In the intricate world of medical coding, few procedures demand as much precision and nuanced understanding as the hysterectomy. As one of the most common major gynecological surgeries performed worldwide, its accurate representation in a patient’s medical record is paramount. The transition to ICD-10-PCS (International Classification of Diseases, Tenth Revision, Procedure Coding System) marked a seismic shift from the relative simplicity of ICD-9-CM volume 3. No longer is a single code like “68.9” sufficient. Instead, ICD-10-PCS requires coders to become architectural linguists, deconstructing a complex surgical procedure into its fundamental components and rebuilding it into a precise, seven-character alphanumeric code that tells the complete story of the intervention.
Why does this matter? The implications of accurate hysterectomy coding ripple through the entire healthcare ecosystem. It directly impacts hospital reimbursement, ensuring that the resources, skill, and time expended are fairly compensated through DRGs (Diagnosis-Related Groups). It fuels vital health data analytics, enabling researchers and public health officials to track surgical trends, outcomes, and prevalence of conditions like fibroids or endometriosis. It affects quality metrics and patient safety reporting. An incorrectly coded hysterectomy can lead to claim denials, audits, and a distorted picture of a facility’s surgical profile. This article is designed to be your definitive guide, a deep dive into the anatomy of an ICD-10-PCS hysterectomy code. We will dissect each character, explore the subtle yet critical distinctions between root operations, and navigate the complexities of anatomical approaches and device reporting. By the end, you will possess the knowledge and confidence to code even the most complex hysterectomy procedures with unwavering accuracy.
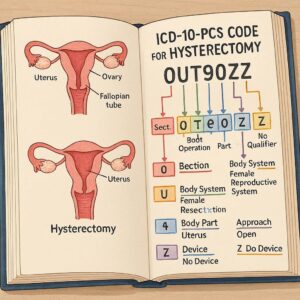
ICD-10-PCS Code for Hysterectomy
2. Understanding the Foundation: The Structure of ICD-10-PCS
Before we address the specifics of hysterectomy, one must have a firm grasp of the ICD-10-PCS framework. Every code is a seven-character string, where each character represents a specific aspect of the procedure. For the Medical and Surgical section (the section where nearly all hysterectomies reside), the characters represent the following:
-
Section (1st Character): Always 0 for Medical and Surgical.
-
Body System (2nd Character): For hysterectomy, this is almost always U for the Female Reproductive System.
-
Root Operation (3rd Character): This is the core objective of the procedure. It is the most critical and often the most challenging character to determine for a hysterectomy. We will explore the options (Resection, Excision, Extirpation, Destruction) in exhaustive detail.
-
Body Part (4th Character): This specifies the precise part of the uterus or surrounding structures that were operated on (e.g., Uterus, Cervix, Endometrium).
-
Approach (5th Character): This describes the technique used to reach the surgical site (e.g., Open, Laparoscopic, Percutaneous Endoscopic, Via Natural or Artificial Opening).
-
Device (6th Character): This character specifies if a device was left in place after the procedure. For hysterectomies, this is crucial for certain approaches and can include drainage devices or radioactive elements.
-
Qualifier (7th Character): This provides additional information about the procedure. For hysterectomies, this is often a Z for No Qualifier, but it can specify diagnostic or other contextual details.
Understanding this structure is the first step. The real art lies in applying it to the vast spectrum of hysterectomy techniques.
3. The Central Question: Identifying the Correct Root Operation for Hysterectomy
The root operation is the cornerstone of the ICD-10-PCS code. Misidentifying it will result in an entirely incorrect code. The official coding guidelines and the PCS Tables provide the definitions, but their application requires careful analysis of the operative report. For hysterectomy, the four potential root operations are Resection, Excision, Extirpation, and Destruction.
3.1. Root Operation: Resection (Root Operation 0UT)
Definition: Resection is defined as “cutting out or off, without replacement, all of a body part.” The key phrase is “all of a body part.”
Application to Hysterectomy: This is the most common root operation for a total hysterectomy. When the entire uterus, including the corpus and cervix, is completely removed, the procedure qualifies as a Resection.
-
Total Hysterectomy (with or without salpingo-oophorectomy): The removal of the entire uterus and cervix is a resection of the body part “Uterus.”
-
Supracervical (Subtotal) Hysterectomy: This is a critical distinction. In a supracervical hysterectomy, the cervix is intentionally left in place. Therefore, the entire body part “Uterus” is not removed. This procedure is NOT a Resection. It would typically be coded as an Excision (see below).
