Imagine a intricate, living roadmap of rivers and tributaries, all hidden from direct view, yet responsible for sustaining the most complex organ in the human body—the brain. When something goes awry within this vascular network—a blockage, a weakening, a rupture—the consequences can be devastating. Stroke, aneurysm, and arteriovenous malformations are not just medical terms; they are life-altering events. In the high-stakes world of neurology and neurosurgery, the cerebral angiogram stands as a cornerstone diagnostic and guiding tool. It is the “gold standard” for visualizing the blood vessels of the brain, providing a dynamic, real-time movie of blood flow that no static image can match.
But in the modern healthcare ecosystem, a procedure’s clinical brilliance is only one part of the story. For every physical act performed by a physician, there is a parallel act of data translation performed by a medical coder. This translation, captured in codes like those from the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS), is what drives reimbursement, informs public health data, fuels clinical research, and impacts hospital revenue cycles. A miscoded cerebral angiogram is not merely a clerical error; it can lead to claim denials, inaccurate patient records, and flawed data that misrepresents the quality of care provided.
This article is designed to be the definitive guide for medical coders, health information management (HIM) professionals, and students seeking to master the intricate details of ICD-10-PCS coding for cerebral angiography. We will move beyond simple code look-ups and delve deep into the “why” and “how,” building a robust understanding from the ground up. We will explore the relevant anatomy, deconstruct the PCS code structure character by character, navigate complex procedural scenarios, and highlight common pitfalls. By the end of this journey, you will not just know which codes to assign; you will possess the confidence and knowledge to justify them, ensuring accuracy and integrity in this critical niche of neurological coding.
ICD-10-PCS Code for Cerebral Angiography
Table of Contents
Toggle2. Foundational Knowledge: Prerequisites for Accurate Coding
Before a single character of a PCS code can be assigned, a coder must be fluent in the language of the procedure itself. This foundational knowledge is the bedrock upon which accurate coding is built.
2.1. Understanding the “Why”: The Clinical Indications for a Cerebral Angiogram
A physician does not order an invasive procedure like a cerebral angiogram without a compelling clinical reason. Understanding these indications provides crucial context for the medical record and can sometimes guide coding decisions. Common indications include:
-
Suspected Acute Ischemic Stroke: To identify the location and extent of a blockage in a cerebral artery.
-
Detection and Evaluation of Cerebral Aneurysms: To visualize the size, shape, and location of a weakened, bulging area in a vessel wall.
-
Assessment of Arteriovenous Malformations (AVMs) and Fistulas: To map the complex tangles of abnormal connections between arteries and veins.
-
Vasospasm: Often following a subarachnoid hemorrhage, blood vessels can constrict dangerously; angiography assesses the severity.
-
Pre-surgical Planning: Providing a detailed vascular map for upcoming brain tumor resections or other neurosurgical procedures.
-
Evaluation of Traumatic Injury: To identify vessel dissection, laceration, or pseudoaneurysm after head trauma.
-
Follow-up after Treatment: To check the status of a coiled aneurysm, a stented artery, or an AVM that has been treated with embolization.
2.2. A Primer on Cerebral Vasculature: The Roadmap of the Brain’s Blood Supply
The brain is supplied by two primary pairs of arteries: the internal carotid arteries and the vertebral arteries.
-
The Internal Carotid Arteries: These ascend through the neck and enter the skull. They primarily supply the anterior (front) and middle parts of the brain, including the frontal, parietal, and temporal lobes. Their major branches include the:
-
Ophthalmic Artery
-
Anterior Cerebral Artery (ACA)
-
Middle Cerebral Artery (MCA) – the most common site of ischemic strokes.
-
Posterior Communicating Artery
-
-
The Vertebral Arteries: These ascend through the cervical vertebrae and join at the brainstem to form the Basilar Artery. This system supplies the posterior (back) of the brain, including the brainstem, cerebellum, and occipital lobes. Key branches include:
-
Posterior Inferior Cerebellar Artery (PICA)
-
Anterior Inferior Cerebellar Artery (AICA)
-
Superior Cerebellar Artery
-
Posterior Cerebral Arteries (PCA)
-
At the base of the brain, the Circle of Willis is a circulatory anastomosis that connects the carotid and vertebrobasilar systems, providing a potential safety net for blood flow.
