Within the intricate landscape of modern medicine, few conditions are as insidiously pervasive and surgically challenging as adhesions. These bands of scar tissue, which form abnormally between organs and structures, are a common sequel to surgery, infection, or trauma. They can lie dormant for years, only to manifest suddenly as debilitating pain, dangerous bowel obstructions, or infertility. For surgeons, lysis of adhesions—the precise cutting and freeing of these fibrous bands—is a delicate and often complex procedure requiring immense skill. For the medical coder, however, this procedure represents a different kind of challenge: one of meticulous precision, anatomical knowledge, and a deep understanding of the ICD-10-PCS system.
The transition to ICD-10-PCS marked a paradigm shift in procedural coding, moving from a limited-number system to one of immense specificity and logic. Coding for a lysis of adhesions is a prime example of where this specificity is paramount. An incorrect code can misrepresent the patient’s condition, the surgeon’s work, and the resources utilized, leading to denied claims, compliance issues, and flawed data. This article is designed to be the definitive guide for medical coders, auditors, and healthcare professionals seeking to master the art and science of accurately classifying lysis of adhesions procedures. We will embark on a detailed journey through the ICD-10-PCS framework, deconstruct the procedure from a clinical and coding perspective, and navigate the nuanced scenarios that test even the most experienced coders. By the end, you will possess the knowledge to approach any adhesiolysis coding scenario with confidence and accuracy.
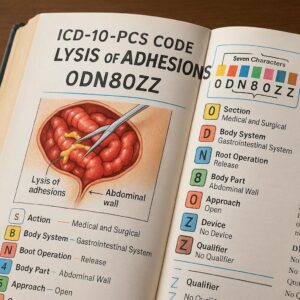
ICD-10-PCS Code for Lysis of Adhesions
2. Understanding the Foundation: The ICD-10-PCS Framework
Before delving into the specifics of adhesiolysis, one must have a firm grasp of the ICD-10-PCS structure. Unlike its predecessor, ICD-9-CM, which often relied on a single code for a broad procedure, ICD-10-PCS uses a multi-axial, seven-character alphanumeric code. Each character has a specific meaning, and together, they create a precise description of the procedure performed.
The Seven Characters of a PCS Code
-
Section: The first character identifies the broad section where the procedure is classified (e.g., Medical and Surgical, Obstetrics, Placement).
-
Body System: The second character specifies the general body system (e.g., Gastrointestinal, Musculoskeletal, Respiratory).
-
Root Operation: The third character is the cornerstone of the code. It defines the objective of the procedure—what the provider did (e.g., cutting, removing, putting in).
-
Body Part: The fourth character identifies the specific body part upon which the root operation was performed.
-
Approach: The fifth character describes the technique used to reach the site of the procedure (e.g., open, percutaneous, laparoscopic).
-
Device: The sixth character specifies if a device was left in place. For lysis of adhesions, this is almost always “Z” for No Device.
-
Qualifier: The seventh character provides additional information about the procedure. For most adhesiolysis codes, this is “Z” for No Qualifier.
The Medical and Surgical Section (0)
The vast majority of lysis of adhesions procedures fall under the Medical and Surgical section, represented by the first character 0. This section encompasses procedures performed for the purpose of cutting, altering, or restoring a body part.
3. Deconstructing the Procedure: What is Lysis of Adhesions?
To code a procedure correctly, one must first understand it clinically. Lysis of adhesions, or adhesiolysis, is not a single, monolithic action but a targeted intervention.
The Pathophysiology of Adhesions
Adhesions are fibrous bands of scar tissue that form between anatomical structures that are normally separate. They are the body’s natural response to injury, most commonly from:
-
Previous Surgery: The leading cause. The handling of tissues, exposure to air, and the healing process can trigger adhesion formation. Common culprits include hysterectomies, colectomies, and appendectomies.
-
Infection: Pelvic inflammatory disease (PID) or peritonitis can cause widespread inflammation and subsequent adhesions.