Coding Focus: The coder must confirm from the operative report that the surgeon has documented the removal of the entire uterus. Phrases like “total hysterectomy,” “uterus and cervix removed as a single specimen,” or “complete removal of the uterine corpus and cervix” point directly to Resection.
3.2. Root Operation: Excision (Root Operation 0UB)
Definition: Excision is defined as “cutting out or off, without replacement, a portion of a body part.” The key phrase is “a portion of a body part.”
Application to Hysterectomy: This root operation applies when only a part of the uterus is removed.
-
Supracervical (Subtotal) Hysterectomy: As mentioned, this procedure involves the removal of the uterine corpus while leaving the cervix. Since only a portion of the entire “Uterus” body part is removed, it is coded as an Excision of the Uterus.
-
Trachelectomy: This is the surgical removal of the cervix. Since the cervix is a specific body part in ICD-10-PCS, and the entire cervix is removed, this is actually a Resection of the Cervix, not an Excision.
-
Endometrial Ablation (with tissue removal): Some ablation techniques, like hysteroscopic resection, involve the physical removal of the endometrium. If the endometrium is cut out and removed, this would be coded as an Excision of the Endometrium.
Coding Focus: The operative report must be scrutinized to determine if the procedure was partial. For a supracervical hysterectomy, the report will explicitly state that the cervix was preserved.
3.3. Root Operation: Extirpation (Root Operation 0UC)
Definition: Extirpation is defined as “taking or cutting out solid matter from a body part.” The key concept is the removal of “solid matter” such as a foreign body, thrombus, or calculus from within a body part, where the body part itself remains.
Application to Hysterectomy: This root operation is rarely used for a classic hysterectomy but is highly relevant for related procedures.
-
Removal of a Leiomyoma (Fibroid): If a surgeon performs a myomectomy—the removal of fibroids from the uterine wall—the root operation is Extirpation. The solid matter (the fibroid) is taken out, but the uterus (the body part) is repaired and remains. This is distinct from a hysterectomy where the uterus itself is removed.
-
Evacuation of Hematometra: The removal of retained blood from the uterine cavity is also an Extirpation.
Coding Focus: Do not confuse a myomectomy (Extirpation) with a hysterectomy (Resection/Excision). They are fundamentally different procedures with different objectives.
3.4. Root Operation: Destruction (Root Operation 0U5)
Definition: Destruction is defined as “physical eradication of all or a portion of a body part by the direct use of energy, force, or a destructive agent.” The key is that the tissue is eradicated in situ, not physically cut out. No specimen is sent to pathology.
Application to Hysterectomy: This is not used for a standard hysterectomy. However, it is the correct root operation for certain types of endometrial ablation.
-
Endometrial Ablation (without tissue removal): Procedures that use thermal energy (e.g., balloon ablation), microwave, or cryoablation to destroy the endometrial lining are coded as Destruction. The endometrium is eradicated by energy, not surgically excised.
Coding Focus: The absence of a tissue specimen is a major clue. If the procedure note describes the application of energy to ablate tissue and no specimen is sent to pathology, Destruction is the likely root operation.
4. The Surgical Approach: The Fourth Character’s Pivotal Role
The approach character describes the technique used to reach the surgical site. For hysterectomy, this has significant implications for coding and reimbursement. The common approaches are:
-
Open (0): A traditional incision is made into the abdominal cavity (e.g., Pfannenstiel or vertical midline incision).
-
Percutaneous Endoscopic (4): This is the approach for laparoscopic-assisted procedures. The surgeon uses a laparoscope inserted through small abdominal incisions to visualize the procedure and uses other instruments to perform the hysterectomy.
-
Via Natural or Artificial Opening (7): This refers to procedures performed entirely through the vagina or through an artificial opening like a stoma. A total vaginal hysterectomy uses this approach.
-
Via Natural or Artificial Opening Endoscopic (8): This is used for hysteroscopic procedures that are performed through the cervix (a natural opening) with the use of an endoscope. This would be used for hysteroscopic excision or destruction of the endometrium.
-
External (X): Used for procedures performed from outside the body, such as external beam radiation. Not used for hysterectomy.
Combination Approaches: A single procedure may use multiple approaches. ICD-10-PCS guidelines state that the approach character is coded to the technique used to reach the deepest body part that was the focus of the procedure. For example, in a Laparoscopically Assisted Vaginal Hysterectomy (LAVH), the laparoscopic portion is used to address adhesions or the adnexa, but the uterus itself is removed through the vagina. Therefore, the root operation of Resection of the Uterus would take the approach 7 (Via Natural or Artificial Opening).
