In the intricate world of medical coding, few procedures present a challenge as complex and nuanced as spinal fusion. For the coder, it is a puzzle where each piece—anatomy, surgical intent, technological approach, and implantable hardware—must be perfectly aligned to construct an accurate and compliant picture. An incorrectly placed code is not merely a clerical error; it can distort clinical data, impede research, trigger audit flags, and ultimately jeopardize the financial integrity of a healthcare institution. The transition to ICD-10-PCS brought with it an unprecedented level of specificity, moving from a handful of fusion codes in ICD-9-CM to hundreds, if not thousands, of potential combinations. This granularity, while powerful, demands a coder be part anatomist, part surgical technician, and part linguistic detective.
This article is designed to be your definitive navigational chart through this labyrinth. We will embark on a detailed, professional journey exceeding 15,000 words, dissecting every character of the ICD-10-PCS code for spinal fusion. We will move beyond simple definitions into the realm of applied mastery. You will learn not just what the codes are, but why they are structured as such and how to derive them from the most complex operative reports. From the foundational principles of the PCS system to advanced scenarios involving combined approaches and hybrid constructs, this guide aims to transform confusion into clarity. Prepare to delve deep into the vertebrae, explore surgical corridors, and decipher the language of spinal devices, all in pursuit of coding excellence.
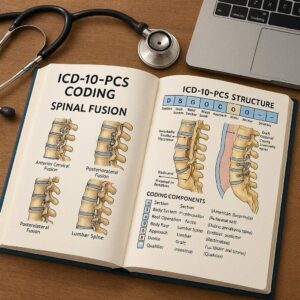
ICD-10-PCS Coding for Spinal Fusion
Foundational Knowledge: The Building Blocks of ICD-10-PCS
Before confronting the spine, one must understand the toolbox. ICD-10-PCS (Procedure Coding System) is a multi-axial, alphanumeric system. Each code is seven characters long, and each character has a specific meaning within a defined table. This structure is fundamentally different from ICD-9-CM and requires a paradigm shift in thinking.
-
Characters Represent Specific Attributes: Each of the seven positions provides distinct information about the procedure.
-
Tables are Key: Codes are built by selecting values from rows and columns within a specific PCS table. You do not “look up” a procedure name; you build the code based on its components.
-
Standardized Definitions: Every root operation (Character 3) has a precise, standardized definition that must be applied strictly, regardless of the colloquial surgical term used.
The power—and complexity—of PCS lies in this structure. A single change in one character, say the approach from “open” to “percutaneous,” creates a completely unique code, reflecting a fundamentally different procedural technique and patient resource use.
Deconstructing the Spinal Fusion Code: The 7th Character System
Every ICD-10-PCS code for a Spinal Fusion in the Medical and Surgical section will follow this blueprint:
0 | G | R | V | J | 9 | G
(Example: Posterior Approach, L4-L5, Interbody Fusion Device)
Let’s break down what each character represents:
-
1st Character: Section. Always 0 for “Medical and Surgical.”
-
2nd Character: Body System. This changes based on the root operation and the part of the spine. For fusion (root operation “G”), it is either:
-
G for “Musculoskeletal System” (for joints of extremities, spine, etc.)
-
R for “Musculoskeletal System – Bones” (for bones themselves, like vertebral bodies).
-
We will clarify this critical distinction in the Root Operation section.
-
-
3rd Character: Root Operation. Always G for “Fusion.”
-
4th Character: Body Part. This specifies the exact vertebral joint(s) being fused (e.g., C3-C4, T9-T10, L4-L5, L5-S1, or multiple levels).
-
5th Character: Approach. How the surgeon accessed the site (e.g., Open, Percutaneous, Posterior, Anterior, etc.).
-
6th Character: Device. What, if anything, is put in the body to aid the fusion (e.g., Interbody Fusion Device, Synthetic Substitute, Autologous Tissue Substitute).
-
7th Character: Qualifier. For spinal fusions, this almost always indicates the number of vertebral joints fused. This is a critical element for specificity.
The coder’s task is to extract the correct value for each of these seven slots from the operative report.
Section 1: The “Medical and Surgical” Section (0)
This is the simplest character. Any procedure that is surgical in nature (involving cutting, putting in devices, removing tissue, etc.) falls into this section. All spinal fusions we will discuss are in Section “0.”
Section 2: The Body System (Root Operation Dependent)
This is our first major decision point, and it hinges entirely on the PCS definition of the root operation “Fusion.”
-
Definition of Fusion (G): “Joining together portions of an articular body part rendering the articular body part immobile.” The key term is “articular body part.”
-
An articular body part is a joint. Therefore, spinal fusion is the joining of a spinal joint.
In the spine, there are two primary types of joints:
-
The Intervertebral Joint (Symphysis): The joint between two vertebral bodies, connected by the intervertebral disc. This is the joint fused in an interbody fusion.
-
The Vertebral Arch Joint (Facet Joint): The posterior joints between vertebral arches. These are fused in a posterior fusion (posterolateral gutter fusion).