[Placeholder for Image: A detailed, labeled diagram of the cerebral vasculature, including the Circle of Willis.]
*Caption: A detailed map of the cerebral vasculature is essential for understanding the specific body part values in ICD-10-PCS.*
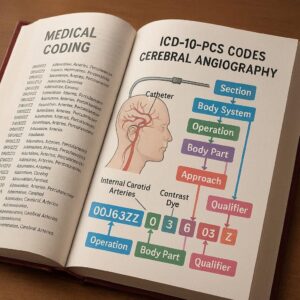
2.3. The ICD-10-PCS Framework: A Brief Overview of its Structure
ICD-10-PCS is a multi-axial, seven-character alphanumeric code set. Each character has a specific meaning, and together they provide a highly specific description of a procedure.
-
1st Character: Section (e.g., Medical and Surgical, Imaging, Measurement and Monitoring)
-
2nd Character: Body System
-
3rd Character: Root Operation (the objective of the procedure)
-
4th Character: Body Part
-
5th Character: Approach (how the site was reached)
-
6th Character: Device
-
7th Character: Qualifier
For cerebral angiography, our focus will be primarily within the Imaging Section (B).
3. Deconstructing the ICD-10-PCS Code for Cerebral Angiography
Let’s build a cerebral angiogram code from the ground up, examining the options and definitions for each character.
3.1. The First Character: Section B – Imaging
The Imaging section includes procedures that include “the recording, replication, production, or viewing of a static or dynamic visual representation of a body part, organ, or region.” This is the correct section for a cerebral angiogram, as its primary purpose is to produce a visual representation (the angiographic images) of the cerebral vessels.
3.2. The Second Character: Body System 2 – Central Nervous System and Cranial Nerves
For procedures imaging the brain and its blood vessels, the correct Body System is 2 – Central Nervous System and Cranial Nerves.
3.3. The Third Character: Root Operation – Plain Radiography vs. Computerized Tomography
This character defines the type of imaging technology used.
-
Plain Radiography (0): This is the classic, “fluoro-guided” catheter angiogram. It involves the use of a fluoroscope to produce real-time, dynamic X-ray images. Contrast dye is injected, and the radiologist watches it flow through the vessels. This is the most common root operation for a traditional diagnostic cerebral angiogram.
-
Computerized Tomography (2): This refers to a CT Angiogram (CTA). In a CTA, contrast is injected intravenously (IV), and a CT scanner takes rapid, thin-slice images of the head, which are then reconstructed into 3D models of the vasculature. It is less invasive than a catheter angiogram but may offer less dynamic detail.
3.4. The Fourth Character: Body Part/Region – Specifying the Precise Vessels
This is one of the most critical and detailed aspects of coding a cerebral angiogram. The coder must review the procedure report carefully to see which vessels were specifically selected and injected with contrast.
-
Intracranial Artery (70): A general value used when the specific intracranial artery is not documented.
-
Cerebral Artery (71): Used for imaging of the anterior, middle, or posterior cerebral arteries.
-
Internal Carotid Artery (65): Used when the cervical (neck) portion of the internal carotid is imaged. If the catheter is advanced into the intracranial internal carotid and its branches are imaged, multiple codes may be necessary.
-
Vertebral Artery (68): Used for imaging the vertebral artery.
-
Head Arteries (6V): This is a broader category used for imaging of the extracranial arteries of the head, such as the external carotid artery and its branches.
-
Cerebral Vein (73) / Intracranial Vein (74): Used for cerebral venography (imaging of the veins).
Crucial Note on Laterality: Many of these body parts are bilateral. The coder must assign separate codes for the right and left sides if both are imaged and the report specifies the laterality. For example, a bilateral internal carotid angiogram would require two codes: one for the right internal carotid artery and one for the left.
3.5. The Fifth Character: Approach – The Path to the Target
The approach describes the technique used to reach the region being imaged. For catheter-based angiography, this is almost always Percutaneous (3). This means the procedure was performed by puncturing the skin (e.g., in the groin for a femoral approach or the wrist for a radial approach) and threading a catheter through the vessels to the target.
