In the vast, intricate ecosystem of modern healthcare, where human life and complex technology intersect, there exists a language of profound consequence. It is a language not of words, but of alphanumeric sequences—a language that translates a surgeon’s skilled hands, a patient’s journey through pain to mobility, and a hospital’s resources into a data point that reverberates through the entire system. This is the world of medical coding. And within this world, few codes carry as much clinical, financial, and administrative weight as the one representing a Right Total Knee Arthroplasty in the ICD-10-PCS system.
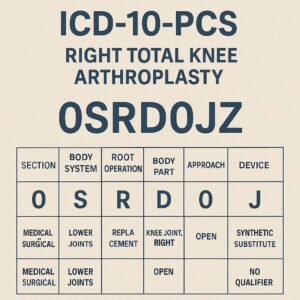
Imagine a code. Not as a dry, bureaucratic cipher, but as a dense, multidimensional capsule of information. The code 0SRD0JZ is such a capsule. To the untrained eye, it is meaningless. To the professional coder, the healthcare administrator, the researcher, and the health policy analyst, it tells a complete story: “Replacement of right knee joint with a synthetic substitute, open approach, using a cemented metal prosthetic component.” This single code communicates the what, the where, the how, and the with what of a major surgical event. It drives appropriate reimbursement, ensures accurate clinical data for registries, influences hospital quality metrics, and fuels research into orthopedic outcomes.
This article is a masterclass in understanding, constructing, and applying this critical code and its numerous variants. We will embark on a detailed journey exceeding 15,000 words, moving from the foundational anatomy of the knee, through the technical nuances of the ICD-10-PCS system, to the cutting edge of orthopedic innovation. This is not a simple lookup guide; it is a deep dive into the “why” behind the “what,” designed for aspiring and experienced medical coders, healthcare administration students, billing specialists, and curious clinical professionals who seek to master the precision required in this field. Our target audience is anyone who understands that in healthcare data, precision is not just about accuracy—it’s about integrity, fairness, and advancing medicine itself.
ICD-10-PCS Coding for Right Total Knee Arthroplasty
Table of Contents
Toggle2. The Knee Unraveled: A Primer on Anatomy and Pathology
To code a procedure, one must first understand the anatomy it seeks to restore. The knee is not a simple hinge; it is a marvel of biomechanical engineering, a complex synovial joint that must provide stability under immense load while allowing for smooth, flexible movement.
Key Anatomical Structures:
-
Femur: The thigh bone, whose distal end forms the rounded femoral condyles.
-
Tibia: The shin bone, whose proximal plateau provides the primary weight-bearing surface.
-
Patella: The kneecap, embedded in the quadriceps tendon, which articulates with the femoral groove.
-
Articular Cartilage: The slick, white tissue covering the ends of the bones, providing a near-frictionless surface.
-
Meniscus: Two C-shaped wedges of fibrocartilage (medial and lateral) that act as shock absorbers and stabilizers between the femur and tibia.
-
Synovial Membrane & Joint Capsule: The lining and sac that contain synovial fluid for lubrication.
-
Ligaments: The crucial stabilizers—the Anterior and Posterior Cruciate Ligaments (ACL, PCL) inside the joint, and the Medial and Lateral Collateral Ligaments (MCL, LCL) on the sides.
The Path to Replacement: Common Indications
Total knee arthroplasty is an elective procedure of last resort, considered only after conservative measures (physical therapy, medications, injections, lifestyle changes) have failed. The primary driver is the relentless pain and functional limitation caused by the irreversible destruction of the articular cartilage.
-
Primary Osteoarthritis (OA): The most common cause. The “wear-and-tear” arthritis where cartilage gradually erodes, leading to bone-on-bone contact, pain, stiffness, bony spur formation (osteophytes), and deformity.
-
Rheumatoid Arthritis (RA): An autoimmune, inflammatory disease where the synovial membrane proliferates and attacks the cartilage and bone, causing systemic joint destruction.
