In the dynamic landscape of modern healthcare, few areas are as clinically intense and administratively complex as the management of acute respiratory failure. Within this domain, Bilevel Positive Airway Pressure (BiPAP) has emerged as a cornerstone non-invasive therapy, a vital bridge that can prevent a patient from crossing the precarious threshold into invasive mechanical ventilation. For the healthcare professional, its whirring hum is a sound of hope; for the clinical documentation specialist and medical coder, it represents a critical data point that carries significant financial and quality implications. The assignment of a diagnosis-related group (DRG), the accuracy of quality reporting, and the very financial stability of a healthcare institution can hinge on the precise translation of a patient’s respiratory journey into the alphanumeric language of ICD-10-PCS.
This article delves deep into one of the most specific and consequential directives within this coding system: the assignment of the ICD-10-PCS code for BiPAP ventilation when its application extends beyond 48 hours. This is not merely an arbitrary time limit; it is a codified distinction that reflects a sustained, intensive level of care. Coding it correctly is not just a matter of clerical accuracy—it is an act of clinical fidelity. A misunderstanding or misapplication can lead to underpayment, audit flags, and a distorted picture of patient acuity. Through this exhaustive exploration, we will dissect the official guidelines, unravel complex clinical scenarios, and provide a robust framework for ensuring that your coding practices are as precise and reliable as the life-supporting technology they represent. Prepare for a journey into the heart of respiratory care coding, where every hour counts and every character in a code tells a story.
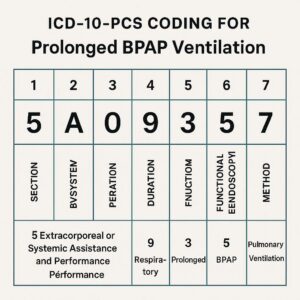
ICD-10-PCS Coding for Prolonged BiPAP Ventilation
2. Understanding the Basics: What is BiPAP and When is it Used?
Before a single code can be assigned, a fundamental understanding of the therapy itself is paramount. BiPAP, a brand name that has become a generic term (much like “Kleenex” for tissues), stands for Bilevel Positive Airway Pressure. It is a specific form of non-invasive ventilation (NIV) delivered through a tightly fitted mask that covers the nose, mouth, or both.
The core mechanic of BiPAP is its delivery of two distinct levels of positive air pressure:
-
Inspiratory Positive Airway Pressure (IPAP): A higher pressure level that supports the patient’s inhalation, actively assisting the work of breathing by “blowing” air into the lungs. This helps overcome airway resistance and improves tidal volume (the amount of air moved with each breath).
-
Expiratory Positive Airway Pressure (EPAP): A lower pressure level that maintains during exhalation. This pressure keeps the alveoli (the tiny air sacs in the lungs) from collapsing at the end of a breath, improving oxygenation by maintaining functional residual capacity (FRC).
The clinical beauty of BiPAP lies in this duality. It simultaneously assists ventilation (by supporting inhalation with IPAP) and improves oxygenation (by preventing alveolar collapse with EPAP). This makes it exceptionally effective for certain types of respiratory failure, particularly:
-
Acute Hypercapnic Respiratory Failure: Characterized by a buildup of carbon dioxide (CO2) in the blood. This is common in exacerbations of Chronic Obstructive Pulmonary Disease (COPD). The IPAP support does the work the fatigued diaphragm and respiratory muscles cannot, effectively “blowing off” the excess CO2.
-
Hypoxemic Respiratory Failure: Characterized by critically low oxygen levels in the blood. While its effect is more pronounced on CO2 clearance, the EPAP component of BiPAP can help recruit collapsed alveoli, thereby improving oxygenation in conditions like pneumonia or cardiogenic pulmonary edema.
-
Post-Extubation Support: Used to prevent re-intubation in patients who have been successfully weaned from a mechanical ventilator but still require some respiratory support.
-
Neuromuscular Weakness: For patients with conditions like Amyotrophic Lateral Sclerosis (ALS) or Myasthenia Gravis, where the respiratory muscles are weak, BiPAP provides the necessary muscle assistance to maintain adequate ventilation, especially during sleep.
