Imagine trying to breathe through a straw that is partially pinched shut. For millions of individuals suffering from a deviated nasal septum, this sensation is a daily reality. The nose, our primary gateway for respiration, is far more than a passive organ of smell; it is a sophisticated, dynamic structure that humidifies, filters, and warms the air we breathe before it reaches our delicate lungs. At the core of this structure lies the nasal septum, a partition that, when straight and true, allows for laminar, effortless airflow. But when this septum is deviated—crooked, bent, or obstructing—it can lead to a cascade of problems: chronic nasal congestion, recurrent sinus infections, sleep-disordered breathing, facial pain, and a significant diminishment in quality of life.
Septoplasty stands as the cornerstone surgical solution to this pervasive problem. It is a functional procedure designed not to change the external appearance of the nose, but to reconstruct its internal architecture, restoring the patent airway that is so vital to our well-being. For the medical coder, accurately representing this procedure in the digital language of healthcare is paramount. The transition to the ICD-10-PCS (International Classification of Diseases, Tenth Revision, Procedure Coding System) has transformed this task from a simple look-up exercise into a nuanced, analytical process. Understanding septoplasty in ICD-10-PCS requires a deep dive into the surgeon’s intent, the specific anatomical structures manipulated, and the technical approach employed. This article serves as a masterclass in that analytical process. We will journey from the basic anatomy of the nose, through the intricate steps of the surgery, and into the granular details of building a precise and compliant PCS code, empowering you with the knowledge to code septoplasty with confidence and accuracy.
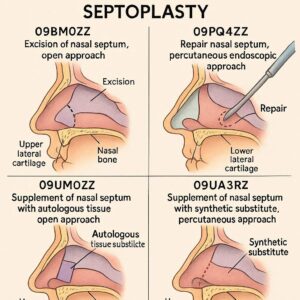
ICD-10-PCS for Septoplasty
2. The Foundation: Understanding Nasal Anatomy and the Deviated Septum
Before a single line of operative report can be interpreted or a single PCS character assigned, a solid grasp of the relevant anatomy is non-negotiable. The nasal cavity is a complex space, and the septum is its central supporting wall.
The Nasal Septum: The Central Partition
The nasal septum is a structure composed of both bony and cartilaginous components, covered by a specialized mucous membrane called the mucoperichondrium and mucoperiosteum.
-
Septal Cartilage: This is the primary, flexible anterior portion of the septum. It forms the support for the lower two-thirds of the nasal dorsum (the bridge) and the columella (the tissue between the nostrils).
-
Perpendicular Plate of the Ethmoid Bone: A thin, flat bone that extends superiorly from the septal cartilage, forming the upper part of the septum. It is a crucial structure, as it is attached to the skull base.
-
Vomer Bone: A trapezoidal bone that forms the postero-inferior section of the septum, articulating with the perpendicular plate and the maxillary and palatine bones.
These three components together form the septal partition. A key anatomical concept for the coder is the mucoperichondrial/mucoperiosteal flap. During a septoplasty, the surgeon carefully elevates this vascularized tissue layer off the underlying cartilage and bone. This flap is preserved and later repositioned, acting as a natural biological dressing that facilitates healing.
What is a Deviated Septum?
A deviated septum occurs when the nasal septum is displaced from the midline, causing a narrowing of one or both nasal passages. Deviations can be congenital (present from birth) or acquired, most commonly from trauma such as a broken nose. Deviations can take various forms:
-
Anterior Deviation: Often more symptomatic as it occurs in the main airflow pathway.
-
Spurs: Sharp, bony projections that can form at the junction of the vomer and ethmoid bones.
-
C-Shaped or S-Shaped Deviations: Curvatures that can obstruct one or both sides of the nose.
Adjacent Structures: The Turbinates
While not part of the septum, the inferior turbinates are intimately involved in nasal airflow and are frequently addressed during septoplasty. These are scroll-like bones covered in erectile tissue that project into the nasal cavity. They help humidify and filter air. In response to a deviated septum, the inferior turbinate on the wider, opposite side often becomes enlarged or hypertrophied to fill the space (a condition known as compensatory hypertrophy). Failure to address this hypertrophy during septoplasty can lead to a suboptimal surgical outcome, as the enlarged turbinate can continue to cause obstruction.
3. The Procedural Spectrum: From Simple Septoplasty to Septorhinoplasty
The term “septoplasty” can encompass a range of techniques, from a straightforward correction to a complex reconstruction involving multiple grafts. The coder must discern the specific type of procedure performed.