-
Post-Traumatic Arthritis: Following a significant fracture or ligamentous injury that damages the joint surface, leading to premature degenerative changes.
-
Avascular Necrosis (Osteonecrosis): Death of bone tissue due to interrupted blood supply, leading to collapse of the femoral condyle or tibial plateau.
The patient’s journey typically involves progressive pain (initially with activity, later at rest), swelling, stiffness (especially after sitting), decreased range of motion, and often the development of a varus (bow-legged) or valgus (knock-kneed) deformity. When this pain robs an individual of the ability to walk, work, sleep, or enjoy life, the conversation turns to TKA.
3. The Procedure Decoded: What is a Total Knee Arthroplasty?
A Total Knee Arthroplasty (TKA), commonly called a knee replacement, is a surgical procedure to resurface a damaged knee joint. The goal is to remove the diseased bone and cartilage and replace them with artificial components (prostheses) to restore alignment, function, and relieve pain. It is a meticulous, step-by-step process.
The Surgical Sequence:
-
Incision & Approach: A longitudinal incision is made over the anterior knee. The standard approach is open, directly visualizing the joint. The quadriceps tendon and patella may be moved aside (parapatellar approach).
-
Joint Exposure & Bone Preparation: The damaged joint surfaces are exposed. Precision cutting guides (instruments or computer navigation) are used to make exact bone cuts:
-
The distal end of the femur is resected to accept the femoral component.
-
The proximal surface of the tibia is resected flat to accept the tibial component.
-
The underside of the patella may be resurfaced to accept a patellar button (part of a “total” knee replacement, though sometimes omitted).
-
-
Trial Component Placement: Trial (temporary) components are inserted. The surgeon assesses knee stability, range of motion, alignment, and patellar tracking. Adjustments are made as necessary.
-
Final Implantation: The trial components are removed. The final prosthetic components are fixed in place. Fixation is a critical choice:
-
Cemented: Polymethylmethacrylate (PMMA) bone cement is used as a grout to secure the components to the bone. Common for most patients, especially those with osteoporosis.
-
Cementless: The prosthetic components have a porous or textured surface that allows the patient’s own bone to grow into it (biological fixation). Used for younger, more active patients with good bone quality.
-
Hybrid: One component (often the femur) is cemented, and the other (often the tibia) is press-fit without cement.
-
-
Closure: The joint is irrigated, drains may be placed, and the deep tissues, fascia, subcutaneous layer, and skin are closed in layers.
Understanding these steps is vital for coding, as each decision—the approach, the fixation method, the specific components used—must be reflected in the final ICD-10-PCS code.
4. The Foundation: Understanding the ICD-10-PCS Structure
ICD-10-PCS (Procedure Coding System) is a wholly different paradigm from its ICD-10-CM (diagnosis) counterpart. It is not a terminology but a multiaxial, standardized system where each character in a 7-character code has a specific meaning and position. There are no “default” assumptions. Every character must be chosen based on the documentation.
For the Medical and Surgical section (the first character ‘0’), the structure is as follows:
| Clinical Scenario | Key Documentation Clues | ICD-10-PCS Code | Code Breakdown |
|---|---|---|---|
| Standard Primary TKA, Cemented | “Cemented components,” “PMMA used for fixation” | 0SRD0J0 | 0: Med/Surg, S: Lower Joints, R: Replacement, D: Rt Knee, 0: Open, J: Synthetic, 0: Cement |
| Standard Primary TKA, Cementless | “Cementless,” “press-fit,” “porous-coated,” “bone ingrowth” | 0SRD0J1 | …J1: Cementless |
| Hybrid Fixation TKA | “Femoral component cemented, tibial component cementless” | 0SRD0J3 | …J3: Hybrid |
| Reverse Hybrid TKA | “Femoral component cementless, tibial component cemented” | 0SRD0J2 | …J2: Reverse Hybrid |
| Primary TKA, Fixation Unspecified | “Components implanted,” no mention of cement or press-fit (Query Required) | 0SRD0JZ | …JZ: No Qualifier (Unspecified) |
| Revision TKA (Stage 1: Spacer) | “Removal of existing prosthesis, insertion of antibiotic cement spacer” | 0SPD0LZ & 0SHD07Z | P: Removal, H: Insertion |
| Patellofemoral Arthroplasty (Right) | “Resurfacing of patella and femoral trochlea only” | 0SUD0JZ (or qualifier) | U: Supplement (Adding to the joint surface), different body part/op. |
This structure demands precision. The coder acts like a detective and an architect, building the code one verified piece of information at a time.
