorta ultrasound CPT codes.
For 93978 (Complete Vascular Study)
-
I71.4 – Abdominal aortic aneurysm, without rupture
-
I71.3 – Abdominal aortic aneurysm, ruptured (emergency)
-
I71.6 – Thoracoabdominal aortic aneurysm
-
I77.72 – Dissection of abdominal aorta
-
R10.9 – Unspecified abdominal pain (use cautiously)
-
R09.89 – Pulsatile abdominal mass
For 93979 (Limited Vascular Study)
-
Z09 – Follow-up exam after treatment (for surveillance)
-
I71.4 (if known AAA)
-
Z86.79 – Personal history of AAA repair
For 76770 (Complete Abdominal)
-
R10.0 – Acute abdomen
-
R10.9 – Abdominal pain
-
K80.00 – Gallstone with acute cholecystitis
-
R16.1 – Splenomegaly
For G0389 / 76706 (Screening)
-
Z13.6 – Encounter for screening for cardiovascular disorders
-
Z00.00 – Encounter for general adult medical exam (Medicare wellness)
Warning: Payers will deny 93978 for a screening diagnosis. And they will deny G0389 for a symptomatic diagnosis. Match the code to the reason.
A Quick Reference Table for Daily Use
Print this table. Tape it to your monitor. Use it every day.
| If the order says… | And the indication is… | Use this CPT code |
|---|---|---|
| “Aorta duplex” | Rule out AAA, known AAA, post-EVAR | 93978 |
| “Limited aorta” | Surveillance, quick re-check | 93979 |
| “Abdominal ultrasound” | Pain, nausea, mass, organ check | 76770 |
| “Limited abdomen” | Single organ or focused area | 76775 |
| “AAA screening” | No symptoms, Medicare wellness | G0389 or 76706 |
How to Appeal a Denial for an Aorta Ultrasound Code
Denials happen. Even to great coders.
If your claim for 93978 gets denied, here is a simple appeal process.
Step 1: Read the Denial Code
Look at the Explanation of Benefits (EOB). Common denial codes for aorta ultrasounds include:
-
CO-50 (Not medically necessary)
-
CO-97 (Benefit for this service not included)
-
PR-2 (Customary fee/reduction)
Step 2: Check Your Documentation
Go back to the report. Does it clearly support medical necessity? Does it mention symptoms or a known diagnosis?
If the report says “Screening” or “Routine,” you will lose the appeal.
Step 3: Write a Simple Appeal Letter
Keep it short. Include:
-
Patient name and ID number.
-
Date of service.
-
CPT code (93978).
-
A clear statement of medical necessity.
-
Attach the relevant portion of the report.
Example sentence:
“The 93978 was medically necessary because the patient presented with a pulsatile abdominal mass (R09.89), and the duplex study was required to rule out an abdominal aortic aneurysm.”
Step 4: Submit and Wait
Send the appeal to the address on the EOB. Follow up in 30 days if you do not hear back.
Most appeals for 93978 succeed when the documentation supports the code.
Frequently Asked Questions (FAQ)
1. Can I use 93978 for a bedside aorta ultrasound in the ER?
Generally, no. Bedside ultrasounds are often limited and performed by emergency physicians, not vascular techs. Many payers expect a lower-level code like 93979 or even an unlisted code (76999) if documentation is sparse. Check your hospital’s policy.
2. What is the difference between 93978 and 76770 in plain English?
93978 looks at blood flow in the aorta specifically. 76770 looks at all the organs in the belly, including the aorta. Think of 93978 as a “plumbing exam” and 76770 as a “house inspection.”
3. Does Medicare cover 93978 for AAA screening?
No. Medicare covers G0389 for screening. Medicare covers 93978 only for diagnostic purposes (symptoms or known disease).
4. How often can I bill 93979 for aneurysm surveillance?
Most payers allow once every 12 months for a stable, small AAA (3.0–4.0 cm). For larger aneurysms or rapid growth, more frequent studies may be covered. Always check the payer’s medical policy.
5. What if the doctor only wants the aorta measured and no Doppler?
You cannot use 93978 because Doppler is part of a complete vascular study. Use 93979 (limited vascular) or 76775 (limited abdominal) depending on the order. Many coders default to 93979 in this case.
6. Is there a specific CPT code for a thoracic aorta ultrasound?
Yes. For the thoracic aorta, use 93880 (duplex scan of the aorta, arch, and supraarch vessels) or 93350 (echocardiography for the ascending aorta). Thoracic aorta coding is a different world. That is a topic for another guide.
7. Can I bill both a vascular study and an abdominal ultrasound on the same day?
Only if the doctor documents two separate and distinct exams for different reasons. Example: A patient with abdominal pain (76770) who also has a known AAA requiring separate vascular mapping (93978). This is rare. Append modifier -59 to the secondary code.
Additional Resources for Aorta Ultrasound Coding
No single article can cover every edge case. Coding rules change. Payer policies shift.
For the most current information, bookmark these trusted resources:
-
CMS Local Coverage Determinations (LCDs): Search your state’s Medicare contractor for “Aorta Duplex” or “93978.”
-
American College of Radiology (ACR) Appropriateness Criteria: Free guidelines on when an aorta ultrasound is appropriate.
-
American Medical Association (AMA) CPT Manual: The official source. Buy the current year.
-
AAPC Forums (Medical Coding subreddit and official AAPC site): Real-world advice from working coders.
👉 Recommended link: CMS.gov – Ultrasound of the Abdominal Aorta Coverage (Search for “Aorta Duplex NCD” for national coverage policy)
A Final Note on Honest Coding
I want to leave you with something important.
CPT codes are not just billing tools. They tell the story of the patient’s care. When you code 93978, you are telling the insurance company: “We performed a complete, medically necessary vascular study of the aorta.”
When you code 93979, you are saying: “We did a focused, limited exam for a specific reason.”
And when you code 76770, you are saying: “We looked at the whole abdomen, and the aorta was part of that picture.”
Do not inflate codes. Do not bill for work you did not do. And never, ever change a code just to get paid.
Honest coding protects your patients. It protects your practice. And it protects your reputation.
Conclusion
Choosing the right CPT code for an aorta ultrasound depends entirely on the exam’s purpose: vascular studies use 93978 (complete) or 93979 (limited), while abdominal exams use 76770 (complete) or 76775 (limited). Screening codes like G0389 or 76706 are reserved for asymptomatic Medicare patients. Always match your code to the documentation, and you will avoid denials and audits.
Disclaimer: The information provided in this article is for educational and informational purposes only. CPT codes, regulations, and payer policies change frequently. Always verify coding requirements with your local medical billing specialist or the current CPT manual.
Author: Senior Medical Billing Writer
Date: APRIL 11, 2026





