In the intricate world of medical coding, few areas demand as much precision and clinical understanding as coding for pulmonary hypertension (PH). It is a complex, progressive, and often misunderstood condition that bridges the specialties of cardiology and pulmonology. For the medical coder, PH represents a significant challenge—a challenge where a single digit in a code can dramatically alter the clinical picture, impact the severity of illness, and ultimately, determine the legitimacy of a claim for reimbursement. This is not merely an academic exercise; it is a critical function that supports patient care, fuels clinical research through accurate data, and ensures the financial viability of healthcare providers.
This comprehensive guide is designed to be your definitive resource. We will move beyond a simple listing of codes and delve into the pathophysiology of PH, the logic behind the World Health Organization (WHO) classification system, and the nuanced application of ICD-10-CM guidelines. We will dissect each code within the I27 block, providing clear, actionable guidance on its proper use, supported by real-world case studies. Our goal is to transform your approach from one of uncertainty to one of confident mastery, empowering you to navigate the complexities of PH coding with accuracy and expertise. Whether you are a seasoned coder, a healthcare administrator, or a clinical professional seeking to understand the billing implications of your work, this article will provide the depth and detail you require.
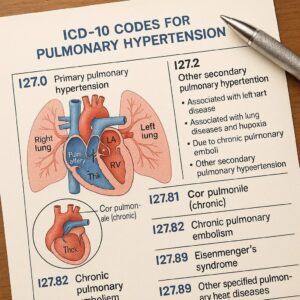
icd-10-codes for pulmonary hypertension
2. Understanding Pulmonary Hypertension: A Primer for Coders
To code a condition correctly, one must first understand it. Pulmonary hypertension is not a single disease but a hemodynamic and pathophysiological condition defined by an abnormal increase in pressure within the blood vessels of the lungs.
The Physiology of the Pulmonary Circuit
The human circulatory system is composed of two main circuits: the systemic circuit (heart to body and back) and the pulmonary circuit (heart to lungs and back). The right side of the heart pumps deoxygenated blood through the pulmonary arteries into the vast, low-pressure, high-compliance network of the lungs. Here, carbon dioxide is released, and oxygen is picked up. The now-oxygenated blood returns to the left side of the heart via the pulmonary veins, ready to be pumped out to the body. The normal mean pulmonary artery pressure (mPAP) is about 8-20 mmHg at rest.
The Clinical Definition: What is Pulmonary Hypertension?
Pulmonary hypertension is formally defined by a mean pulmonary artery pressure (mPAP) of >20 mmHg at rest, as measured by the gold-standard test, right heart catheterization. This elevated pressure puts a strain on the right ventricle of the heart, which is not designed to pump against high resistance. Over time, this leads to right ventricular hypertrophy (thickening of the heart muscle) and eventual right-sided heart failure, a condition known as cor pulmonale.
Symptoms are often non-specific and insidious, including shortness of breath (dyspnea) on exertion, fatigue, chest pain, dizziness, and fainting (syncope). This non-specific presentation often leads to delays in diagnosis, sometimes for years.
3. The World Health Organization (WHO) Groups: The Bedrock of PH Coding
The clinical classification of PH is the cornerstone of accurate coding. The WHO has organized PH into five broad groups based on shared pathological and hemodynamic characteristics and similar treatment approaches. This classification is updated periodically at world symposia and is directly reflected in the structure of the ICD-10-CM code set.
Group 1: Pulmonary Arterial Hypertension (PAH)
This group comprises conditions that directly affect the small pulmonary arterioles, causing them to constrict, thicken, and become blocked. It is characterized by pre-capillary PH.
-
Idiopathic PAH (IPAH): PAH with no known cause.
-
Heritable PAH: Caused by genetic mutations (e.g., BMPR2).
-
Drug- and Toxin-Induced: Associated with certain appetite suppressants or illicit drugs.