5. Deconstructing 0SRD: The Root Code for Right Knee Replacement
Let’s build our foundational code block for a standard right TKA.
-
1st Character – Section:
0-
This is a Medical and Surgical procedure. All invasive procedures that cut, alter, or manipulate tissue fall under this section.
-
-
2nd Character – Body System:
S-
This denotes the Lower Joints body system. In PCS, joints are their own distinct body systems, separate from bones.
Sis specifically for lower joints (hip, knee, ankle, toe). Upper joints (shoulder, elbow, wrist, finger) use the body systemR.
-
-
3rd Character – Root Operation:
R-
This is the heart of the code: Replacement. Per the official PCS definitions, “Replacement is taking out or off a device from a body part and putting back an identical or similar device in or on the same body part without cutting or puncturing the skin or a mucous membrane” OR more pertinently for a primary TKA, “putting in or on biological or synthetic material that physically takes the place and/or function of all or a portion of a body part.”
-
Key Concept: The body part (the knee joint) is being completely replaced by a prosthetic device. This is distinct from Reposition (moving to normal alignment), Supplement (adding to), or Bypass (rerouting).
-
-
4th Character – Body Part:
D-
This specifies the exact location: Knee Joint, Right. PCS is fully laterality-specific. The character
Dis reserved for the right knee joint. The left knee joint isE. This leaves no room for error; the documentation must clearly state “right.”
-
Our root code is now 0SRD. This sequence tells us: “A Medical and Surgical procedure on the Lower Joints, involving the Replacement of the Right Knee Joint…” The remaining three characters complete the story.
6. Beyond the Root: The Critical 6th and 7th Character Choices
While the first four characters set the stage, the 5th, 6th, and particularly the 7th character are where the granular, clinically significant details are captured.
5th Character: The Approach – A Gateway to Complexity
The approach describes how the surgeon accessed the knee joint. For most primary TKAs, this is straightforward.
-
0– Open: Cutting through the skin or mucous membrane and other body layers to directly visualize the anatomical site. This is the standard approach for a TKA. The entire joint is exposed. -
Other Approaches (Less Common in Primary TKA):
-
3– Percutaneous: Entry by puncture or minor incision, using instrumentation for the procedure without direct visualization. NOT used for a full joint replacement. -
4– Percutaneous Endoscopic: Percutaneous entry with the use of a visualizing scope. While arthroscopy is common for knee diagnostics (like meniscectomy), it is not a viable approach for implanting the large components of a TKA. However, it may be used in conjunction with an open approach for diagnostic or assistive purposes, but the approach for the replacement itself remains “Open.”
-
For our standard case, the 5th character is 0. Code now: 0SRD0
6th Character: The Device – The Heart of the Matter
This character specifies what is being put in to replace the body part. In a TKA, this is the prosthetic implant. The PCS table for Lower Joints, Replacement, provides specific options.
-
J– Synthetic Substitute: This is the core device value for a primary TKA. It encompasses the entire prosthetic knee system—the metal femoral component, the tibial tray (metal), the polyethylene (plastic) insert, and often a patellar button. “Synthetic Substitute” is a broad category for man-made materials replacing a body part. -
K– Nonautologous Tissue Substitute: This refers to non-living biological tissue from another human or animal (e.g., cadaveric cartilage, donor tissue). This is not used for a standard TKA. It might be used in a rare reconstructive procedure but not for a total joint replacement with metal and plastic.
