In the dynamic landscape of interventional cardiology and cardiothoracic surgery, few innovations have been as transformative as Transcatheter Aortic Valve Replacement (TAVR). From a high-risk, last-resort intervention to a mainstream therapy for severe aortic stenosis across all risk categories, TAVR has reshaped patient care pathways. Yet, for every sophisticated deployment of a bioprosthetic valve, there exists an equally complex narrative written not in clinical notes, but in the alphanumeric language of medical codes. This narrative determines hospital reimbursement, impacts quality metrics, and fuels critical health services research. The ICD-10-PCS code for a TAVR procedure is far more than a billing marker; it is a precise, multi-axial descriptor of a patient’s journey through a cutting-edge therapy.
This definitive guide is crafted for the medical coding professional, the cardiovascular service line analyst, and the healthcare administrator who seeks not just to assign a code, but to understand the intricate anatomy of its construction. We will embark on a deep dive that transcends basic code lookup, exploring the clinical nuances, coding guidelines, and philosophical underpinnings of the ICD-10-PCS system as it applies to TAVR. With the procedure’s volume soaring, the risk of coding inaccuracies—leading to revenue loss or compliance issues—has never been greater. This article, exceeding a detailed exploration of thousands of words, aims to fortify your expertise, turning coding from a task into a specialized skill central to the financial and operational vitality of modern cardiovascular care.
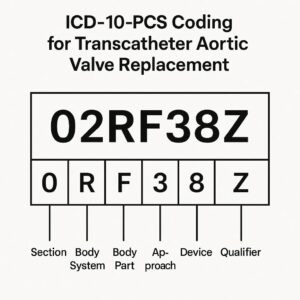
ICD-10-PCS Coding for Transcatheter Aortic Valve Replacement
2. Understanding TAVR: A Clinical Primer for Coders
To code accurately, one must first understand what is being coded. TAVR, also known as Transcatheter Aortic Valve Implantation (TAVI), is a minimally invasive procedure to replace a diseased aortic valve. Unlike open-heart surgical aortic valve replacement (SAVR), TAVR does not require sternotomy or cardiopulmonary bypass.
The Problem: Aortic Stenosis
The aortic valve is the gateway between the heart’s left ventricle and the aorta. Severe calcific aortic stenosis narrows this opening, forcing the heart to work harder, leading to heart failure, syncope, angina, and ultimately, death if untreated.
The TAVR Solution:
A collapsible bioprosthetic valve, mounted on a stent and delivery catheter, is compressed and advanced to the native valve site. The primary access routes are:
-
Transfemoral (TF): The most common (>80%). The catheter is threaded from the femoral artery in the groin, retrograde up the aorta to the heart.
-
Transapical (TA): Access via a small incision between the ribs, puncturing the left ventricular apex. Used when femoral access is unsuitable.
-
Alternative Access: Includes transaortic (direct aortic arch), subclavian, carotid, and caval-aortic approaches.
The new valve is positioned within the native, calcified valve and deployed, either by balloon expansion or self-expansion. It immediately begins functioning, pushing the diseased leaflets aside.
Why This Matters for Coding: The access approach, the need for cardiopulmonary bypass (rarely used in TAVR as a “standby” or in complex cases), concomitant procedures, and the specific device used are all critical variables that will directly influence the final ICD-10-PCS code.
3. Navigating the ICD-10-PCS Universe: Foundational Concepts
ICD-10-PCS is a procedural classification system built on a structure of seven alphanumeric characters. Each character represents an axis of specification, providing a high degree of granularity.
-
Character 1: Section – The broadest category (e.g., Medical and Surgical, Placement).
-
Character 2: Body System – The general physiological system (e.g., Heart and Great Vessels).
-
Character 3: Root Operation – The single most important concept. The objective of the procedure (e.g., Replacement, Insertion).
-
Character 4: Body Part – The specific site of the procedure.
-
Character 5: Approach – How the procedure site was reached (e.g., Percutaneous, Open).
-
Character 6: Device – The item left in place after the procedure.
-
Character 7: Qualifier – An additional attribute, often used to specify diagnostic or other contextual information.
For TAVR, we operate almost exclusively in the Medical and Surgical section (Character 1: 0) on the Heart and Great Vessels body system (Character 2: 2).
4. Deconstructing the TAVR Procedure: A Step-by-Step Coding Analysis
A typical transfemoral TAVR involves multiple reportable procedural steps. Coders must analyze the operative report to identify each distinct objective.
-
Access and Crossing: The physician gains arterial access, often using ultrasound guidance, and places a sheath. Wires are advanced across the aortic valve.