For a CT Angiogram (CTA), the contrast is injected intravenously, so the approach is Via Natural or Artificial Opening (7), as the IV line enters the venous system through a natural opening (the skin puncture is considered the “artificial opening” component of the approach definition).
3.6. The Sixth Character: Device – The Crucial Role of Intracranial Catheters
This character identifies any device that remains in the body after the procedure concludes. For a diagnostic cerebral angiogram, no device remains. The catheter is removed at the end of the procedure. Therefore, the correct value is ZZ – No Device.
However, if the diagnostic angiogram is immediately followed by an interventional procedure (e.g., coiling or stenting), the diagnostic angiogram code would still be ZZ, as its purpose was solely imaging. The device placed during the intervention (e.g., the coil or stent) would be coded in the separate interventional procedure code from the Medical and Surgical section.
3.7. The Seventh Character: Qualifier – Contrast and Other Agents
This character specifies the contrast material used. For virtually all cerebral angiograms, this is High Osmolar Contrast (A) or, more commonly in modern practice, Low Osmolar Contrast (B). The radiology report will typically specify the type of contrast used (e.g., Iohexol, Ioversol). If the type is unspecified, the coder should use X – Diagnostic, which is a catch-all for unspecified contrast.
ICD-10-PCS Code Table for Common Cerebral Angiography Procedures
The table below provides a quick reference for building common cerebral angiogram codes.
| Procedure Description | 1st (Section) | 2nd (Body System) | 3rd (Root Operation) | 4th (Body Part) | 5th (Approach) | 6th (Device) | 7th (Qualifier) | Complete Code |
|---|---|---|---|---|---|---|---|---|
| Diagnostic Left Carotid Angiogram | B (Imaging) | 2 (CNS) | 0 (Plain Radiography) | 65 (Left Int Carotid Art) | 3 (Percutaneous) | ZZ (No Device) | B (Low Osmolar Contrast) | B20.65.3ZZB |
| Diagnostic Right Vertebral Angiogram | B (Imaging) | 2 (CNS) | 0 (Plain Radiography) | 68 (Right Vertebral Art) | 3 (Percutaneous) | ZZ (No Device) | B (Low Osmolar Contrast) | B20.68.3ZZB |
| CT Angiogram of Cerebral Arteries | B (Imaging) | 2 (CNS) | 2 (Computerized Tomo) | 71 (Cerebral Artery) | 7 (Via Natural/Art Open) | ZZ (No Device) | B (Low Osmolar Contrast) | B22.71.7ZZB |
| Diagnostic Angiogram, Unspecified Intracranial Artery | B (Imaging) | 2 (CNS) | 0 (Plain Radiography) | 70 (Intracranial Artery) | 3 (Percutaneous) | ZZ (No Device) | X (Diagnostic) | B20.70.3ZZX |
4. Coding in Action: Practical Scenarios and Code Building
Let’s apply our knowledge to realistic procedural reports.
Scenario 1: Diagnostic Cerebral Angiogram via Femoral Access
Procedure Note Excerpt: “After informed consent, the patient was prepped and draped in the usual sterile fashion. Under local anesthesia, the right common femoral artery was accessed using a Seldinger technique. A 5-French sheath was placed. A diagnostic catheter was advanced over a guidewire under fluoroscopic guidance into the aortic arch. Selective catheterization of the left internal carotid artery was performed. Contrast injection was performed with filming in multiple projections, demonstrating normal anatomy of the left internal carotid, anterior cerebral, and middle cerebral arteries. The catheter was then withdrawn, and the sheath was removed. Hemostasis was achieved with manual compression.”
Coding Analysis:
-
Procedure: Diagnostic angiogram.
-
Root Operation: Plain Radiography (0) – used fluoroscopy.
-
Body Part: Left Internal Carotid Artery (65). The report specifies selective catheterization and imaging of this vessel and its branches (ACA, MCA).
-
Approach: Percutaneous (3) – via the femoral artery.
-
Device: No Device (ZZ) – the catheter and sheath were removed.
-
Qualifier: The type of contrast isn’t specified, so we use X (Diagnostic).
Assigned Code: B20.65.3ZZX – Plain Radiography of Left Internal Carotid Artery, Percutaneous Approach, Diagnostic Contrast.
