In the high-stakes theater of cardiac surgery, few procedures are as complex and transformative as the replacement of the mitral valve. This intricate operation addresses life-threatening dysfunctions—stenosis, regurgitation, endocarditis—restoring hemodynamic stability and quality of life. Yet, for every physical procedure performed in the operating room, a parallel, equally critical process unfolds in the domain of health information management: the precise and accurate translation of that procedure into an alphanumeric code. This is the world of ICD-10-PCS (Procedure Coding System), where clinical complexity meets administrative necessity.
The ICD-10-PCS code for a mitral valve replacement is not merely a billing artifact; it is a multi-dimensional data point that drives reimbursement, informs public health statistics, fuels clinical research, and impacts hospital quality metrics. A single misplaced character can shift the narrative of a patient’s record, misrepresent resource utilization, and trigger significant financial and compliance repercussions. This article delves deep into the granular details of constructing the ICD-10-PCS code for mitral valve replacement, moving beyond basic code look-ups to explore the anatomy, surgical techniques, device technology, and documentation nuances that underpin each of the seven characters. Designed for medical coders, coding students, clinical documentation integrity (CDI) specialists, and healthcare administrators, this exhaustive guide aims to equip you with the knowledge to navigate this challenging terrain with confidence and precision.
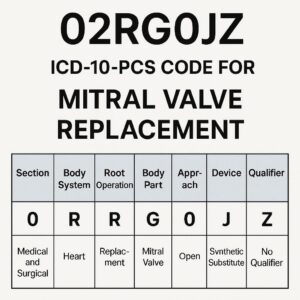
ICD-10-PCS Code for Mitral Valve Replacement
Section 1: Foundational Anatomy and Clinical Indications for Mitral Valve Replacement
Anatomy of the Mitral Apparatus: To code accurately, one must first understand what is being coded. The mitral valve is a complex, bileaflet structure located between the left atrium and left ventricle. It is more accurately termed the mitral apparatus, consisting of:
-
Anterior and Posterior Leaflets: Thin but strong flaps of tissue that open to allow blood flow into the ventricle and close to prevent backflow.
-
Chordae Tendineae: Tendon-like cords that tether the leaflet edges to the papillary muscles, preventing prolapse.
-
Papillary Muscles: Specialized muscles within the left ventricle that contract to tighten the chordae.
-
Mitral Annulus: A fibrous ring that forms the structural base for the valve leaflets.
Primary Indications for Replacement (When Repair is Not Feasible):
-
Rheumatic Mitral Stenosis: Thickened, fused leaflets from rheumatic fever, often calcified.
-
Severe Mitral Regurgitation: Due to myxomatous degeneration (e.g., Barlow’s disease, flail leaflet), ischemic cardiomyopathy (papillary muscle dysfunction), or endocarditis with destructive vegetation.
-
Failed Previous Repair: When a prior surgical or percutaneous mitral valve repair breaks down.
-
Calcific Degeneration: Severe annular or leaflet calcification that makes the valve immobile and irreparable.
Section 2: Deconstructing ICD-10-PCS: The Framework of a Seven-Character Code
ICD-10-PCS is a procedural taxonomy built on a consistent, multi-axial structure. Each of the seven characters represents a specific aspect of the procedure, offering an astonishing degree of specificity. For the Medical and Surgical section (the first character 0), the framework is:
Character 1: Section (0) – Medical and Surgical
Character 2: Body System (2) – Heart and Great Vessels
Character 3: Root Operation – The objective of the procedure (See Section 3)
Character 4: Body Part – The specific site (See Section 4)
Character 5: Approach – How the site was accessed (See Section 5)
Character 6: Device – What was put in (See Section 6)
Character 7: Qualifier – Additional information (See Section 7)
The general code structure for a mitral valve replacement begins with 02R. This article will dissect each subsequent character choice.
Section 3: The Root Operation – What is Truly Being Done? (Replacement vs. Supplement)
The root operation is the cornerstone of the code. For valve replacement, the definition is clear-cut:
-
Root Operation R: REPLACEMENT – “Putting in or on biological or synthetic material that physically takes the place and/or function of all or a portion of a body part.”