Distinguishing BiPAP from its close relative, CPAP (Continuous Positive Airway Pressure), is crucial. CPAP delivers a single, constant pressure throughout the breathing cycle. It is excellent for maintaining an open airway (as in obstructive sleep apnea) and improving oxygenation but provides no active assistance for inhalation. BiPAP is the more advanced therapy, reserved for sicker patients whose own respiratory drive and muscle strength are insufficient.
3. The Foundation: Navigating the ICD-10-PCS Alphabet for Respiratory Support
The ICD-10-PCS system is built on a logical, multi-axial structure. Each character in a seven-character code represents a specific piece of information about the procedure. For procedures related to the Administration Section, which is where respiratory assistance is coded, the structure is as follows:
-
Section (1st Character): 3 – Administration
-
Body System (2nd Character): E – Physiological Systems and Anatomical Regions
-
Root Operation (3rd Character): This is the most critical character for our discussion. It defines the objective of the procedure.
-
Body Part/Region (4th Character): Specifies the anatomical area where the substance is introduced or the function is performed.
-
Approach (5th Character): Describes the technique used to reach the procedure site.
-
Substance/Device (6th Character): Identifies the substance being administered or the device being used.
-
Qualifier (7th Character): Provides additional information about the procedure.
For respiratory support, we are concerned with two primary Root Operations within the Administration Section:
-
Introduction (3rd Character = 0): This root operation is defined as “Putting in or on a therapeutic, diagnostic, nutritional, physiological, or prophylactic substance except blood or blood products.” In the context of respiratory care, this is used for intermittent treatments. Examples include:
-
A single nebulizer treatment with albuterol.
-
Incentive spirometry.
-
Intermittent positive pressure breathing (IPPB).
-
-
Performance (3rd Character = 1): This is the root operation for BiPAP. It is defined as “Carrying out or accomplishing a function.” The Official Coding Guidelines for ICD-10-PCS explicitly state: “The Performance root operation is used to identify the continuous assistance of a physiological function.” This is the key distinction. BiPAP is not a substance being introduced; it is a device that is continuously performing or assisting the physiological function of breathing.
The table below provides a clear comparison of these two root operations in the context of respiratory care.
ICD-10-PCS Root Operations for Respiratory Therapy Procedures
| Feature | Root Operation: Introduction (0) | Root Operation: Performance (1) |
|---|---|---|
| Definition | Putting in or on a substance. | Carrying out or accomplishing a function. |
| Clinical Analogy | “Giving a drug” or “applying a treatment.” | “Using a machine to do a body’s job.” |
| Duration | Typically intermittent, discrete sessions. | Continuous assistance. |
| Example Procedures | Nebulizer treatments, inhaled medications. | Mechanical Ventilation, BiPAP, CPAP. |
| ICD-10-PCS Code | Example: 3E0L3GC (Introduction of other gas into respiratory tract, via natural or artificial opening) | 5A09357 (Performance of respiratory ventilation, less than 24 consecutive hours) 5A09457 (Performance of respiratory ventilation, 24-96 consecutive hours) |
Note: The codes in the Performance row are from the New Technology section, which will be explained in the next section.
4. The 48-Hour Threshold: A Pivotal Moment in Coding and Clinical Distinction
Historically, coding for mechanical ventilation and BiPAP was housed in the Medical and Surgical Section, under the root operation “Insertion” of a “tracheostomy device” or “other device.” This was clinically unintuitive. The 2022 ICD-10-PCS update represented a paradigm shift, moving these codes to the New Technology Section (character 1 = 5) to better reflect the nature of the service: the performance of a physiological function.
The New Technology Section uses a similar multi-axial structure but is tailored for tracking emerging procedures and technologies. The codes for respiratory ventilation are now found here, and they incorporate a crucial variable: time.