-
Coding Impact: This is typically included in the main procedure and not separately coded unless a separate, significant service like a diagnostic cardiac catheterization is performed.
-
-
Balloon Aortic Valvuloplasty (BAV): A balloon is often inflated to pre-dilate the calcified native valve, creating space for the TAVR valve.
-
Coding Impact: This is a separately reportable procedure. Root Operation: Dilation of the Aortic Valve via Percutaneous approach. (e.g., 02703ZZ).
-
-
Valve Deployment: The TAVR delivery system is advanced, positioned, and the valve is deployed.
-
Coding Impact: This is the core TAVR procedure. The root operation is debated (see next section).
-
-
Post-Dilation: Sometimes a second balloon inflation is needed to fully seat the valve.
-
Coding Impact: Another instance of Dilation, separately coded.
-
-
Permanent Pacemaker (PPM) Implantation: A significant minority of patients (10-20%) develop conduction abnormalities requiring a new PPM.
-
Coding Impact: A separate procedure from a different PCS table (e.g., Placement, Heart and Great Vessels table for leads, Administration for the pulse generator).
-
-
Access Site Management: Closure devices (e.g., Perclose, Mynx) are used.
-
Coding Impact: Usually included in the vascular access closure. May be coded if a separate Repair of the artery is documented.
-
5. The Core Decision: Root Operations for TAVR (02RF vs. X2RF)
This is the central, and often misunderstood, aspect of TAVR coding. Two root operations are candidates: Replacement (R) and Insertion (J).
Official Coding Guideline B3.10: “If the objective of the procedure is to take over the function of a body part, the root operation is Replacement. If the objective is to put in a device without taking over the function of a body part, the root operation is Insertion.”
The Argument for Replacement (02RF):
-
The TAVR valve unequivocally takes over the function of the native aortic valve.
-
The native valve leaflets are not removed; they are permanently displaced and rendered non-functional. The new valve assumes the physiological role.
-
The ICD-10-PCS Replacement table for the Heart and Great Vessels includes a specific body part value for the “Aortic Valve” and numerous device values for synthetic and zooplastic substitutes. This aligns perfectly with TAVR.
-
This is the predominant, industry-standard choice supported by the AHA Coding Clinic and most payer policies.
The Argument for Insertion (X2RF):
-
Some argue that since the native valve is not excised, it is not “replaced” in the traditional surgical sense. They view the valve as being “inserted” into the aortic valve space.
-
The Insertion table also has an “Aortic Valve” body part and device values.
-
However, this interpretation conflicts with the core definition focusing on function, not anatomical removal.
Authoritative Guidance: The AHA Coding Clinic for ICD-10-CM/PCS, Fourth Quarter 2016, page 90, addressed this directly: “For a transcatheter aortic valve replacement (TAVR) procedure… the appropriate root operation is Replacement.” This settled the debate for compliant coding.
Conclusion: The correct root operation for a standard TAVR procedure is Replacement (R). The core code family begins with 02R (Medical/Surgical, Heart & Great Vessels, Replacement).
6. Detailed Code Building: The Seven Characters of Precision
Let’s build a complete code for a typical case: Transfemoral TAVR with a balloon-expandable bovine pericardial valve.
-
Character 1: Section = 0 (Medical and Surgical)
-
Character 2: Body System = 2 (Heart and Great Vessels)
-
Character 3: Root Operation = R (Replacement)
-
Character 4: Body Part = F (Aortic Valve)
Values: F=Aortic Valve. Other less common: G=Mitral Valve, etc. -
Character 5: Approach = 4 (Percutaneous)
*This is key for transfemoral/transseptal access. For transapical or transaortic, it would be “Open” (0).* -
Character 6: Device = K (Zooplastic Tissue)
This is the most critical device decision. See Section 8 below. -
Character 7: Qualifier = Z (No Qualifier)
Typically Z for TAVR. Other qualifiers might be used for hybrid procedures or other specifics.
Final Code: 02RF4KZ – Replacement of Aortic Valve with Zooplastic Tissue, Percutaneous Approach.
What about a self-expanding valve with porcine tissue? The approach (percutaneous) and body part (aortic valve) are the same. Only the device character changes based on the manufacturer’s specifications.
7. The Concomitant Procedures Challenge
TAVR is rarely performed in isolation. Coders must be vigilant for other PCS-coded procedures.
-
Balloon Aortic Valvuloplasty (BAV): 02703ZZ – Dilation of Aortic Valve, Percutaneous Approach.
-
Coronary Angioplasty/Stenting: Coded from the Dilation or Restriction tables in the Lower Arteries system.
-
Pacemaker Implantation: A two-system code set.