Scenario 2: CT Angiogram of the Head for Aneurysm Detection
Procedure Note Excerpt: “The patient was placed on the CT table. An 18-gauge IV was placed in the right antecubital vein. Using a power injector, 80 mL of Iohexol contrast was administered. Helical CT imaging of the head was performed from the base of C1 through the vertex. 3D reconstructions of the intracranial vasculature were created. The study was negative for aneurysm.”
Coding Analysis:
-
Procedure: CT Angiogram.
-
Root Operation: Computerized Tomography (2).
-
Body Part: Cerebral Artery (71) – the purpose was to evaluate the intracranial arteries for aneurysm.
-
Approach: Via Natural or Artificial Opening (7) – intravenous injection.
-
Device: No Device (ZZ).
-
Qualifier: Low Osmolar Contrast (B) – Iohexol is a low-osmolar agent.
Assigned Code: B22.71.7ZZB – Computerized Tomography of Cerebral Artery, Via Natural or Artificial Opening, Low Osmolar Contrast.
Scenario 3: Cerebral Angiogram with Subsequent Mechanical Thrombectomy
This is a more complex but common scenario in comprehensive stroke centers.
Procedure Note Excerpt (Part 1 – Diagnostic): “Access was gained in the right femoral artery. An aortic arch angiogram was performed. Selective catheterization of the left internal carotid artery was performed. Angiography confirmed a large vessel occlusion of the M1 segment of the left middle cerebral artery.”
Procedure Note Excerpt (Part 2 – Intervention): “A guide catheter was advanced into the left internal carotid artery. A microcatheter and stent retriever were advanced through the guide catheter, across the clot. The stent retriever was deployed and then withdrawn, removing the thrombus. Post-procedure angiography demonstrated complete recanalization (TICI 3 flow) of the left MCA territory.”
Coding Analysis:
This requires two separate PCS codes from different sections.
-
For the Diagnostic Angiogram:
-
Section: Imaging (B)
-
Code: B20.65.3ZZX (Plain Radiography of Left Internal Carotid Artery, Percutaneous Approach, Diagnostic Contrast). This captures the diagnostic imaging that identified the blockage. The device is ZZ because the initial diagnostic catheter does not remain.
-
-
For the Mechanical Thrombectomy:
-
Section: Medical and Surgical (0)
-
Body System: Central Nervous System (0)
-
Root Operation: Extraction (D) – The objective is to pull out the obstruction.
-
Body Part: Left Middle Cerebral Artery (71)
-
Approach: Percutaneous (3)
-
Device: ZZ (No Device) – The stent retriever is removed.
-
Qualifier: ZZ (None)
-
Code: 00D.63ZZ – Extraction of Left Middle Cerebral Artery, Percutaneous Approach.
-
[Placeholder for Image: A side-by-side comparison of a cerebral angiogram image showing a blocked vessel (pre-thrombectomy) and a clear vessel (post-thrombectomy).]
Caption: Angiographic images from a mechanical thrombectomy procedure. The diagnostic phase (left) identifies the occlusion, coded in the Imaging section. The therapeutic phase (right) restores flow, coded in the Medical and Surgical section.
5. Navigating Common Pitfalls and Complexities
5.1. Diagnostic Angiogram vs. Angiogram as Part of an Intervention
This is the single most important distinction. A “diagnostic” angiogram is a self-contained procedure whose sole purpose is to obtain images. If an intervention follows, the initial catheter placement and imaging that guide that intervention are not coded separately. The intervention code includes all necessary catheter placement and roadmapping. Only if a complete, formal diagnostic study is performed and interpreted before the decision to intervene is made, should a separate imaging code be assigned. The documentation must clearly support this sequence.
5.2. The Importance of Laterality in Coding
ICD-10-PCS is exquisitely specific about laterality. Coding a bilateral procedure with a single unilateral code is incorrect. If the report states “bilateral internal carotid injections,” you must assign:
-
B20.65.3ZZB (Left)
-
B20.66.3ZZB (Right)
5.3. Differentiating Between Catheter Types and Their Coding Impact
The type of catheter used (e.g., diagnostic vs. guide catheter) does not change the Imaging code. The Imaging code is concerned with the act of imaging, not the tools used to deliver contrast (as long as they are removed). The device character (6th) is only for items that remain.