For a standard primary TKA, the 6th character is J. Code now: 0SRD0J
7th Character: The Qualifier – The Crucial Differentiator
This is arguably the most important character for TKAs, as it defines the fixation method—how the implant is secured to the bone. This has major clinical and sometimes reimbursement implications.
-
Z– No Qualifier: Used only when the documentation does not specify a fixation method. This should be a last resort. Coders must query the surgeon for clarification if the operative report is silent on this critical detail. -
0– Cement: The prosthesis is fixed using poly-methyl methacrylate (PMMA) bone cement. Documentation keywords: “cemented,” “with cement,” “PMMA.” -
1– Cementless: The prosthesis is fixed via press-fit or bone ingrowth. Documentation keywords: “cementless,” “porous-coated,” “hydroxyapatite-coated,” “press-fit,” “biological fixation.” -
2– Reverse Hybrid: The femoral component is cementless, and the tibial component is cemented. Must be explicitly documented. -
3– Hybrid: The femoral component is cemented, and the tibial component is cementless. Must be explicitly documented.
The 7th character choice is driven entirely by explicit surgeon documentation.
7. The Surgeon’s Narrative: Linking Documentation to the Code
The operative report is the coder’s bible. It must be read thoroughly. Key phrases that map directly to PCS characters include:
-
For Laterality (4th Character): “Right total knee arthroplasty,” “Right TKA,” “Addressed the right knee joint.”
-
For Approach (5th Character): “A standard midline anterior incision was made… The joint was entered via a medial parapatellar arthrotomy.” (This describes an Open approach).
-
For Device (6th Character): Implant stickers in the report listing the manufacturer (e.g., Zimmer NexGen, Stryker Triathlon, DePuy Attune) confirm a Synthetic Substitute.
-
For Qualifier – Fixation (7th Character):
-
“The tibial and femoral components were cemented in place using Palacos cement.” →
0– Cement -
“A cementless, porous-coated femoral component was impacted. A cementless tibial baseplate with trabecular metal was secured.” →
1– Cementless -
“The femoral component was cemented. A cementless tibial component was press-fit.” →
3– Hybrid -
“The femoral component was press-fit. The tibial component was cemented.” →
2– Reverse Hybrid
-
The coder must never assume. If the report says “total knee components were placed” without mentioning fixation, a query is mandatory.
8. Case Studies in Complexity: From Simple to Highly Unusual
Case Study 1: The Standard Primary TKA
-
Documentation: “Uneventful right total knee arthroplasty. Implanted cemented femoral and tibial components with a polyethylene insert and patellar resurfacing.”
-
Code:
0SRD0JZ? NO. Wait. It says “cemented.” The qualifier is not ‘Z’ (unspecified). It is ‘0’ for Cement. -
Correct Code:
0SRD0J0(Replacement of Right Knee Joint with Synthetic Substitute, Open Approach, Cemented).
Case Study 2: The Young Athlete with Osteonecrosis
-
Documentation: “Right total knee arthroplasty for avascular necrosis in a 45-year-old male. Given excellent bone stock, a cementless, porous-coated implant system was used for both femoral and tibial components.”
-
Code:
0SRD0J1(Replacement of Right Knee Joint with Synthetic Substitute, Open Approach, Cementless).
Case Study 3: The Complex Revision TKA (A Different Root Operation)
-
Scenario: A patient presents 10 years after a primary TKA with a loose, painful implant. The surgeon removes the old femoral and tibial components, places antibiotic-impregnated cement spacers, and plans for a new implant in 6 weeks after infection clears.
-
Coding Logic: This is NOT a Replacement during the first stage. The objective is to take out the old device and put in a temporary spacer to deliver antibiotics. This is a Removal of the old device (root operation:
P– Removal) and an Insertion of a drainage device (the antibiotic spacer) into the joint (root operation:H– Insertion). -
Potential Codes:
0SPD0LZ(Removal of Device from Right Knee Joint, Open Approach) and0SHD07Z(Insertion of Irrigation Device into Right Knee Joint, Open Approach). This illustrates that a “revision” surgery often involves multiple, distinct PCS root operations.