-
Associated with Other Conditions: This is a key sub-category for coders, including PAH associated with:
-
Connective tissue diseases (e.g., scleroderma, lupus)
-
HIV infection
-
Portal hypertension (Portopulmonary hypertension)
-
Congenital heart disease
-
Group 2: PH Due to Left Heart Disease
This is the most common form of PH. It results from elevated pressures in the left side of the heart, which are transmitted backward through the pulmonary veins into the pulmonary arteries (post-capillary PH). Common causes include:
-
Left ventricular systolic or diastolic dysfunction (Heart Failure)
-
Valvular heart disease (e.g., mitral stenosis, mitral regurgitation)
Group 3: PH Due to Lung Diseases and/or Hypoxia
This group is caused by chronic lung diseases that lead to destruction of the lung tissue (and thus the vascular bed) or chronic hypoxia (low oxygen levels), which causes pulmonary vasoconstriction.
-
Chronic Obstructive Pulmonary Disease (COPD)
-
Interstitial Lung Disease (ILD)
-
Sleep-disordered breathing (e.g., Obstructive Sleep Apnea)
-
Chronic high-altitude exposure
Group 4: PH Due to Pulmonary Artery Obstructions
This group is primarily comprised of Chronic Thromboembolic Pulmonary Hypertension (CTEPH). It is caused by organized blood clots that obstruct the pulmonary arteries, leading to increased pressure. It is a potential long-term complication of acute pulmonary embolism.
Group 5: PH with Unclear or Multifactorial Mechanisms
This is a heterogeneous group of conditions where the mechanisms of PH are unclear, complex, or multifactorial.
-
Hematologic disorders (e.g., chronic hemolytic anemia)
-
Systemic disorders (e.g., sarcoidosis, vasculitis)
-
Metabolic disorders
-
Other (e.g., chronic renal failure, tumor obstruction)
4. Navigating the ICD-10-CM Code Block: I27
The codes for pulmonary hypertension are located in Chapter 9 of ICD-10-CM, “Diseases of the Circulatory System,” under the code block I27 – Other pulmonary heart diseases.
A Deep Dive into the Official Guidelines
The ICD-10-CM Official Guidelines for Coding and Reporting provide critical instruction. For I27, there is a crucial note:
“Code also the underlying disease or sequelae of the underlying condition, if known and applicable.”
This “code also” instruction is not a sequencing rule; it means you must report both the PH code and the code for the underlying cause. The sequencing will depend on the circumstances of the encounter.
The Hierarchy of Codes: A Roadmap for Coders
The structure of the I27 codes is hierarchical, moving from less specific to more specific. The following table provides a clear overview of this structure and its alignment with the WHO groups.
ICD-10-CM Codes for Pulmonary Hypertension Mapped to WHO Groups
| ICD-10-CM Code | Code Description | Corresponding WHO Group(s) | Clinical Context & Notes |
|---|---|---|---|
| I27.0 | Primary pulmonary hypertension | Group 1 (Idiopathic PAH) | An older term largely synonymous with Idiopathic PAH. Use only if documented as such. |
| I27.1 | Kyphoscoliotic heart disease | Group 3 / 5 | PH caused by severe curvature of the spine, which restricts lung function. Rare. |
| I27.20 | Pulmonary hypertension, unspecified | N/A | A nonspecific code to be used only when the medical record lacks detail on the type or cause. |
| I27.21 | Secondary pulmonary arterial hypertension | Group 1 (Associated PAH) | Used for WHO Group 1 PAH that is associated with another condition (e.g., connective tissue disease, HIV). |
| I27.22 | Pulmonary hypertension due to left heart disease | Group 2 | The most commonly used code for the most common cause of PH. |
| I27.23 | Pulmonary hypertension due to lung diseases and hypoxia | Group 3 | Used when PH is a complication of chronic lung disease or chronic hypoxia. |
| I27.24 | Chronic thromboembolic pulmonary hypertension | Group 4 | Used specifically for CTEPH. |
| I27.29 | Other secondary pulmonary hypertension | Group 5 | A catch-all for secondary PH that doesn’t fit I27.21-I27.24 (e.g., due to sarcoidosis, hematologic disorders). |
| I27.81 | Cor pulmonale (chronic) | A complication, not a cause | Use as an additional code when right heart failure is documented as a direct result of PH. |
| I27.89 | Other specified pulmonary heart diseases | N/A | For other rare pulmonary heart diseases not elsewhere classified. |
| I27.9 | Pulmonary heart disease, unspecified | N/A | A nonspecific code for when documentation is limited to “pulmonary heart disease.” |
5. Code-Specific Analysis and Documentation Requirements
I27.0 – Primary pulmonary hypertension
This code is a legacy term. In modern clinical practice, this is referred to as Idiopathic Pulmonary Arterial Hypertension (IPAH). Coders should use I27.0 only if the physician specifically documents “primary pulmonary hypertension.” If “idiopathic PAH” is documented, I27.0 is still the correct code, as there is no specific code for “idiopathic” in the I27.2- series. There is no underlying cause to code with I27.0.