-
Key Concept: The native body part (the diseased mitral valve) is excised and removed. Its function is then assumed by the implanted prosthetic device. This is a complete substitution.
-
Critical Distinction from Root Operation U: SUPPLEMENT
-
Supplement means “putting in or on biological or synthetic material that physically reinforces and/or augments the function of a portion of a body part.” This is not a replacement.
-
Clinical Example: A mitral valve annuloplasty, where a supportive ring (device) is sewn around the native valve annulus to improve its function, but the native leaflets are retained. This would be coded to
02UG(Supplement Mitral Valve with Synthetic Substitute, Open).
Coding Rule: If the native valve is excised and removed, it is Replacement. If the native valve is repaired, supported, or altered but remains in place, it is likely Supplement or another root operation like Repair (Q) or Restriction (V).
Section 4: Character 4: The Body Part – Pinpointing the Mitral Valve
Within the Heart and Great Vessels system, the mitral valve has a specific identifier. However, the coder must be vigilant for concurrent procedures.
-
Character 4:
G– Mitral Valve – This is the standard, straightforward body part for an isolated mitral valve replacement. -
Complexity with Multiple Valves: A critical decision point arises when more than one valve is replaced during the same operative episode.
-
Separate Procedures: If the aortic and mitral valves are both replaced via the same sternotomy, you would code two separate procedures:
02RG(Mitral Valve Replacement) and02RF(Aortic Valve Replacement). -
Combined Device: There is no single ICD-10-PCS code for a “double valve replacement.” Each valve is coded individually.
-
-
Consideration for Subvalvular Apparatus: The official coding guidelines do not provide a unique body part for the chordae or papillary muscles in this context. When the entire mitral apparatus is replaced, it is still coded to the mitral valve (
G).
Section 5: Character 5: The Surgical Approach – From Open Sternotomy to Percutaneous
The approach describes the technique used to reach the operative site. Technological advances have significantly expanded the options for mitral valve therapy.
| Approach Character | Approach Name | Description | Typical Use in MVR |
|---|---|---|---|
| 0 | Open | Cutting through the skin, tissues, and sternum to directly visualize the heart. | Traditional, full sternotomy. |
| 3 | Percutaneous | Access via needle puncture of the skin, using catheters and imaging guidance without direct visualization. | Transcatheter Mitral Valve Implantation (TMVI) or Valve-in-Valve procedures. |
| 4 | Percutaneous Endoscopic | Percutaneous access with the use of an endoscope for visualization. | Less common for MVR; more for diagnostics or辅助. |
| 7 | Via Natural or Artificial Opening | Entry via a natural orifice (e.g., mouth, urethra). | Not applicable for mitral valve procedures. |
| 8 | Via Natural/Artificial Opening Endoscopic | As above, but with an endoscope. | Not applicable for mitral valve procedures. |
Key Decision: The most common are 0 (Open) for surgical MVR and 3 (Percutaneous) for TMVI. The documentation must clearly state the technique: “median sternotomy,” “open chest,” or “transcatheter,” “transseptal puncture,” “transapical access.”
Section 6: Character 6: The Device – The Heart of the Code
This character defines the prosthetic valve implanted. The choice is critical and entirely dependent on the operative report’s specification.
-
Character 6:
0– Synthetic Substitute: This is the mechanical valve. Made of carbon and titanium, it is extremely durable but requires lifelong anticoagulation (e.g., warfarin). Brands include St. Jude Medical, On-X, Medtronic Hall. -
Character 6:
2– Zooplastic Tissue: This is a tissue valve from an animal, most commonly a porcine (pig) valve or a bovine (cow) pericardial valve. These do not require long-term anticoagulation but have a limited lifespan (~10-15 years). -
Character 6:
3– Autologous Tissue Substitute: Rarely used for MVR. This would involve using the patient’s own tissue (e.g., a pulmonary autograft “Ross Procedure,” which is more common for aortic valve replacement). -
**Character 6:
4– Tissue Engineered Substitute (Future-focused): For experimental or next-generation bio-engineered valves. Not commonly in use as of 2025.