-
Lead(s): 02HK0JZ, 02H60JZ (Insertion of pacemaker lead into heart chambers).
-
Pulse Generator: 0JH808Z (Insertion of pacemaker device into chest subcutaneous tissue).
-
-
Cardiopulmonary Bypass: 5A1221Z – Assistance with Cardiac Output using Extracorporeal Pump.
-
Diagnostic Cardiac Cath: 4A023N7 – Measurement of Cardiac Sampling and Pressure, Central Vascular.
Multiple Procedure Rule: Remember, all distinct procedures meeting criteria for reporting should be coded. The presence of a BAV does not make the TAVR a “combination” code; they are separate.
8. Device-Specific Coding: Mapping Valves to the ICD-10-PCS Table
Character 6 is where specific valve models are generalized into ICD-10-PCS categories. The coder must reference the device paperwork or hospital’s chargemaster linking the specific implant to the correct PCS device value. Here is a general guide:
| PCS Device Character | Device Value | General Description | Example Valve Platforms (Check Specific Models!) |
|---|---|---|---|
| K | Zooplastic Tissue | Tissue from an animal. | Many balloon-expandable valves (e.g., Edwards SAPIEN 3, SAPIEN XT – bovine pericardium). |
| L | Synthetic Substitute | Fully man-made, non-tissue. | Not typically used for current TAVR valves. |
| M | Zooplastic Tissue + Synthetic | A combination device. | Many self-expanding valves (e.g., Medtronic Evolut FX, Evolut PRO+ – porcine tissue on a nitinol frame). |
| N | Body Part + Synthetic | A human allograft with synthetic support. | Not typically used for TAVR. |
| R | Zooplastic Tissue + Body Part | A composite of animal and human tissue. | Rare for TAVR. |
Crucial Note: A “tissue” valve does not automatically mean “Zooplastic.” Some valves use bovine (cow) or porcine (pig) pericardium. The frame material (stainless steel, nitinol) determines if it is pure “Zooplastic” (K) or a combination “Zooplastic + Synthetic” (M). Always verify with device-specific mapping.
9. Comprehensive TAVR Coding Table: A Quick-Reference Guide
The table below provides a snapshot of common TAVR scenarios and their corresponding ICD-10-PCS codes. This is a learning tool; always validate against the official code set and documentation.
ICD-10-PCS Coding Scenarios for Common TAVR Procedures
| Procedure Description | Root Operation | ICD-10-PCS Code (Example) | Code Breakdown & Notes |
|---|---|---|---|
| Primary TAVR, Transfemoral, Bovine Pericardial Valve | Replacement | 02RF4KZ | 0:MedSurg, 2:Heart, R:Replacement, F:Aortic Valve, 4:Percutaneous, K:Zooplastic Tissue, Z:No Qualifier |
| Primary TAVR, Transapical, Porcine/Nitinol Valve | Replacement | 02RF0MZ | Approach is 0:Open (for transapical, transaortic). Device is M:Zooplastic+Synthetic. |
| Balloon Aortic Valvuloplasty (during same session) | Dilation | 02703ZZ | 0:MedSurg, 2:Heart, 7:Dilation, 0:Aortic Valve, 3:Percutaneous, Z:No Device, Z:No Qualifier. Code separately. |
| TAVR with Percutaneous Coronary Intervention (PCI) | Replacement + Dilation | 02RF4KZ + 02703ZZ + 02713DZ | The PCI (e.g., LAD stent) is coded from the Lower Arteries table (02713DZ: Dilation of LAD with Drug-Eluting Intraluminal Device). |
| TAVR requiring new Permanent Pacemaker | Replacement + Insertion(s) | 02RF4KZ + 02HK0JZ + 0JH808Z | PPM requires two codes: lead insertion into heart (02HK0JZ) and generator insertion into pocket (0JH808Z). |
| Valve-in-Valve TAVR (into failed surgical bioprosthesis) | Replacement | 02RF4KZ | Same root operation and code structure. The body part is still the “Aortic Valve,” which now includes the failed bioprosthesis. The approach/device vary. |
10. Compliance and Audit Focus: Avoiding Denials and Ensuring Accuracy
TAVR codes are high-dollar and high-audit-risk. Key areas of scrutiny:
-
Medical Necessity & Diagnosis Coding: The ICD-10-CM diagnosis is paramount. I35.0 (Nonrheumatic aortic (valve) stenosis) is primary. Supporting codes like heart failure (I50.9), syncope (R55), etc., must be present and correctly sequenced.
-
Device-Character Mismatch: Auditors will verify the PCS device character (K, M, etc.) matches the actual implant used. An incorrect device character is a common cause of technical denials.