I27.1 – Kyphoscoliotic heart disease
This is a very specific code for PH resulting from a severe structural deformity of the spine (kyphoscoliosis), which impairs lung expansion and leads to chronic hypoxia. The documentation must clearly link the PH to the spinal deformity.
I27.2 – Other secondary pulmonary hypertension (The Workhorse Code)
This is the most important category for coders, as it contains the specific etiologies.
-
I27.20 – Pulmonary hypertension, unspecified: This is a low-specificity code that should be a last resort. It triggers audits and may lead to denied claims if more specific information is available in the record. It is acceptable only during an initial workup before a cause is determined.
-
I27.21 – Secondary pulmonary arterial hypertension: Documentation is key. The physician must document PAH in the context of an associated condition like scleroderma, HIV, or portal hypertension. The coder must then code also the underlying condition (e.g., M34.0 Progressive systemic sclerosis, B20 Human immunodeficiency virus [HIV] disease, K76.6 Portal hypertension).
-
I27.22 – Pulmonary hypertension due to left heart disease: This code requires documentation explicitly linking the PH to left heart disease, such as “PH secondary to diastolic heart failure” or “PH due to severe mitral valve stenosis.” Code also the specific heart condition (e.g., I50.31 Acute diastolic (congestive) heart failure, I05.0 Mitral stenosis).
-
I27.23 – Pulmonary hypertension due to lung diseases and hypoxia: The documentation must state the PH is due to or associated with a chronic lung condition or hypoxia. Examples: “PH secondary to advanced COPD” or “PH in the setting of idiopathic pulmonary fibrosis.” Code also the lung disease (e.g., J44.9 Chronic obstructive pulmonary disease, unspecified, J84.112 Idiopathic pulmonary fibrosis).
-
I27.24 – Chronic thromboembolic pulmonary hypertension: This code is reserved for confirmed CTEPH. It should not be used for acute pulmonary embolism (I26.-). Documentation often includes findings from V/Q scans and pulmonary angiograms. Code also the personal history of pulmonary embolism (I82.92-).
-
I27.29 – Other secondary pulmonary hypertension: This is the code for WHO Group 5. Use this when the cause is documented as a multifactorial or rare disorder not covered by I27.21-I27.24, such as sarcoidosis, vasculitis, or chronic hemolytic anemia. Code also the underlying condition (e.g., D86.0 Sarcoidosis of lung, D58.9 Hereditary hemolytic anemia, unspecified).
I27.81 – Cor pulmonale (Chronic)
Cor pulmonale is right heart failure resulting from PH due to lung disease. It is a manifestation of the underlying pulmonary condition. The instructional note under I27.81 states: “Code first the underlying pulmonary disease.” This is a critical sequencing rule.
-
Example: A patient with COPD and cor pulmonale.
-
Code 1: J44.9 Chronic obstructive pulmonary disease, unspecified
-
Code 2: I27.81 Cor pulmonale (chronic)
-
6. The Art of Sequencing: Primary Diagnosis, Comorbidities, and Manifestations
Sequencing—deciding which code to list first—is driven by the reason for the encounter, as per the Uniform Hospital Discharge Data Set (UHDDS) guidelines.
-
Inpatient Encounter for PH Management: If a patient is admitted primarily for management of their WHO Group 1 PAH (e.g., titration of vasodilator therapy), the PH code (I27.21) would be the principal diagnosis. The associated condition (e.g., M34.0 Systemic sclerosis) would be listed as a secondary diagnosis.
-
Inpatient Encounter for Underlying Condition: If a patient is admitted for an exacerbation of their COPD, and the PH is a chronic, stable comorbidity, then the COPD (J44.1) is the principal diagnosis, and the PH (I27.23) is secondary.
-
The “Code Also” Instruction: This reminds you that both codes are necessary for a complete picture, but sequencing depends on the circumstance.