Coding Clinic Guidance: The AHA’s Coding Clinic has reinforced that the distinction between “zooplastic” and other biological materials must come from the documentation. If the report states “bioprosthetic valve,” “tissue valve,” or specifically “porcine” or “bovine pericardial,” code to 2.
Section 7: Character 7: The Qualifier – Laterality and Specificity
The mitral valve is inherently a single, midline structure. Therefore, there is no laterality qualifier (no left/right).
-
Character 7:
Z– No Qualifier: This is the default and almost universally used character for a standard mitral valve replacement. -
Other Qualifiers: In the
02Rtable, other qualifiers likeJ(Synthetic Substitute, Resurfacing) are not applicable to valve replacement. Always default toZunless future PCS updates introduce new qualifiers for specific technologies.
Section 8: Building the Complete Code: Practical Case Scenarios
Let’s apply our knowledge to build complete, valid codes.
Scenario 1: Traditional Surgical MVR
-
Op Note Excerpt: “Via standard median sternotomy, the patient was placed on cardiopulmonary bypass. The diseased mitral valve was sharply excised. A 29-mm On-X mechanical prosthetic valve was implanted with interrupted sutures.”
-
Code Construction:
-
Section: 0 (Medical/Surgical)
-
Body System: 2 (Heart/Great Vessels)
-
Root Operation: R (Replacement)
-
Body Part: G (Mitral Valve)
-
Approach: 0 (Open)
-
Device: 0 (Synthetic Substitute – Mechanical)
-
Qualifier: Z (No Qualifier)
-
-
Final ICD-10-PCS Code:
02RG0JZ
Scenario 2: Transcatheter Mitral Valve Implantation (TMVI)
-
Op Note Excerpt: “Under fluoroscopic and TEE guidance, a catheter was advanced percutaneously via the femoral vein, across the interatrial septum. A 31-mm Edwards SAPIEN 3 valve (bovine pericardial) was deployed within the native mitral annular position.”
-
Code Construction:
-
Char 1-4: 02RG (Replacement of Mitral Valve)
-
Approach: 3 (Percutaneous)
-
Device: 2 (Zooplastic Tissue – Bovine Pericardial)
-
Qualifier: Z
-
-
Final ICD-10-PCS Code:
02RG32Z
Scenario 3: Mitral and Aortic Valve Replacement (Double Valve)
-
Op Note Excerpt: “Through a median sternotomy, on cardiopulmonary bypass, we excised the stenotic aortic valve and replaced it with a 23-mm Magna Ease pericardial valve. We then excised the regurgitant mitral valve and replaced it with a 27-mm St. Jude Mechanical valve.”
-
Code Construction:
-
Procedure 1 – Aortic Valve:
02RF0JZ(Replacement of Aortic Valve with Synthetic Substitute, Open) -
Procedure 2 – Mitral Valve:
02RG0JZ(Replacement of Mitral Valve with Synthetic Substitute, Open)
-
-
Two separate codes are required.
Section 9: Common Documentation Pitfalls and CDI Opportunities
Ambiguous documentation is the primary source of coding errors and queries.
-
“Valve was replaced with a bioprosthesis.”
-
Pitfall: “Bioprosthesis” is often used generically. Is it zooplastic (animal) or synthetic (mechanical)?
-
CDI Opportunity: Query for clarification: “Can you specify the type of bioprosthetic valve implanted: mechanical (e.g., On-X) or tissue (e.g., porcine, bovine)?”
-
-
“Minimally invasive MVR performed.”
-
Pitfall: “Minimally invasive” is a clinical term, not a PCS approach. It could mean a mini-thoracotomy (still coded Open
0) or a fully percutaneous (3) procedure. -
CDI Opportunity: Query: “Please specify the surgical approach: full sternotomy, mini-thoracotomy, or percutaneous/transcatheter?”
-
-
Lack of Specification in Re-Do Operations: A “valve-in-valve” transcatheter procedure inside a failing bioprosthesis is a replacement (
02RG3...), not a revision. Documentation must state the prior valve is being “replaced.”
Section 10: The Role of Imaging and Technology
The operative report is the gold standard, but supporting documents are invaluable.