Classic Septoplasty (SMR vs. Modern Septoplasty)
Historically, the procedure was known as a Submucous Resection (SMR), which involved the removal of large portions of the deviated cartilage and bone. The modern septoplasty is a more conservative and reconstructive procedure. The goal is to preserve as much of the native septal cartilage and bone as possible. The surgeon makes an incision, elevates the mucoperichondrial flaps, identifies the deviated segments, and then either repositions, scores, shaves, or removes only the most severely deviated portions. The key is to straighten the septum while maintaining its structural support function.
Endoscopic Septoplasty
This is a minimally invasive variation where the surgeon uses a nasal endoscope (a thin, rigid tube with a camera and light) for visualization. The endoscope provides magnified, illuminated views of the deeper parts of the septum, allowing for precise correction of posterior deviations and spurs with smaller incisions. The PCS coding for an endoscopic septoplasty differs from an open approach in a single character—the Approach.
Septoplasty with Turbinate Reduction
As mentioned, this is an extremely common combination. The turbinate reduction (or turbinoplasty) is a separate procedure but is performed during the same operative session to comprehensively treat nasal obstruction. Techniques for turbinate reduction include:
-
Resection: Partial removal of the turbinate bone and soft tissue.
-
Coblation/Radiofrequency Ablation: Using energy to shrink the underlying soft tissue.
-
Microdebrider-Assisted Turbinoplasty: Using a powered instrument to remove soft tissue while preserving the mucosa.
The coder must determine if the turbinate procedure constitutes a separate root operation, such as Excision or Destruction.
Septorhinoplasty
This is a combined functional and cosmetic procedure. A septoplasty is performed to correct the internal deviation and improve breathing, while a rhinoplasty is performed to change the external shape and appearance of the nose. This is a critical distinction in PCS coding, as the two components target different body parts and often involve different root operations. A septorhinoplasty will typically require two separate PCS codes.
4. Introduction to ICD-10-PCS: A Paradigm Shift from ICD-9-CM
For coders trained in the era of ICD-9-CM, the shift to ICD-10-PCS can be jarring. ICD-9-CM Volume 3 used a largely numeric system with codes that often represented a specific procedure name (e.g., 21.5 for septoplasty). ICD-10-PCS is fundamentally different. It is a multi-axial, seven-character alphanumeric system where each character has a specific meaning. There are no “pre-defined” procedure codes; instead, the coder builds a code based on the details of the operative report.
The Seven Characters of an ICD-10-PCS Code:
Each character in a PCS code represents a specific aspect of the procedure:
-
Section: The broadest category (e.g., Medical and Surgical).
-
Body System: The general physiological system (e.g., Ear, Nose, Sinus).
-
Root Operation: The objective or intent of the procedure—this is the most critical conceptual element.
-
Body Part: The specific anatomical site.
-
Approach: The technique used to reach the site.
-
Device: Any device that remains after the procedure.
-
Qualifier: Adds additional information about the procedure.
This structure allows for immense specificity. For example, instead of one code for “septoplasty,” ICD-10-PCS can generate different codes for an open approach versus an endoscopic approach, and for a procedure that uses a graft versus one that does not.
5. Deconstructing the Septoplasty PCS Code: The Seven Characters
Let’s build a septoplasty code from the ground up, character by character.
Section: 0 – Medical and Surgical
This is straightforward. A septoplasty is a surgical procedure, so it always falls into Section 0.
Body System: 9 – Ear, Nose, Sinus
The nasal septum is part of the nasal cavity, which is classified under the “Ear, Nose, Sinus” body system. Therefore, the second character is 9.
Root Operation: What is the Surgeon Actually Doing?
This is the heart of PCS coding and the source of most confusion for septoplasty. The official definition of the root operation is key. The most common root operations for septoplasty are Alteration, Repair, and Resection.
-
Root Operation: Alteration
-
Definition: Modifying the natural anatomical structure of a body part without affecting its function. This does not mean the function is unaffected; it means the procedure’s purpose is purely aesthetic.
-
Application to Septoplasty: Alteration is used for cosmetic rhinoplasty. If the procedure is performed only to change the appearance of the nose and there is no functional goal, Alteration is the correct root operation. It is not typically used for a functional septoplasty.
-
-
Root Operation: Repair
-
Definition: Restoring, to the extent possible, a body part to its normal anatomical structure and function. This includes putting parts back in their normal alignment.