The current coding options for the Performance of Respiratory Ventilation are:
-
5A09357: Performance of Respiratory Ventilation, Less than 24 Consecutive Hours
-
5A09457: Performance of Respiratory Ventilation, 24-96 Consecutive Hours
-
5A09557: Performance of Respiratory Ventilation, Greater than 96 Consecutive Hours
Here is where the “greater than 48 hours” concept, which is deeply ingrained in coder education, requires careful reconciliation with the current code descriptors. The 48-hour rule was a long-standing guideline from the ICD-10-PCS Official Guidelines for Coding and Reporting, Section X.A.4, which stated that a patient who received “less than 96 hours” of mechanical ventilation could only be assigned a principal diagnosis of respiratory failure if the ventilation lasted for more than 48 hours. This was a DRG and diagnosis sequencing rule, not a PCS code descriptor.
The Critical Reconciliation:
-
For PCS Coding (The Procedure): You must use the actual, consecutive hours of ventilation. If BiPAP is used for 60 consecutive hours, the correct PCS code is 5A09457 (24-96 consecutive hours).
-
For Diagnosis Sequencing (The Reason): The “greater than 48 hours” rule still influences whether respiratory failure can be principal. For that same 60-hour BiPAP case, respiratory failure can be assigned as the principal diagnosis because the ventilation lasted >48 hours.
Therefore, the topic “ICD-10-PCS code BiPAP greater than 48 hours” is a hybrid concept. It points to the use of code 5A09457, but it is triggered by the fact that the duration has crossed the 48-hour threshold, making it a clinically significant event for both procedure coding and diagnosis prioritization. The 48-hour mark is a proxy for a higher level of acuity and resource use.
5. Deconstructing the Code: A Step-by-Step Build of 5A09457
Let us construct the code for BiPAP lasting 72 consecutive hours, piece by piece, to understand its full meaning.
-
1st Character (Section): 5 – New Technology. This indicates the code is part of a set created to track specific technologies, in this case, modern respiratory support.
-
2nd Character (Body System): A – Physiological Systems. The function being performed is physiological (breathing), not a surgical intervention on an anatomical part.
-
3rd Character (Root Operation): 0 – Performance. This confirms the procedure is the “carrying out of a physiological function,” which is breathing.
-
4th Character (Body System): 9 – Respiratory System. This specifies which physiological system is being assisted.
-
5th Character (Duration): 4 – 24-96 Consecutive Hours. This is the character that captures the prolonged nature of the support. For our scenario of 72 hours, this is the correct character. (A ‘5’ would be used for >96 hours).
-
6th Character (Function): 5 – Ventilation. This distinguishes it from other respiratory functions, such as oxygenation (which has its own set of codes for Extracorporeal Membrane Oxygenation – ECMO).
-
7th Character (Qualifier): 7 – Other Equipment. This is the default qualifier for BiPAP and CPAP. It distinguishes it from a standard mechanical ventilator (which would use Qualifier ‘Z’ – No Qualifier).
Thus, the complete code 5A09457 tells the entire story: “Using new technology to perform the physiological function of respiratory ventilation for between 24 and 96 consecutive hours, using other equipment (BiPAP).”
6. Clinical Scenarios and Coding Applications: From the ER to the ICU
Theory is essential, but application is where coding accuracy is proven. Let’s explore several detailed patient scenarios.
Scenario 1: The Straightforward COPD Exacerbation
-
Presentation: A 68-year-old male with severe COPD presents to the ER in acute respiratory distress. Arterial Blood Gas (ABG) shows respiratory acidosis with a pH of 7.25 and elevated PaCO2.
-
Treatment: He is placed on BiPAP in the ICU. The therapy continues uninterrupted for 60 consecutive hours until his ABG normalizes and he is successfully weaned.
-
Coding: 5A09457 is assigned. The duration is 60 hours, which falls squarely within the 24-96 hour range. The principal diagnosis would be acute respiratory failure due to COPD exacerbation, as the BiPAP duration was >48 hours.
Scenario 2: The Interrupted Course – The “Stop-and-Start” Challenge
-
Presentation: A 55-year-old female with congestive heart failure and pneumonia develops hypoxemic respiratory failure.