6. The Synergy of PCS and CPT: A Coder’s Dual Responsibility
In the United States, coders often work with two code sets: ICD-10-PCS for inpatient procedures and CPT (Current Procedural Terminology) for outpatient and physician services. It is vital to understand that they are different systems with different rules.
-
ICD-10-PCS (B20.65.3ZZB): Describes the objective of the procedure (Plain Radiography of the Left Internal Carotid Artery).
-
CPT (e.g., 36222 – 36224): Describes the work of the physician (Selective catheterization and radiologic supervision & interpretation).
A single ICD-10-PCS code might correspond to multiple CPT codes depending on the specific vessels catheterized. Coders must be proficient in both systems and apply them in the correct context (inpatient vs. outpatient).
7. Conclusion: Summarizing the Content of the Article in Three Lines
Mastering ICD-10-PCS for cerebral angiography requires a deep understanding of neurovascular anatomy and a meticulous approach to deconstructing the procedure report. Accurate coding hinges on correctly identifying the imaging modality, the specific vessels imaged, the procedural approach, and the use of contrast, while carefully distinguishing standalone diagnostic studies from those integral to an intervention. By applying this structured methodology, coders ensure data integrity, support appropriate reimbursement, and contribute meaningfully to patient care documentation.
8. Frequently Asked Questions (FAQs)
Q1: What is the difference between a code from the Imaging section (B) and the Medical and Surgical section (0) for a cerebral angiogram?
A: The Imaging section (B) is used when the primary goal of the procedure is to obtain diagnostic images. The Medical and Surgical section (0) is used when the primary goal is therapeutic (e.g., to repair an aneurysm, remove a clot, or embolize a vessel). A diagnostic angiogram that is followed by an intervention may have codes from both sections.
Q2: How do I code a cerebral angiogram that images multiple vessels?
A: You must assign a separate code for each uniquely defined body part that is selectively catheterized and imaged. For example, if the report documents selective imaging of the right internal carotid artery and the left vertebral artery, you would assign two codes: B20.66.3ZZB and B20.68.3ZZB.
Q3: The operative report just says “cerebral angiogram” without specifying the vessels. What should I do?
A: You should query the physician for clarification. If a query is not possible, you must use the most general, appropriate code. In this case, that would be B20.70.3ZZX (Plain Radiography of Intracranial Artery, Unspecified), but this should be a last resort as it lacks specificity.
Q4: Why is the Device character always “ZZ” for a diagnostic angiogram?
A: Because in a purely diagnostic procedure, all catheters, sheaths, and guidewires are removed upon completion. The Device character is only used to report a device that remains in the body after the procedure is concluded.
Q5: How do I code a venous phase of a cerebral angiogram?
A: If the venous phase is part of a standard arterial study, it is included and not coded separately. However, if a separate, distinct cerebral venogram is performed (e.g., to evaluate for venous sinus thrombosis), it would be coded separately using Body Part values like 73 (Cerebral Vein) or 74 (Intracranial Vein).
9. Additional Resources
-
The Official ICD-10-PCS Guidelines: Published annually by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). This is the ultimate authority.
-
American Health Information Management Association (AHIMA): Offers a wealth of resources, including practice briefs, webinars, and the Journal of AHIMA with coding articles.
-
American Academy of Professional Coders (AAPC): Provides certification, training, and networking opportunities for medical coders.
-
RadiologyInfo.org: A patient-friendly site from the ACR and RSNA that provides excellent descriptions and videos of procedures, which can aid coder understanding.
-
Netter’s Atlas of Human Anatomy / Frank H. Netter MD: An indispensable visual reference for human anatomy, including the cerebral vasculature.
Date: November 22, 2025
Author: Dr. Anya Sharma, MD, CIC, CCS-P
Disclaimer: This article is intended for educational purposes and to provide a foundational understanding of ICD-10-PCS coding principles. It is not a substitute for the official ICD-10-PCS guidelines, codebooks, or professional coding advice. Medical coders must use the current year’s official resources and adhere to their facility’s coding policies when assigning codes.