-
Separate Procedure Reporting: Undercoding (missing BAV or PPM) loses revenue. Overcoding (separately coding integral steps like wire placement) creates compliance risk.
-
Approach Accuracy: Miscoding a transfemoral (percutaneous) as open, or vice versa, misrepresents the procedure’s complexity.
-
Documentation Linkage: The operative report must clearly support all coded elements: the procedure, approach, any devices implanted, and all concomitant procedures.
Audit-Proofing Tip: Create an internal “TAVR Coding Sheet” that surgeons and coders complete collaboratively for every case, documenting access, valve model/mapping, concomitant procedures, and complications.
11. The Future of Coding: TMVR, Sutureless Valves, and Emerging Tech
The principles learned here extend to other transcatheter therapies:
-
Transcatheter Mitral Valve Repair (TMVr) e.g., MitraClip: Root Operation is Restriction (02UG3JZ) – it reduces the orifice area, not replaces the valve.
-
Transcatheter Mitral Valve Replacement (TMVR): Would be Replacement of Mitral Valve (02RG…), facing similar device and access challenges.
-
Sutureless Surgical AVR: An open procedure, but the valve is “deployed” similar to TAVR. It is still an open Replacement (02RF0..).
-
Percutaneous Pulmonary Valve Replacement: Replacement in the “Pulmonary Valve” body part (02RG…).
Staying current with AHA Coding Clinic and CMS transmittals is non-negotiable as this field evolves.
12. Conclusion: The Art and Science of Procedural Coding
Accurate ICD-10-PCS coding for TAVR is a critical fusion of clinical understanding and precise procedural taxonomy. By mastering the root operation of Replacement, diligently mapping devices, and comprehensively capturing all procedural components, coding professionals ensure rightful reimbursement, support vital data analytics, and uphold the integrity of the patient’s medical record. In the fast-paced world of structural heart interventions, the coder’s role is not passive but integral—translating groundbreaking medicine into the standardized language that powers the healthcare ecosystem.
13. Frequently Asked Questions (FAQs)
Q1: What is the most common ICD-10-PCS code for a transfemoral TAVR?
A: While device-dependent, the most common structure is 02RF4KZ (Replacement of Aortic Valve with Zooplastic Tissue, Percutaneous Approach), often used for bovine pericardial balloon-expandable valves.
Q2: Do I code the removal of the native aortic valve during TAVR?
A: No. The native valve is not excised; it is displaced. The objective is Replacement (taking over function), not Excision or Resection. Only the root operation Replacement is coded.
Q3: How do I code a “Valve-in-Valve” TAVR done inside a failed surgical bioprosthesis?
A: Code it as a Replacement of the Aortic Valve (02RF…). The fact that it is within a previous prosthesis does not change the root operation or body part. The approach and device values are based on the current procedure.
Q4: What if the TAVR procedure is aborted after the balloon valvuloplasty?
A: Code the procedures that were completed (e.g., the Balloon Aortic Valvuloplasty, 02703ZZ). Do not code the TAVR replacement, as the valve was not implanted.
Q5: Where can I find the official device mapping for a specific Edwards or Medtronic valve?
A: The hospital’s chargemaster or materials management system should maintain the crosswalk between specific implantable device HCPCS codes (e.g., C2625) and the corresponding ICD-10-PCS device character. The manufacturer may provide guidance, but the hospital’s mapping is authoritative for coding.
14. Additional Resources and References
-
Official ICD-10-PCS Code Set and Guidelines: Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS). https://www.cms.gov/medicare/coding/icd10
-
AHA Coding Clinic for ICD-10-CM/PCS: The paramount authority for official coding advice. Search archives for “TAVR” and “transcatheter aortic valve.”
-
Society of Thoracic Surgeons (STS) / American College of Cardiology (ACC) TVT Registry: While clinical, provides essential context on procedure details and terminology.
-
American Health Information Management Association (AHIMA): Offers advanced coding credentials (CCA, CCS, CCS-P) and continuing education on procedural coding.
-
American Academy of Professional Coders (AAPC): Specialty credentials (CIRCC for cardiovascular) and resources for physician-based coding.
-
Manufacturer Technical Docs: Edwards Lifesciences and Medtronic provide detailed valve specifications useful for understanding device composition.
Date: December 12, 2025
Author: Medical Coding & Cardiovascular Procedural Expert
Disclaimer: *This article is intended for educational and informational purposes for healthcare professionals, specifically medical coders and billing specialists. It is not a substitute for official coding guidelines, payer policies, or clinical advice. Always consult the most current ICD-10-PCS code set, AHA Coding Clinic, and provider documentation for definitive coding decisions.*