-
Treatment: She is started on BiPAP on Monday at 10:00 AM. She tolerates weaning trials, and BiPAP is discontinued on Tuesday at 2:00 PM (a 28-hour duration). However, on Wednesday at 4:00 AM, her oxygen saturation drops precipitously, and BiPAP is re-initiated for another 30 hours.
-
Coding: This is a critical test of the “consecutive” rule. The two periods of BiPAP are not added together. The first episode was 28 hours (5A09457). The second, separate episode was 30 hours (5A09457). You would assign the code twice, reflecting two distinct performances of respiratory ventilation. The clock resets with any discontinuation of therapy.
Scenario 3: The Transition from BiPAP to Intubation
-
Presentation: A 70-year-old male with ARDS (Acute Respiratory Distress Syndrome) is managed with BiPAP.
-
Treatment: He is on BiPAP for 36 hours but continues to deteriorate. He is intubated and placed on a mechanical ventilator for the next 5 days.
-
Coding: The 36 hours of BiPAP is coded as 5A09457. The subsequent mechanical ventilation via the endotracheal tube is a separate procedure. Since the mechanical ventilator is now performing the function, and it lasts for 5 days (>96 hours), it is coded as 5A09557. Both codes are assigned. The BiPAP was a trial that failed, and its duration does not contribute to the duration of the invasive ventilation; each has its own “consecutive hours” clock.
7. Navigating Grey Areas: DNR, Comfort Care, and the Question of “Intent”
One of the most challenging areas for coders involves patients with limitations of care.
Scenario: BiPAP for Comfort in a DNR/DNI Patient
-
Situation: An 85-year-old patient with metastatic cancer and a Do-Not-Resuscitate/Do-Not-Intubate (DNR/DNI) order develops pulmonary edema. She is struggling to breathe and is extremely anxious. The medical team initiates BiPAP not with the “curative” intent of reversing the respiratory failure, but with the “palliative” intent of relieving dyspnea and anxiety—to provide comfort.
-
The Coding Question: Is this still coded as 5A09457 if it lasts >48 hours?
-
The Official Guidance: According to the *AHA Coding Clinic for ICD-10-CM/PCS*, the intent of the provider does not change the nature of the procedure. BiPAP is a form of respiratory ventilation regardless of whether the goal is curative or palliative. If the device is performing the physiological function of breathing for the patient for a continuous period, the procedure code must be assigned. The clinical indication (palliative care) would be reflected in the diagnosis codes (e.g., R06.00, Dyspnea; Z51.5, Encounter for palliative care), not by withholding the PCS code. The code represents what was done, not why it was done.
8. The Critical Role of Physician Documentation
The coder is wholly dependent on the medical record. Vague documentation like “patient on BiPAP” is insufficient. The record must clearly support the code assignment.
What Coders Need to See:
-
Clear Start and Stop Times: The exact datetime for initiation and discontinuation of therapy is non-negotiable. This is often found in respiratory therapy flowsheets, nursing notes, and physician progress notes.
-
Duration: A specific statement of total consecutive hours is ideal but rare. The start/stop times must be used to calculate it.
-
Mode of Ventilation: The documentation should explicitly state “BiPAP” and ideally include the settings (e.g., IPAP/EPAP). This distinguishes it from CPAP or high-flow nasal cannula, which are coded differently.
-
Medical Necessity: The reason for BiPAP should be clear, such as “for acute hypercapnic respiratory failure” or “for hypoxemia secondary to pneumonia.”
Clinical Documentation Integrity (CDI) specialists play a vital role here, querying physicians when this information is missing or ambiguous to ensure the record accurately reflects the patient’s high level of acuity.
9. Common Pitfalls and Audit Risks: Ensuring Coding Compliance
Several common errors can lead to denials and audit failures:
-
Averaging Hours: If a patient is on BiPAP for 20 hours one day and 28 the next, but it was continuous, it’s 48 consecutive hours (5A09457). If it was two separate episodes, they are coded separately. Do not average.
-
Confusing BiPAP with High-Flow Nasal Cannula (HFNC): HFNC warms and humidifies high-flow oxygen but does not provide positive pressure ventilation. It is not coded as performance of respiratory ventilation. This is a frequent and costly error.