-
Intraoperative Transesophageal Echocardiogram (TEE) Reports: Confirm valve pathology, measurements, and immediate post-implant function.
-
Device/Implant Records: The specific manufacturer and model name/number are often recorded separately and can definitively identify a device as mechanical or tissue.
-
Anesthesia Records: Can corroborate the approach (e.g., “positioned for sternotomy” vs. “prepped for percutaneous access”).
Section 11: Compliance, Auditing, and Future Directions
Coding accuracy is a compliance imperative. Auditors will verify:
-
Medical necessity linking the ICD-10-CM diagnosis code (e.g.,
I05.0Rheumatic mitral stenosis) to the procedure. -
One-to-one device correlation: The code’s device character must match the implant record exactly.
-
Unbundling: Ensuring separate codes for the valve replacement and any concomitant procedures (e.g., CABG, atrial ablation) are supported.
The Future: The field is evolving towards transcatheter solutions and sutureless valves. ICD-10-PCS will likely require new device characters or qualifiers to keep pace. Staying current with Coding Clinic and PCS updates is essential.
Conclusion
Accurate ICD-10-PCS coding for mitral valve replacement demands a synthesis of anatomical knowledge, surgical understanding, and meticulous attention to documentation detail. From distinguishing a root operation to identifying a device, each character builds a precise narrative of the patient’s intervention. By mastering this seven-character lexicon, healthcare professionals ensure data integrity, support optimal patient care analysis, and uphold the financial and compliance pillars of modern medicine. The code 02RG0JZ is far more than a sequence of characters; it is the digital signature of a life-altering cardiac procedure.
Frequently Asked Questions (FAQs)
Q1: What is the code for a minimally invasive robotic mitral valve replacement?
A: Robotic-assisted surgery is still considered an Open approach (0) in PCS, as it involves cutting through tissue layers to establish portals. The robotic aspect is not currently separately qualifiable. The code would be 02RG0JZ or 02RG02Z based on the device, with the approach 0.
Q2: How do I code a mitral valve replacement with a homograft (human donor valve)?
A: A human tissue valve (homograft/allograft) is classified under Zooplastic Tissue (Character 2). The code would be 02RG02Z for an open procedure.
Q3: What if the operative report only says “prosthetic valve” without specifying mechanical or tissue?
A: This is incomplete documentation. You must query the physician for clarification. It is not appropriate to assume or default to one type. A generic code does not exist.
Q4: Is there a code for a mitral valve “valve-in-ring” procedure?
A: A transcatheter valve placed inside a previously implanted annuloplasty ring is still a replacement of the native mitral valve function. You would code 02RG32Z (if using a tissue valve percutaneously). The existing ring is not the body part being replaced; the mitral valve apparatus is.
Q5: How do I handle coding for a patient undergoing a TMVI who requires conversion to an open MVR in the same operation?
A: Code only the procedure that was completed. If the percutaneous attempt was aborted and an open MVR was performed, you code only the open MVR (02RG0JZ/02RG02Z). The attempted percutaneous approach is not coded.
Additional Resources & References
-
Official ICD-10-PCS Coding Guidelines: Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). www.cms.gov
-
AHA Coding Clinic for ICD-10-CM/PCS: The authoritative source for official coding advice and quarterly updates. American Hospital Association.
-
The Society of Thoracic Surgeons (STS) National Database: Provides clinical definitions and benchmarks for cardiac surgery procedures. www.sts.org
-
American College of Cardiology (ACC): Clinical guidelines on valvular heart disease management, informing medical necessity. www.acc.org
-
Textbook: *Cardiothoracic Surgical Coding: A Complete Guide to ICD-10-PCS and CPT*, by Mary L. Brandt, MD, et al. A comprehensive resource for complex cardiothoracic coding scenarios.
Date: December 3, 2025
Author: The Healthcare Coding Institute
Disclaimer: This article is for educational and informational purposes only. It is not a substitute for official coding guidelines, payer-specific policies, or professional medical advice. Always consult the most current ICD-10-PMS manuals, AHA Coding Clinic, and physician documentation for final coding determinations.