9. The Table of Precision: A Coding Roadmap
The table below serves as a quick-reference guide for coding the most common Right TKA scenarios. Remember, the operative report is the final authority.
| Clinical Scenario | Key Documentation Clues | ICD-10-PCS Code | Code Breakdown |
|---|---|---|---|
| Standard Primary TKA, Cemented | “Cemented components,” “PMMA used for fixation” | 0SRD0J0 | 0: Med/Surg, S: Lower Joints, R: Replacement, D: Rt Knee, 0: Open, J: Synthetic, 0: Cement |
| Standard Primary TKA, Cementless | “Cementless,” “press-fit,” “porous-coated,” “bone ingrowth” | 0SRD0J1 | …J1: Cementless |
| Hybrid Fixation TKA | “Femoral component cemented, tibial component cementless” | 0SRD0J3 | …J3: Hybrid |
| Reverse Hybrid TKA | “Femoral component cementless, tibial component cemented” | 0SRD0J2 | …J2: Reverse Hybrid |
| Primary TKA, Fixation Unspecified | “Components implanted,” no mention of cement or press-fit (Query Required) | 0SRD0JZ | …JZ: No Qualifier (Unspecified) |
| Revision TKA (Stage 1: Spacer) | “Removal of existing prosthesis, insertion of antibiotic cement spacer” | 0SPD0LZ & 0SHD07Z | P: Removal, H: Insertion |
| Patellofemoral Arthroplasty (Right) | “Resurfacing of patella and femoral trochlea only” | 0SUD0JZ (or qualifier) | U: Supplement (Adding to the joint surface), different body part/op. |
10. Common Pitfalls and Auditor Red Flags
-
Assuming Laterality: Never code from a schedule that says “TKA” without confirming right vs. left in the report.
0SRDis not the same as0SRE. -
Defaulting to ‘Z’ (Unspecified) for Fixation: This is a major audit risk and can lead to payment denial or down-coding. It indicates incomplete documentation.
-
Confusing Root Operations: Calling a Removal of hardware a Revision. Revision is a clinical term, not a PCS root operation. You must identify the objective: Removal, Replacement, Insertion, etc.
-
Ignoring Multiple Procedures: A TKA often includes a concomitant Synovectomy (excision of synovial tissue) or a Ligament Repair. These are separate, additional PCS codes (e.g.,
0SBG0ZZfor excision of right knee synovium). -
Mishandling Bilateral Procedures: Each knee replacement is coded separately (
0SRD0J0and0SRE0J0). A modifier (like -50 in CPT) is not used in PCS; the laterality is in the code itself.
11. The Impact of Precision: From Reimbursement to Big Data
Accurate coding transcends the billing office. A precisely coded 0SRD0J1 (cementless) vs. 0SRD0J0 (cemented) has ripple effects:
-
Reimbursement: DRGs (Diagnosis-Related Groups) may differ based on procedure complexity and device use. Accurate coding ensures fair payment for the hospital’s resources.
-
Clinical Registries: National joint registries (like the American Joint Replacement Registry) use this data to track implant longevity, complication rates, and surgical outcomes. Mis-coded fixation skews this vital research.
-
Quality Metrics & Public Reporting: Hospital complication and readmission rates for specific procedures are publicly reported. Accurate procedural data is essential for fair comparisons.
-
Supply Chain & Inventory: Hospital administration uses procedure volume data (e.g., cementless vs. cemented knees) to manage implant purchasing and inventory.
12. The Future: Robotics, Custom Implants, and Coding Evolution
The field of TKA is evolving, and PCS must adapt.
-
Robotic-Arm Assisted Surgery: This is still an Open approach (character 5 = 0). The robotic system is a tool for precision bone preparation. The PCS code does not currently have a character to denote robotic assistance; this is captured elsewhere in the claim (e.g., with a separate CPT code or a device code).