-
Application to Septoplasty: This is the most appropriate and commonly used root operation for a standard, functional septoplasty. The goal is to straighten the deviated septum (restore normal anatomy) to improve nasal breathing (restore function). The actions of excising a small piece of cartilage, scoring it to allow it to straighten, or fracturing and repositioning it all fall under the umbrella of “restoring to normal alignment.” Therefore, for a pure functional septoplasty, the root operation is Repair.
-
-
Root Operation: Resection
-
Definition: Cutting out or off, without replacement, all of a body part.
-
Application to Septoplasty: This is the root operation for the old Submucous Resection (SMR) technique, where a significant portion of the septal cartilage and/or bone is removed and not replaced. In a modern septoplasty, if a sizable piece of septum is removed and no graft is placed, Resection may be appropriate. However, Repair is generally preferred if any reconstructive effort is made.
-
Conclusion on Root Operation: For the vast majority of contemporary functional septoplasties documented in modern operative reports, the correct root operation is Repair.
Body Part: Pinpointing the Anatomical Site
The body part character specifies what is being repaired. For a septoplasty, the choices are:
-
J – Nasal Septum: This is the default and most common choice. It represents the entire septal structure (cartilage and bone).
-
0 – Nasal Mucosa: This would only be used if the procedure was exclusively on the mucous membrane covering, such as a simple release of adhesions (synechiae), not for a standard septoplasty which involves the underlying cartilage/bone.
For a standard septoplasty, the body part character is J.
Approach: How Access is Achieved
The approach describes the technique used to reach the operative site. For septoplasty, the common approaches are:
-
0 – Open: The surgeon makes an external incision on the columella (the skin between the nostrils) to gain access to the septal framework. This is common in septorhinoplasty.
-
3 – Percutaneous: The surgeon makes an incision through the skin. This is not typical for an isolated septoplasty.
-
7 – Via Natural or Artificial Opening: The surgeon enters through a natural opening—in this case, the nostril (nares). This is the approach for a standard, non-endoscopic septoplasty performed through a Killian or hemitransfixion incision inside the nose.
-
8 – Via Natural or Artificial Opening Endoscopic: The surgeon enters through the nostril but uses an endoscope for visualization. This is the approach for an endoscopic septoplasty.
The correct approach is determined by the operative report’s description. For a standard internal septoplasty, it’s 7. For an endoscopic one, it’s 8.
Device: Not Typically Used in Septoplasty
This character identifies a device that remains in the body after the procedure. In a septoplasty, devices like sutures or splints are temporary and are not coded. If a permanent implant (e.g., a synthetic septal button) were used, it would be coded here, but this is rare. For almost all septoplasties, the device character is Z – No Device.
Qualifier: The Crucial Detail for Grafts
The qualifier provides additional information. In the context of Repair of the Nasal Septum, the qualifier indicates whether a graft was used.
-
Z – No Qualifier: Used when no graft is placed.
-
7 – Autologous Tissue Substitute: Used when tissue from the patient’s own body is used as a graft. In septoplasty, this is most commonly a piece of septal cartilage or bone that was removed, sculpted, and then replaced as a graft to support the straightened septum. It could also be ear cartilage or a rib graft.
-
8 – Nonautologous Tissue Substitute: Used when donor tissue (allograft, such as cadaveric rib cartilage) or synthetic material (e.g., PDS plate) is used as a graft.
If the operative report states “a piece of harvested septal cartilage was used as a spreader graft,” the qualifier would be 7.
6. Common Coding Scenarios with Practical Examples
Let’s apply our knowledge to real-world examples.
Scenario 1: Standard Open Septoplasty
-
Op Report Snippet: “…a left hemitransfixion incision was made. Mucoperichondrial flaps were elevated. A significant cartilaginous deviation was identified in the caudal septum. The deviated segment was sharply excised, scored on the concave side, and then replaced. The septum was noted to be in the midline. Mucoperichondrial flaps were re-approximated. Silastic splints were placed.”
-
Code Building:
-
Section/Body System: 0 / 9 (Medical & Surgical / Ear, Nose, Sinus)
-
Root Operation: Repair (restoring the septum to midline alignment)
-
Body Part: Nasal Septum (J)
-
Approach: Via Natural or Artificial Opening (7) – through the nostril.
-
Device: No Device (Z)
-
Qualifier: No Qualifier (Z) – The excised cartilage was scored and replaced, but it was not taken from a separate donor site; it was a repositioning of the native septum. This does not typically qualify as a “graft” in the PCS sense.