5. The Body Part Character: Pinpointing the Uterine Anatomy
The body part character specifies the anatomical site. The choices in the Female Reproductive System body system (2nd character U) include:
-
Uterus (0): This represents the entire organ (corpus and cervix).
-
Cervix (1): The uterine cervix.
-
Endometrium (2): The lining of the uterus.
-
Corpus Uteri (3): The body of the uterus above the cervix.
The selection is straightforward based on the root operation:
-
For a Total Hysterectomy (Resection), the body part is Uterus (0).
-
For a Supracervical Hysterectomy (Excision), the body part is also Uterus (0), because you are excising a portion of the entire “Uterus” body part.
-
For a Trachelectomy (Resection), the body part is Cervix (1).
-
For an Endometrial Ablation/Excision, the body part is Endometrium (2).
6. The Device Character: A Crucial and Often-Missed Detail
The device character indicates if a device was left in place. For many hysterectomies, this will be Z (No Device). However, there are two critical exceptions:
-
Drainage Device (0): If a surgical drain (e.g., Jackson-Pratt drain) is placed in the surgical bed at the end of the procedure, the device character is 0.
-
Radioactive Element (U): This is used in some cancer treatments where a radioactive substance is placed in a body cavity. It is rarely used in a standard hysterectomy but is a valid option in the table.
Important Note: The device character is only used to report devices that remain after the procedure is completed. Surgical instruments, sutures used for re-anastomosis, and temporary retractors are not coded here.
7. Putting It All Together: Practical Coding Scenarios and Examples
Let’s synthesize everything we’ve learned into practical coding exercises.
Scenario 1: Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy (TAH-BSO) for Fibroids
-
Operative Report: The surgeon performs an open procedure via a Pfannenstiel incision. The uterus, cervix, fallopian tubes, and ovaries are removed en bloc. A surgical drain is left in the pelvis.
-
Coding Analysis:
-
The removal of the entire uterus and cervix is a Resection (T).
-
The body system is Female Reproductive (U).
-
The body part is Uterus (0). (Note: The adnexal removal requires separate codes).
-
The approach is Open (0).
-
A drain was left, so the device is Drainage Device (0).
-
The qualifier is No Qualifier (Z).
-
-
ICD-10-PCS Code: 0UT00ZZ – Resection of Uterus, Open Approach, with Drainage Device.
-
Additional Codes Required: You would also assign codes for the bilateral salpingectomy (0UT20ZZ) and bilateral oophorectomy (0UT20ZZ) using the Resection root operation.
Scenario 2: Laparoscopic Supracervical Hysterectomy (LSH)
-
Operative Report: Using a laparoscopic approach, the surgeon morcellates and removes the uterine corpus. The cervix is carefully preserved. No drain is placed.
-
Coding Analysis:
-
Only the uterine corpus is removed, leaving the cervix. This is an Excision (B) of a portion of the uterus.
-
Body system is Female Reproductive (U).
-
Body part is Uterus (0).
-
The approach is Percutaneous Endoscopic (4).
-
No device was left, so device is No Device (Z).
-
Qualifier is No Qualifier (Z).
-
-
ICD-10-PCS Code: 0UB44ZZ – Excision of Uterus, Percutaneous Endoscopic Approach.
Scenario 3: Total Vaginal Hysterectomy
-
Operative Report: The surgeon removes the entire uterus and cervix through the vaginal canal without any laparoscopic assistance.
-
Coding Analysis:
-
The entire uterus is removed, so it is a Resection (T).
-
Body system is Female Reproductive (U).
-
Body part is Uterus (0).
-
The approach is Via Natural or Artificial Opening (7).
-
No device, so No Device (Z).
-
Qualifier is No Qualifier (Z).
-
-
ICD-10-PCS Code: 0UT70ZZ – Resection of Uterus, Via Natural or Artificial Opening.
Scenario 4: Hysteroscopic Endometrial Resection for Menorrhagia
-
Operative Report: A hysteroscope is passed through the cervix. The endometrium is systematically resected using an electrosurgical loop and the tissue is removed for pathology.
-
Coding Analysis:
-
The endometrium is being cut out and removed. This is an Excision (B) of a portion of a body part (the endometrium).
-
Body system is Female Reproductive (U).
-
Body part is Endometrium (2).
-
The approach is Via Natural or Artificial Opening Endoscopic (8) (through the cervix with a scope).