-
Inflammation: Conditions like Crohn’s disease or diverticulitis can lead to adhesions.
-
Radiation Therapy: Can cause tissue damage and fibrosis.
-
Trauma: Blunt or penetrating trauma can initiate the healing process that results in adhesions.
These bands can be thin and filmy or thick, dense, and vascular. They can cause problems by constricting, compressing, or tethering structures like the small intestine, fallopian tubes, or tendons, leading to a range of complications.
Clinical Indications for Lysis
A surgeon performs lysis of adhesions to relieve the complications caused by these bands. Common indications include:
-
Small Bowel Obstruction (SBO): Adhesions are the most common cause of SBO. The bands can kink, twist, or compress loops of bowel, preventing the passage of contents.
-
Chronic Abdominal or Pelvic Pain: Adhesions can pull on sensitive structures, causing significant pain.
-
Infertility: In women, adhesions around the fallopian tubes or ovaries can prevent the egg and sperm from meeting.
-
Restricted Joint Movement: Adhesions within a joint capsule (e.g., frozen shoulder) can severely limit range of motion.
4. The Heart of the Matter: Identifying the Correct Root Operation
The most critical step in coding a lysis of adhesions is identifying the correct root operation. This is where the core intent of the procedure is captured. For adhesiolysis, three root operations are primarily relevant: Release, Division, and Destruction.
Root Operation: Release (0N9)
-
Official Definition: “Freeing a body part from an abnormal physical constraint by cutting the use of sharp dissection, blunt dissection, or any combination of the two. The body part being freed may be an organ, a tube (e.g., fallopian tube), the spinal cord, or a nerve. The constraint may be an adhesion, a ligament, a tendon, a scar tissue, or a bone.”
-
When to Use It: This is the most commonly used root operation for lysis of adhesions. It is applied when the sole purpose of cutting the adhesion is to free a body part from the constraint it was causing. The adhesion itself is not the target for removal or destruction; it is the obstacle being overcome to liberate the underlying organ, tube, or nerve.
-
Key Concept: The focus is on freeing the body part, not on eliminating the adhesion. The adhesion is the “abnormal physical constraint.”
Root Operation: Division (0N8)
-
Official Definition: “Cutting into a body part without draining fluids and/or gases from the body part in order to separate or transect a body part.”
-
When to Use It: This root operation is used when the adhesion itself is being cut, and the act of cutting is the entire goal. The code reflects the severing of the fibrous band. This is less common than “Release” but may be appropriate in specific contexts, such as dividing a single, well-defined adhesion that is not primarily constricting another structure but is being transected as a standalone procedure.
Root Operation: Destruction (0N5)
-
Official Definition: “Physical eradication of all or a portion of a body part by the direct use of energy, force, or a destructive agent. None of the body part is physically taken out.”
-
When to Use It: This is used if the adhesion is eradicated using a method like laser ablation, cautery, or a chemical agent. The key differentiator from Release or Division is the method: Destruction implies the tissue is not just cut but is broken down and eradicated in situ. If an adhesion is cut with scissors (sharp dissection), it is not destruction. If it is vaporized with a laser, it is destruction.
A Comparative Analysis
The following table clarifies the distinctions between these three root operations in the context of adhesiolysis.
Root Operations for Lysis of Adhesions
| Root Operation | Code Range | Objective | Method Example | Clinical Scenario Example |
|---|---|---|---|---|
| Release | 0N9 | To free a body part from an abnormal physical constraint (the adhesion). | Sharp dissection with Metzenbaum scissors, blunt dissection with a finger. | Freeing a loop of small intestine that is kinked and obstructed by an adhesion. |
| Division | 0N8 | To cut into/transect the adhesion itself. | Cutting a single band with a scalpel. | Dividing a filmy adhesion between the abdominal wall and omentum during a scheduled procedure where it was an incidental finding. |
| Destruction | 0N5 | To eradicate the adhesion tissue in place. | Laser ablation, fulguration with electrocautery. | Vaporizing endometrial adhesions (Asherman’s syndrome) inside the uterine cavity using a hysteroscopic laser. |
5. Mapping the Anatomy: The Body System and Body Part Characters
Once the root operation is determined, the next critical step is identifying the correct Body System (2nd character) and Body Part (4th character). This is where the anatomical location of the adhesion is crucial. The coder must rely heavily on the operative report to answer: Where was the adhesion located, and what structure was it constraining?