-
Patient-Specific Instrumentation (PSI) & Custom Implants: Implants manufactured from a patient’s own MRI/CT scan are still a Synthetic Substitute (character 6 = J). The custom nature is a manufacturing detail not currently distinguished in PCS.
-
The Potential for a “J-Family”: As technology diversifies, future PCS updates may expand the 6th or 7th character to specify “robotic-assisted,” “custom 3D-printed,” or “biologic-coated” implants, demanding even greater coding specificity.
13. Conclusion
Mastering the ICD-10-PCS code for a right total knee arthroplasty is a microcosm of the modern medical coding profession. It requires a synthesis of anatomical knowledge, surgical understanding, meticulous attention to documentation, and strict adherence to a logical, multiaxial system. The code 0SRD0J0 is not just a string of characters; it is a precise, data-rich testament to a life-changing intervention. As technology advances and healthcare data becomes ever more critical, the role of the skilled coder in ensuring this precision only grows in importance. By building each code with care, professionals uphold the integrity of patient records, ensure the financial stability of healthcare institutions, and contribute to the broader landscape of medical knowledge that will shape the future of orthopedic care.
14. Frequently Asked Questions (FAQs)
Q1: What if the operative report only says “right total knee arthroplasty” and doesn’t mention cement?
A: You must query the surgeon. The default should not be to use Z (No Qualifier). The fixation method is a critical piece of information for clinical and coding purposes. A query such as, “Can you please specify the fixation method used for the femoral and tibial components (e.g., cemented, cementless, hybrid)?” is necessary.
Q2: How do I code a partial (unicompartmental) knee arthroplasty?
A: A partial knee replacement is still coded as Replacement (Root Operation R). However, the Body Part character changes. Instead of the entire “Knee Joint” (D), you would use a more specific body part value from the Lower Joints table, such as “Right Knee Joint, Medial Compartment” (if listed). You must consult the current PCS table for the precise body part character.
Q3: The surgeon used computer navigation. Does that change the PCS code?
A: No, not currently. Like robotic assistance, computer navigation is a tool for enhancing the precision of the bone cuts. The fundamental approach (Open) and the procedure (Replacement) remain the same. It is captured elsewhere in the billing process, not in the ICD-10-PCS code structure.
Q4: What is the correct code for removing an old knee implant (a revision)?
A: The correct root operation is Removal (P). The code would be 0SPD0LZ (Removal of Device from Right Knee Joint, Open Approach). The qualifier ‘Z’ is used because the type of device being removed (the old synthetic substitute) is inherent in the procedure context.
Q5: Are there different codes for different brands of knee implants (Zimmer, Stryker, etc.)?
A: No. In ICD-10-PCS, all manufactured knee implant systems are classified under the device “Synthetic Substitute” (character J). The specific brand and model are captured using a different system, typically a Unique Device Identifier (UDI) or a manufacturer-specific code submitted separately on the claim.
15. Additional Resources
-
Centers for Medicare & Medicaid Services (CMS): The official ICD-10-PCS files, tables, and guidelines: https://www.cms.gov/medicare/coding-billing/icd-10-codes
-
American Health Information Management Association (AHIMA): Premier organization for coding professionals, offering education, certifications, and current articles. https://www.ahima.org
-
American Academy of Orthopaedic Surgeons (AAOS): For clinical background, terminology, and surgical techniques. https://www.aaos.org
-
American Joint Replacement Registry (AJRR): To understand how coded data is used in real-world outcomes research. https://www.aaos.org/registries/ajrr/
-
The Coding Institute’s Orthopedic Coding Alert: A specialty newsletter offering practical coding scenarios and updates.
Date: December 09, 2025
Author: The Clinical Coding Specialist
Disclaimer: This article is for educational and informational purposes only. It is not a substitute for official coding guidelines, payer-specific advice, or clinical consultation. Always consult the most current ICD-10-PCS code set, official coding guidelines, and physician documentation for final coding decisions.