-
No device, so No Device (Z).
-
Qualifier is No Qualifier (Z).
-
-
ICD-10-PCS Code: 0UB82ZZ – Excision of Endometrium, Via Natural or Artificial Opening Endoscopic.
Common Hysterectomy Procedures and Their ICD-10-PCS Codes
| Procedure Name | Clinical Description | Root Operation | Body Part | Approach | ICD-10-PCS Code (Example, No Device) |
|---|---|---|---|---|---|
| Total Abdominal Hysterectomy | Open removal of entire uterus & cervix | Resection (T) | Uterus (0) | Open (0) | 0UT00ZZ |
| Total Vaginal Hysterectomy | Vaginal removal of entire uterus & cervix | Resection (T) | Uterus (0) | Via Natural Opening (7) | 0UT70ZZ |
| Laparoscopic Total Hysterectomy | Laparoscopic removal of entire uterus & cervix | Resection (T) | Uterus (0) | Percutaneous Endoscopic (4) | 0UT44ZZ |
| Supracervical Hysterectomy | Removal of uterine corpus, cervix preserved | Excision (B) | Uterus (0) | Varies (e.g., 0,4) | 0UB44ZZ (Laparoscopic) |
| Trachelectomy | Removal of the cervix | Resection (T) | Cervix (1) | Varies (e.g., 0,7) | 0UT10ZZ (Open) |
| Hysteroscopic Myomectomy | Removal of fibroid from within uterus | Extirpation (C) | Uterus (0) | Via Nat/Art Open Endo (8) | 0UC82ZZ |
| Endometrial Ablation (Thermal) | Destruction of endometrium with energy | Destruction (5) | Endometrium (2) | Via Nat/Art Open Endo (8) | 0U582ZZ |
This table provides common examples. The final code must always be based on the complete operative report.
8. Conclusion
Accurate ICD-10-PCS coding for hysterectomy hinges on a meticulous analysis of the operative report to determine the correct root operation—Resection for total removal, Excision for partial removal. The surgical approach must reflect the technique used to access the deepest part of the procedure, while careful attention must be paid to the documentation of any devices left in situ. By systematically applying this foundational knowledge, coders can ensure precision, support appropriate reimbursement, and contribute to the integrity of vital healthcare data.
9. Frequently Asked Questions (FAQs)
Q1: How do I code a radical hysterectomy?
A radical hysterectomy involves the removal of the uterus, cervix, parametria, and upper vagina. In ICD-10-PCS, this is still coded as a Resection of the Uterus (0UT*). The radical nature of the procedure, including the removal of surrounding tissue, is captured by the root operation definition of “cutting out,” which can include adjacent tissue. The specific body parts removed (e.g., parametria) may require additional codes for their excision/resection.
Q2: What is the difference between a laparoscopic hysterectomy (0UT44ZZ) and a laparoscopically assisted vaginal hysterectomy (LAVH) coded as 0UT70ZZ?
The difference lies in the approach character. In a pure laparoscopic hysterectomy, the uterus is detached and often removed through the laparoscopic ports (sometimes with morcellation). The approach is Percutaneous Endoscopic (4). In an LAVH, the laparoscopic portion is used to assist (e.g., lysing adhesions, securing blood vessels), but the uterus is ultimately detached and removed through the vagina. Since the deepest part of the procedure (the removal of the uterus) is done through the vagina, the approach is Via Natural or Artificial Opening (7).
Q3: A supracervical hysterectomy removes the “corpus uteri.” Why is the body part “Uterus” and not “Corpus Uteri”?
This is a fundamental concept in PCS. The body part value “Uterus” represents the whole organ. When you perform a supracervical hysterectomy, you are excising a portion of that whole organ. The body part value “Corpus Uteri” is used when the procedure is performed specifically on the corpus, such as a biopsy of the uterine wall, not when a portion of the whole organ is being removed.
Q4: How do I handle a hysterectomy that is converted from laparoscopic to open?
ICD-10-PCS guidelines state that you code the approach that was used to perform the majority of the procedure. If the surgeon started laparoscopically but converted to an open procedure to complete the hysterectomy, the approach would be Open (0).
Date: November 28, 2025
Author: AI-Assisted Medical Coding Specialist
Disclaimer: This article is intended for educational and informational purposes only. It is not a substitute for professional medical coding advice, official coding guidelines, or the current ICD-10-PCS code set. Coders must always consult the most recent official resources and facility-specific policies when assigning codes.