Navigating the Lower Joints System
For adhesions within a joint, the body system is Lower Joints (N). The body part character specifies the joint.
-
Example: Lysis of adhesions in the right knee joint.
-
Body System: Lower Joints (N)
-
Body Part: Knee Joint, Right (G)
-
Navigating the Anatomical Regions, General System
This is a frequently used system for abdominal and pelvic adhesiolysis. The body system is Anatomical Regions, General (Y). The body part character describes a region, not a specific organ.
-
Example: Lysis of adhesions constricting a loop of small intestine in the peritoneal cavity.
-
Body System: Anatomical Regions, General (Y)
-
Body Part: Peritoneal Cavity (W)
-
-
Example: Lysis of adhesions involving the urinary bladder.
-
Body System: Anatomical Regions, General (Y)
-
Body Part: Urinary Bladder (R)
-
Navigating Other Body Systems
Adhesions can form in many locations, requiring coders to be familiar with various body systems.
-
Pleural Cavity: For adhesions between the lung and chest wall, the body system is Respiratory System (B) and the body part is Pleura (9).
-
Uterus (for Asherman’s Syndrome): The body system is Female Reproductive System (U) and the body part is Endometrium (G).
-
Pericardium: The body system is Heart and Great Vessels (2) and the body part is Pericardium (K).
-
Spinal Cord/Nerves: The body system is Central Nervous System (0) or Peripheral Nervous System (1).
6. The Surgical Approach: From Open to Percutaneous
The fifth character defines the Approach, describing how the surgeon reached the operative site. Accurate assignment reflects the invasiveness of the procedure.
Character 5: The Approach
-
Open (0): The site is exposed via a large incision (e.g., a midline laparotomy).
-
Percutaneous (3): The site is reached via a needle-puncture of the skin.
-
Percutaneous Endoscopic (4): A hybrid approach using percutaneous access with endoscopic visualization.
-
Via Natural or Artificial Opening (7): The site is reached through a natural opening like the mouth or vagina.
-
Via Natural or Artificial Opening Endoscopic (8): The site is reached through a natural opening with the use of an endoscope (e.g., hysteroscopy, cystoscopy).
-
External (X): Procedures performed directly on the skin or outside the body. Not typically used for adhesiolysis.
Clinical Scenarios and Code Selection
Let’s combine our knowledge to build a complete code.
Scenario: A patient presents with a small bowel obstruction. The surgeon performs a laparoscopic procedure, identifies dense adhesions between loops of small bowel, and uses sharp dissection to lyse them, freeing the obstructed bowel.
-
Section: Medical and Surgical (0)
-
Body System: The adhesion is in the abdominal cavity, constricting the intestine. We use Anatomical Regions, General (Y).
-
Root Operation: The goal was to free the small bowel from the constraint. This is Release (N9).
-
Body Part: The adhesion was within the peritoneal cavity. Peritoneal Cavity (W).
-
Approach: The procedure was done laparoscopically. Percutaneous Endoscopic (4).
-
Device: No device was left. No Device (Z).
-
Qualifier: No qualifier is needed. No Qualifier (Z).
Final ICD-10-PCS Code: 0N9W4ZZ – Release of Peritoneal Cavity, Percutaneous Endoscopic Approach.
7. Advanced Coding Scenarios: Beyond the Simple Case
Real-world coding is rarely straightforward. Here are some complex scenarios and how to navigate them.
Lysis of Adhesions as a Conjoined Procedure
Often, adhesiolysis is not the primary procedure but is necessary to gain access to the primary surgical site. According to ICD-10-PCS guidelines, if a procedure is performed to accomplish the approach to the primary procedure, it is not coded separately.