-
Incorrect Code for CPAP: CPAP, while a positive pressure device, is used for a different purpose (splinting the airway open) and does not actively assist ventilation. It is also coded with 5A09357/5A09457/5A09557, as the performance is still of “respiratory ventilation,” but the clinical context and device are different. The key is that both BiPAP and CPAP represent continuous performance.
-
Missing the “Consecutive” Definition: Any break in therapy, even for 30 minutes for a patient to eat, resets the clock for a new episode.
-
Under-Coding Due to Unclear Records: If the duration cannot be determined from the record, the coder cannot assume it was >24 hours. A query is mandatory.
10. The Future of Respiratory Support Coding: Emerging Trends and Technologies
The world of respiratory care is not static. Coders must be prepared for new technologies. For instance, the use of Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) or more advanced non-invasive interfaces are emerging. The New Technology Section is designed for this very purpose. As these modalities become standard of care, it is likely that new, more specific qualifiers (7th character) or even entirely new codes will be introduced to distinguish them from traditional BiPAP and CPAP. The fundamental principles of “Performance,” “Duration,” and “Consecutive” will remain the bedrock upon which these future codes are built.
11. Conclusion
Mastering the ICD-10-PCS code for prolonged BiPAP ventilation is a nuanced but essential skill that sits at the crossroads of clinical medicine, health information management, and healthcare finance. The assignment of code 5A09457 for episodes lasting beyond 48 hours is more than a data entry task; it is a precise declaration of a patient’s journey through a critical illness. By understanding the code’s structure, respecting the strict definition of consecutive time, navigating complex clinical and palliative scenarios, and relying on robust physician documentation, medical coders can ensure accuracy, compliance, and a true reflection of the resources expended in saving lives, one breath at a time.
12. Frequently Asked Questions (FAQs)
Q1: If a patient is on BiPAP for 23 hours and 59 minutes, what code is used?
A1: Code 5A09357 (Less than 24 consecutive hours) is used. The code descriptors are strict; 24 hours means a full 24 hours. Even one minute short requires the lower-duration code.
Q2: How is time calculated if a patient is transferred from an outside hospital on BiPAP?
A2: The receiving hospital is only responsible for coding the procedures performed during its own encounter. You must use the start time at your facility as time zero. The total time at the outside facility should not be aggregated with your facility’s time, as it is a separate encounter. Documentation should be requested to understand the patient’s clinical history, but it does not affect your PCS coding.
Q3: Is there a different code for the first 24 hours vs. the second 24 hours?
A3: No. The code is assigned once per continuous episode, and the duration character (5th character) reflects the total consecutive hours for that entire, uninterrupted episode. You do not code each 24-hour block separately.
Q4: What is the correct code for CPAP used for 50 consecutive hours?
A4: The code is the same: 5A09457. Both BiPAP and CPAP, when used for continuous respiratory support, fall under the “Performance” root operation and are specified by the Qualifier ‘7’ for “Other Equipment.” The clinical diagnosis and physician documentation will differentiate the two therapies.
Q5: Can we code for BiPAP if the patient self-extricates from the mask frequently?
A5: This is a documentation challenge. If the medical record indicates the intent was for continuous use, and the therapy was continuously available and being administered by staff (even if the patient repeatedly pulled it off), it is typically coded as continuous. The clinical team’s efforts to re-apply the mask support this. However, if the therapy was officially discontinued by a provider’s order due to patient intolerance, then the clock stops. Detailed documentation is key.
Date: November 20, 2025
Author: Healthcare Coding Insights Institute
Disclaimer: This article is intended for educational and informational purposes only and is based on the ICD-10-PCS guidelines and coding conventions available as of the publication date. It does not constitute official medical coding advice. Medical coders must consult the most current official ICD-10-PCS code set, Coding Clinic guidelines, and payer-specific policies for accurate coding. The author and publisher are not responsible for any errors, omissions, or consequences resulting from the use of this information.