7. Clinical Documentation Improvement (CDI): A Partnership for Accuracy
Coders are reliant on clear, specific physician documentation. A CDI program fosters a collaborative relationship.
Essential Questions for Physician Queries:
-
If the note only states “pulmonary hypertension,” a query might ask: “Can the type of pulmonary hypertension be specified (e.g., WHO Group) or the underlying cause clarified?”
-
If the note states “PAH” and “scleroderma” but doesn’t link them, a query might ask: “Is the pulmonary arterial hypertension associated with the scleroderma?”
-
If “cor pulmonale” is documented, a query might confirm: “Can the underlying chronic pulmonary condition causing the cor pulmonale be specified?”
Documenting Specificity: From “PH” to a Billable Code
-
Unacceptable: “Pulmonary hypertension.” -> Leads to I27.20.
-
Acceptable: “Pulmonary hypertension, likely due to underlying COPD.” -> Leads to I27.23 and J44.9.
-
Ideal: “Secondary pulmonary arterial hypertension associated with systemic sclerosis.” -> Leads to I27.21 and M34.0.
8. Case Studies: Applying Knowledge to Real-World Scenarios
Case Study 1: Newly Diagnosed Idiopathic PAH
-
Scenario: A 45-year-old female is admitted to the cardiology service for right heart catheterization and initiation of therapy. The final diagnosis is Idiopathic Pulmonary Arterial Hypertension.
-
Documentation: “Idiopathic Pulmonary Arterial Hypertension confirmed by RHC. Patient started on IV epoprostenol.”
-
Coding: I27.0 (Primary pulmonary hypertension) is the principal diagnosis. There is no underlying cause to code.
Case Study 2: PH Exacerbated by COPD
-
Scenario: A 68-year-old male with a known history of severe COPD and pulmonary hypertension is admitted for acute hypercapnic respiratory failure.
-
Documentation: “Admitted for acute-on-chronic respiratory failure secondary to COPD exacerbation. Patient has known pulmonary hypertension due to his underlying lung disease.”
-
Coding:
-
Principal Diagnosis: J44.1 (Chronic obstructive pulmonary disease with (acute) exacerbation)
-
Secondary Diagnosis: I27.23 (Pulmonary hypertension due to lung diseases and hypoxia)
-
Additional Code: J96.22 (Acute and chronic respiratory failure with hypercapnia)
-
Case Study 3: PH and Congestive Heart Failure
-
Scenario: A 75-year-old female is seen in the heart failure clinic for follow-up. She has systolic heart failure with reduced ejection fraction and echocardiography shows significant pulmonary hypertension.
-
Documentation: “Patient with ischemic cardiomyopathy, NYHA Class III. Echocardiogram shows severe pulmonary hypertension secondary to left heart disease.”
-
Coding: (For this outpatient encounter)
-
Primary Diagnosis: I50.21 (Acute systolic (congestive) heart failure) – or the code for the reason for the visit.
-
Secondary Diagnosis: I27.22 (Pulmonary hypertension due to left heart disease)
-
Secondary Diagnosis: I25.10 (Atherosclerotic heart disease of native coronary artery without angina pectoris)
-
Case Study 4: Chronic Thromboembolic PH Post-DVT
-
Scenario: A 52-year-old male presents to a PH specialist for evaluation of persistent dyspnea. He had a massive pulmonary embolism two years ago. A V/Q scan confirms the diagnosis of CTEPH.
-
Documentation: “Chronic thromboembolic pulmonary hypertension (CTEPH) confirmed. History of DVT and PE.”
-
Coding: (For this outpatient encounter)
-
Primary Diagnosis: I27.24 (Chronic thromboembolic pulmonary hypertension)
-
Secondary Diagnosis: I82.92 (Personal history of pulmonary embolism)
-
9. Beyond ICD-10: Linking Diagnosis to CPT and DRG
Accurate ICD-10 coding is essential for justifying medical necessity for procedures and services.
-
Common Procedures:
-
Right Heart Catheterization (RHC): CPT 93503. This is the definitive test for diagnosing and monitoring PH. The ICD-10 code (e.g., I27.21) justifies the need for this invasive procedure.
-
Echocardiogram: CPT 93306. Used for screening and monitoring PH. The ICD-10 code establishes medical necessity.