-
Example: A surgeon plans a cholecystectomy. Upon entering the abdomen laparoscopically, they encounter adhesions from a prior surgery tethering the liver to the abdominal wall. They lyse these adhesions to visualize the gallbladder and perform the cholecystectomy.
-
Coding Decision: The lysis of adhesions was integral to the surgical approach. Only the cholecystectomy is coded.
Conversely, if the adhesiolysis is performed for a different purpose after the approach has been established, it should be coded separately.
-
Example: The surgeon performs the planned cholecystectomy. After removing the gallbladder, they notice a separate loop of small bowel that is obstructed by an adhesion unrelated to the surgical field. They then lyse that adhesion.
-
Coding Decision: The lysis of this obstructive adhesion is a separate, distinct procedure and should be coded in addition to the cholecystectomy.
Multiple Adhesiolysis in a Single Session
If multiple adhesions are lysed in the same anatomical region (e.g., several bands in the peritoneal cavity), only one code is assigned. If adhesions are lysed in distinctly different anatomical regions, multiple codes may be necessary (e.g., lysing adhesions in the peritoneal cavity and also in the pelvic cavity around the uterus).
Recurrent Adhesions and Repeat Procedures
The coding is the same whether it is the first or tenth time a patient has undergone adhesiolysis. The code reflects the procedure performed at that specific encounter.
8. Practical Application: Code Building with Real-World Cases
Let’s solidify our knowledge with detailed case studies.
Case Study 1: Laparoscopic Lysis of Small Bowel Adhesions
-
Op Report Excerpt: “The patient was taken to the OR for acute small bowel obstruction. A 12-mm trocar was placed infraumbilically and the abdomen was insufflated. Dense adhesions were noted between a loop of ileum and the anterior abdominal wall, causing a sharp angulation and obstruction. Using a combination of blunt and sharp dissection through additional trocars, the adhesions were meticulously lysed, completely freeing the involved segment of bowel. The bowel was noted to be viable.”
-
Code Building:
-
Section: 0 (Medical and Surgical)
-
Body System: Y (Anatomical Regions, General) – The adhesion was in the abdominal cavity.
-
Root Operation: N9 (Release) – The goal was to free the small bowel.
-
Body Part: W (Peritoneal Cavity) – This is the general body part for abdominal adhesions.
-
Approach: 4 (Percutaneous Endoscopic) – Laparoscopic.
-
Device: Z (No Device)
-
Qualifier: Z (No Qualifier)
-
-
Final Code: 0N9W4ZZ
Case Study 2: Open Lysis of Knee Joint Adhesions (Arthrolysis)
-
Op Report Excerpt: “The patient with a history of remote knee trauma and progressive stiffness underwent an open arthrolysis of the right knee. A medial parapatellar incision was made. The joint was entered, and extensive fibrotic adhesions within the suprapatellar pouch and medial gutter were identified. These were sharply released, resulting in an immediate improvement in knee flexion and extension.”
-
Code Building:
-
Section: 0 (Medical and Surgical)
-
Body System: N (Lower Joints)
-
Root Operation: N9 (Release) – Freeing the knee joint from the constraint.
-
Body Part: G (Knee Joint, Right)
-
Approach: 0 (Open)
-
Device: Z (No Device)
-
Qualifier: Z (No Qualifier)
-
-
Final Code: 0N9G0ZZ
Case Study 3: Lysis of Pleural Adhesions via Thoracoscopy
-
Op Report Excerpt: “A video-assisted thoracoscopic surgery (VATS) was performed for a persistent pneumothorax. Upon entering the pleural space, numerous dense, vascular adhesions between the visceral and parietal pleura were encountered. These were carefully divided using electrocautery to allow for lung re-expansion.”
-
Code Building:
-
Section: 0 (Medical and Surgical)
-
Body System: B (Respiratory System)
-
Root Operation: N9 (Release) or N8 (Division)? The report says “divided,” but the objective was to free the lung to allow re-expansion. Release (N9) is more appropriate.