Here is the crucial rule:
-
If the procedure targets the intervertebral joint (the disc space), you are fusing an articular body part that is part of the “joints” of the musculoskeletal system. Therefore, the 2nd character is G (Musculoskeletal System).
-
If the procedure targets the vertebral arch (the posterior elements like lamina and facets) for fusion, you are not fusing a defined “joint” in the PCS tables. You are fusing bone. Therefore, the 2nd character is R (Musculoskeletal System – Bones).
Body System (2nd Character) Determination for Spinal Fusion
| Target of Fusion | Anatomic Structure | PCS Body Part Consideration | 2nd Character |
|---|---|---|---|
| Interbody Space | Intervertebral Disc / Vertebral Bodies | Articular Joint | G (Musculoskeletal System) |
| Posterior Elements | Lamina, Facets, Transverse Processes | Bone | R (Musculoskeletal System – Bones) |
| Combined | Both of the above | Two separate codes are typically required. | G for the interbody, R for the posterior. |
Section 3: The Root Operation – “Fusion” (G)
We’ve touched on the definition. It’s vital to understand what fusion is not:
-
It is not Arthrodesis (which is also joining to render immobile, but is found in the “Lower Joints” body system for extremities).
-
It is not Insertion or Replacement of a device (those are separate root operations, though a device may be used in conjunction with a fusion).
-
The intent is permanent immobilization of the joint.
Section 4: The Body Part – A Detailed Atlas of the Spine
This is where specificity soars. The 4th character identifies the precise vertebral joint(s). The values differ between the “G” and “R” body system tables.
In the “G” Body System Table (Interbody Fusions):
Body parts are specific joints: C2-C3, C3-C4, … L4-L5, L5-S1. There are also values for “Cervical Vertebrae, 2 or more” or “Lumbar Vertebrae, 2 or more” which are used when multiple contiguous joints are fused from a single anterior/posterior interbody approach. You must carefully count the joints, not the vertebrae. An L4-S1 fusion involves two joints: L4-L5 and L5-S1.
In the “R” Body System Table (Posterior Fusions):
Body parts are specific vertebrae or ranges: Cervical vertebra, Thoracic vertebra, Lumbar vertebra, Sacrum. For multiple levels, you use values like “Lumbar Vertebra, 2 or more.” Here, you are counting vertebral bodies that have bone graft applied posteriorly.
*Illustration: A labeled spinal column diagram with arrows pointing to sample body part values: “C5-C6” for the G table and “Thoracic Vertebra, 2 or more” for the R table.*
Section 5: The Approach – How Surgeons Access the Spine
The 5th character describes the technique used to reach the operative site. For spinal fusions, common approaches include:
-
0 – Open: Cutting through the skin and fascia (e.g., standard posterior midline incision).
-
J – Percutaneous: Via needle-puncture or small incision, often endoscopic-assisted.
-
8 – Percutaneous Endoscopic: A specific subset of percutaneous.
-
Approach values that define direction:
-
A – Anterior: Approaching from the front of the body.
-
B – Anterior Extrapritoneal: For lumbar access, staying outside the peritoneal cavity.
-
D – Posterior: Approaching from the back.
-
F – Posterior / Anterior: Used for a combined approach during the same operative episode (e.g., an ALIF followed immediately by a posterior instrumentation). This often requires careful analysis.
-
The approach is independent of the body system. An anterior lumbar interbody fusion (ALIF) is Anterior Approach to the Lumbar Vertebral Joint in the G body system.
Section 6: The Device – Interbody Devices, Synthetics, and Autografts
The 6th character specifies what is placed to aid the fusion. Crucially, if no device remains after the procedure, the value is “Z – No Device.”
-
J – Interbody Fusion Device: A structural cage (e.g., PEEK, titanium, carbon fiber) placed in the disc space. Common in TLIF, PLIF, ALIF.
-
M – Synthetic Substitute: Bone graft extenders or replacements (e.g., BMP, calcium phosphate, ceramics).
-
N – Autologous Tissue Substitute: The patient’s own bone (e.g., iliac crest bone graft – ICBG, local bone from laminectomy).
-
Note: Internal fixation devices (rods, screws, plates) are NOT coded here. They are considered “fixation devices” used in the root operation “Insertion” or “Supplement” and are coded separately if the objective is solely fixation and not fusion.
Section 7: The Qualifier – Defining the Number of Levels
This is the final piece of specificity. For fusions in the “G” body system, the qualifier indicates the number of vertebral joints fused.
-
G – 1 Vertebral Joint (e.g., L4-L5 only)
-
H – 2 Vertebral Joints (e.g., L4-S1)
-
J – 3 Vertebral Joints
-
K – 4 Vertebral Joints
-
L – 5 or more Vertebral Joints
-
M – 9 or more Vertebral Joints
For fusions in the “R” body system (posterior bone fusion), the qualifier is almost always Z – No Qualifier, unless otherwise specified in the table.