-
Pulmonary Function Tests (PFTs): CPT 94150, 94200, etc. Used to diagnose and characterize underlying lung disease in Group 3 PH.
-
-
Impact on DRG:
-
In the inpatient setting, the principal diagnosis drives the Major Diagnostic Category (MDC). A principal diagnosis of I27.0 or I27.21 would typically fall into MDC 05 (Diseases and Disorders of the Circulatory System). The presence of a MCC (Major Complication/Comorbidity), such as acute respiratory failure, or the performance of a procedure like RHC, will significantly increase the DRG weight and reimbursement.
-
10. Common Pitfalls and How to Avoid Them
-
Defaulting to I27.20: Always look for more specific documentation. Query if necessary.
-
Confusing Acute PE with CTEPH: I27.24 is for chronic, organized clots. Use I26.- codes for acute embolism.
-
Missequencing Cor Pulmonale: Remember to code first the underlying lung disease when using I27.81.
-
Ignoring the “Code Also” Note: Failing to code the underlying cause (e.g., COPD, heart failure) results in an incomplete claim and misses data critical for risk adjustment.
-
Assuming “PAH” is always I27.21: “PAH” is the name for WHO Group 1. If it’s idiopathic, it’s I27.0. If it’s associated with another condition, it’s I27.21.
11. The Future of PH Coding: ICD-11
The World Health Organization’s ICD-11 has been implemented in some countries and represents the future of medical classification. While the U.S. continues to use ICD-10-CM, it’s helpful to see the evolution. In ICD-11, PH codes are more logically integrated.
-
Example: BB01.0 Pulmonary arterial hypertension (replacing I27.0 and I27.21) with extension codes for etiology.
-
Example: BB01.1 Pulmonary hypertension due to left heart disease (replacing I27.22).
This structure reduces ambiguity and aligns even more closely with the WHO clinical classification.
12. Conclusion: Mastering the Nuances for Compliant Reimbursement
Accurate coding for pulmonary hypertension is a sophisticated process that requires a firm grasp of clinical pathophysiology, a meticulous approach to documentation review, and a strict adherence to ICD-10-CM guidelines. By moving beyond generic codes and leveraging the specificity offered by the I27.2- category, coders can ensure that the clinical story is accurately told, supporting appropriate reimbursement, robust data collection for research, and, ultimately, the highest quality of patient care. Mastery of this complex topic is not just about assigning numbers; it is about speaking the precise language of modern medicine.
13. Frequently Asked Questions (FAQs)
Q1: What is the difference between I27.0 and I27.21?
A: I27.0 (Primary pulmonary hypertension) is used for idiopathic PAH—PAH with no known cause. I27.21 (Secondary pulmonary arterial hypertension) is used for WHO Group 1 PAH that is associated with a known cause, such as connective tissue disease, HIV, or congenital heart disease.
Q2: My physician’s document only says “pulmonary hypertension.” What code should I use?
A: When the documentation lacks specificity regarding the type or cause, you must use I27.20 (Pulmonary hypertension, unspecified). However, this should prompt a query to the physician for more detailed information if possible.
Q3: How do I code a patient with both COPD and pulmonary hypertension?
A: If the documentation states or implies that the PH is due to the COPD, use I27.23 (Pulmonary hypertension due to lung diseases and hypoxia). You must also code also the COPD (e.g., J44.9). The sequencing depends on the reason for the encounter.
Q4: What is the correct code for pulmonary hypertension caused by sleep apnea?
A: Sleep apnea is a lung disease/hypoxia-related cause (WHO Group 3). Therefore, the correct code is I27.23. You must also code also the sleep apnea code (e.g., G47.33 Obstructive sleep apnea).
Q5: When should I use code I27.81 (Cor pulmonale)?
A: Use I27.81 when the physician specifically documents “cor pulmonale,” which is right heart failure resulting from pulmonary disease. Crucially, you must code first the underlying pulmonary condition (e.g., COPD, pulmonary fibrosis) that caused it.
Date: October 22, 2025
Author: The Medical Coding Specialist Team
Disclaimer: This article is intended for educational and informational purposes only and does not constitute medical or legal advice. While every effort has been made to ensure accuracy, medical coding guidelines are subject to change. Always consult the most current official ICD-10-CM coding manuals, payer-specific policies, and clinical documentation for definitive guidance.