-
Body Part: 9 (Pleura)
-
Approach: 4 (Percutaneous Endoscopic) – VATS.
-
Device: Z (No Device)
-
Qualifier: Z (No Qualifier)
-
-
Final Code: 0N994ZZ
9. Common Pitfalls and How to Avoid Them
-
Misidentifying the Body System: Coding a peritoneal adhesion under the Gastrointestinal system instead of Anatomical Regions, General. Solution: Focus on the location of the adhesion, not the organ it’s attached to. If it’s in a cavity or space, Anatomical Regions is often correct.
-
Confusing Root Operations: Using “Division” when “Release” is more accurate. Solution: Always ask: “Was the goal to cut a band (Division) or to free a constrained organ (Release)?” Release is far more common.
-
Documentation Deficiencies: The op report simply states “lysis of adhesions” without specifying location or method. Solution: Query the physician. A query is essential for accurate coding. Ask: “Where were the adhesions located? What structure was being constrained? What was the surgical approach?”
10. The Importance of Precision: Compliance and Reimbursement
Inaccurate coding for lysis of adhesions has direct consequences. An under-coded procedure (e.g., missing a separate adhesiolysis) leads to lost revenue. An over-coded procedure (e.g., coding an approach adhesiolysis separately) is a compliance risk and can be construed as fraud. Furthermore, accurate data is critical for tracking the incidence of adhesion-related complications, evaluating surgical outcomes, and driving research into prevention. Every correctly assigned code contributes to the integrity of healthcare data.
11. Conclusion
Mastering the ICD-10-PCS coding for lysis of adhesions requires a methodical approach: a deep understanding of the root operations of Release, Division, and Destruction; precise identification of the affected body system and part; and a careful analysis of the surgical approach and intent as documented in the operative report. By moving beyond rote memorization and embracing the logic of the PCS system, coders can ensure accuracy, support compliance, and capture the full clinical picture of this common but complex surgical intervention.
12. Frequently Asked Questions (FAQs)
Q1: What is the default root operation if the operative report just says “lysis of adhesions” without further detail?
A1: There is no default. The coder must query the physician for clarification. However, “Release” (0N9) is the most frequently applicable root operation, as the intent is typically to free a constrained organ.
Q2: How do I code a lysis of adhesions that is performed using a robot (e.g., robotic-assisted laparoscopy)?
A2: The approach for robotic-assisted procedures is classified based on the instrumentation used. If the procedure is performed through multiple small incisions with robotic arms, it is coded as Percutaneous Endoscopic (4). The robotic technology is considered the method of performing a percutaneous endoscopic procedure.
Q3: Can I code multiple lysis of adhesions codes for one surgical session?
A3: Yes, but only if the procedures are performed in distinctly different anatomical body parts that fall under different body systems or have unique body part values. For example, lysing adhesions in the peritoneal cavity (0N9W4ZZ) and also performing a hysteroscopic lysis of intrauterine adhesions (0U9G8ZZ) would require two codes. Multiple bands lysed in the same general area (e.g., the peritoneal cavity) are coded only once.
Q4: What is the code for a laparoscopic lysis of pelvic adhesions involving the fallopian tubes (for infertility)?
A4: This would be coded to the body part that is being freed. If the fallopian tube is being freed, the code would be in the Female Reproductive System.
* Section: 0
* Body System: U (Female Reproductive System)
* Root Operation: N9 (Release)
* Body Part: Fallopian Tube, specify left (6) or right (7) or bilateral (see guidelines).
* Approach: 4 (Percutaneous Endoscopic)
* Device: Z
* Qualifier: Z
* Example Code (Right): 0U9N4ZZ
Date: November 19, 2025
Author: Healthcare Coding Insights
Disclaimer: This article is intended for educational purposes and to illustrate expert-level medical coding principles. It is not a substitute for the official ICD-10-PCS guidelines, code books, or professional coding advice. Medical coders must use the current year’s official resources and adhere to facility-specific protocols when assigning codes.