Advanced Scenarios and Case Studies
Case Study 1: Transforminal Lumbar Interbody Fusion (TLIF) at L4-L5 with Percutaneous Screws.
-
Procedure: Surgeon performs a posterior open approach, removes the L4-L5 disc, places a PEEK cage with BMP and local bone graft into the disc space, and places percutaneous pedicle screws.
-
Coding:
-
Interbody Fusion: 0SG30J9 (Fusion, L4-L5 joint, Open, Interbody Fusion Device, Single Joint). This captures the TLIF procedure itself.
-
Posterior Instrumentation: A separate code from the Insertion table (0RH… ) for the percutaneous pedicle screws. The posterolateral bone graft is inherent to the approach and not separately coded as a fusion.
-
Case Study 2: Anterior Cervical Discectomy and Fusion (ACDF) at C5-C6 and C6-C7 with Allograft and Plate.
-
Procedure: Anterior neck approach, removal of C5-C6 and C6-C7 discs, placement of allograft spacers in each space, placement of an anterior cervical plate.
-
Coding: 0SG20JH (Fusion, Cervical Vertebrae 2 or more, Open, Interbody Fusion Device, 2 Vertebral Joints). The plate is separately coded (0SH…).
Common Pitfalls and How to Avoid Them
-
Confusing Body Systems (G vs. R): Re-read the definition of “articular body part.” If the disc space is fused, use G. If only posterior bone graft is placed, use R.
-
Miscounting Levels: Distinguish vertebrae from joints. A fusion from L3 to L5 involves two joints: L3-L4 and L4-L5.
-
Omitting Separate Codes for Instrumentation: Rods, screws, and plates are not part of the fusion code. They are separately reportable procedures.
-
Assuming “No Device” for Autograft: Autologous bone (N) is a device in PCS. “No Device” (Z) means nothing is placed (e.g., in a fusion where only decortication is done, which is virtually non-existent).
The Intersection of Coding, Compliance, and Reimbursement
Accurate PCS coding directly impacts DRG (Diagnosis-Related Group) assignment for inpatient stays. A single-level fusion (DRG 459/460) has a different reimbursement weight than a multi-level fusion (DRG 453/454) or a fusion with major comorbidity. Incorrectly specifying the number of levels or missing a combined approach can lead to a significant financial loss or an overpayment, risking audit recovery. Coders are the guardians of data integrity, ensuring that the code tells the true, detailed story of the surgical event.
Conclusion
Mastering ICD-10-PCS for spinal fusion is a demanding yet essential skill for inpatient coders. It requires a meticulous, definition-driven approach to dissecting operative reports, a solid grasp of spinal anatomy and surgical techniques, and an unwavering commitment to specificity. By systematically addressing each of the seven characters—particularly the critical distinctions in Body System, Body Part, and Qualifier—the coder can confidently construct accurate, compliant codes that reflect the complexity of modern spinal surgery. This precision ensures proper reimbursement, supports valuable clinical data, and upholds the standard of professional coding practice.
Frequently Asked Questions (FAQs)
Q1: How do I code a posterolateral fusion (PLF) without interbody devices?
A: A pure PLF involves placing bone graft on the decorticated posterior elements (transverse processes, facet joints). Since this is fusion of bone and not a defined articular joint, you use the “R” body system. The code would be something like 0RG00JZ (Fusion, Lumbar Vertebra, Open, No Device, No Qualifier) for a single level, or 0RG10JZ for 2 or more lumbar vertebrae.
Q2: What if the surgeon uses both an interbody cage and posterior bone graft?
A: This is a combined fusion. You would code:
-
One code for the interbody fusion (Body System G).
-
A second code for the posterior bone fusion (Body System R), if the documentation explicitly states a separate posterolateral arthrodesis was performed (not just bone graft placed in the facet joints after cage insertion, which may be inherent).
Q3: Does a “minimally invasive” surgery automatically mean “Percutaneous” approach?
A: Not always. “Minimally invasive” is a clinical term. In PCS, “Open” (0) means cutting through skin and fascia to expose the site. A mini-open TLIF with a tubular retractor still uses an “Open” approach. “Percutaneous” (J) is reserved for procedures performed via needle-puncture or tiny incision without an open visualization of the site. Endoscopic procedures may be “Percutaneous Endoscopic” (8).
Q4: How do I handle a fusion that crosses regions (e.g., T12-S1)?
A: You must use the body part value that accurately describes the vertebrae/joints fused. There is no single value for “thoracolumbar” joint. You would use a combination of codes or, if all joints are fused via a single interbody approach from the front, you might use a value like “Vertebral Joint, 9 or more” if applicable, depending on the table. Often, these complex fusions require careful coding of each distinct segment.
Date: December 10, 2025
Author: The Healthcare Coding Specialist
Disclaimer: This article is intended for educational purposes and to illustrate coding principles. It is not a substitute for the official ICD-10-PCS code books, guidelines, or provider documentation. Coders must always rely on the most current official resources and clinical record when assigning codes.