-
-
Final PCS Code: 0C9J7ZZ – Repair of Nasal Septum, Via Natural or Artificial Opening.
Scenario 2: Endoscopic Septoplasty
-
Op Report Snippet: “…the 0-degree endoscope was introduced. A posterior septal spur was identified. Using endoscopic instrumentation, the mucoperiosteum was elevated off the spur, and the bony spur was resected with a punch forceps. The septum was straightened.”
-
Code Building:
-
Section/Body System: 0 / 9
-
Root Operation: Repair (the goal was to straighten the septum by resecting the spur)
-
Body Part: Nasal Septum (J)
-
Approach: Via Natural or Artificial Opening Endoscopic (8)
-
Device: No Device (Z)
-
Qualifier: No Qualifier (Z)
-
-
Final PCS Code: 0C9J8ZZ – Repair of Nasal Septum, Via Natural or Artificial Opening Endoscopic.
Scenario 3: Septoplasty with Turbinate Resection
-
Op Report Snippet: “…septoplasty was performed as described above (via open approach). Attention was turned to the inferior turbinates, which were hypertrophied bilaterally. A microdebrider was used to resect the anterior one-third of the inferior turbinate soft tissue and bone bilaterally.”
-
Code Building: This scenario requires two PCS codes.
-
Code 1 for Septoplasty: 0C9J7ZZ (same as Scenario 1).
-
Code 2 for Turbinates:
-
Root Operation: Excision (cutting out all of a portion of the turbinate).
-
Body Part: The PCS table for the Ear, Nose, Sinus system has specific body part values for turbinates. “Inferior Turbinate, Left” (value 1) and “Inferior Turbinate, Right” (value 2). Since the procedure was bilateral, you need two codes: one for the left and one for the right.
-
Approach: Via Natural or Artificial Opening (7) or Endoscopic (8). The report doesn’t specify an endoscope for the turbinate part, but it’s often implied. If not specified, default to 7. Let’s assume 7.
-
Device/Qualifier: Z / Z.
-
-
Final PCS Codes: 0C9J7ZZ (Septoplasty), 0CBT7ZZ (Excision of Left Inferior Turbinate), 0CBS7ZZ (Excision of Right Inferior Turbinate).
-
Scenario 4: Septorhinoplasty with Grafting
-
Op Report Snippet: “…an open approach was utilized via a transcolumellar incision. The septal cartilage was exposed. A significant dorsal deviation was corrected. A piece of septal cartilage was harvested, carved, and used as a columellar strut graft to support the nasal tip. The nasal bones were then osteotomized to narrow the nasal dorsum.”
-
Code Building: This is a combined procedure requiring two codes.
-
Code 1 for Functional Septoplasty with Graft:
-
Root Operation: Repair (of the septum)
-
Body Part: Nasal Septum (J)
-
Approach: Open (0) – due to the transcolumellar incision.
-
Device: Z
-
Qualifier: Autologous Tissue Substitute (7) – because septal cartilage was harvested and used as a graft.
-
Code: 0C9J0Z7
-
-
Code 2 for Cosmetic Rhinoplasty:
-
Root Operation: Alteration (the osteotomies to narrow the dorsum are for cosmetic appearance)
-
Body Part: Nasal Bone. The PCS table has “Nasal Bone, Left” (5) and “Nasal Bone, Right” (6). Since osteotomies are bilateral, code both.
-
Approach: Open (0)
-
Device/Qualifier: Z / Z
-
Code: 0W5F0ZZ (Alteration of Left Nasal Bone), 0W5G0ZZ (Alteration of Right Nasal Bone)
-
-
7. The Critical Distinction: Septoplasty vs. Rhinoplasty in PCS
This is the single most important conceptual hurdle. The difference lies entirely in the Root Operation, which is determined by the objective of the procedure.
-
Septoplasty (Functional): Root Operation = Repair. The goal is to restore function by correcting a deviated septum.
-
Rhinoplasty (Cosmetic): Root Operation = Alteration. The goal is to change appearance.
When a procedure is a Septorhinoplasty, you are performing both a functional and a cosmetic component. Therefore, you must code both the Repair of the Nasal Septum and the Alteration of the Nasal Bones and/or other external nasal structures. Using only one code is inaccurate and fails to represent the full work performed.
8. Tables for Clarity: PCS Components for Nasal Procedures
ICD-10-PCS Root Operations for Nasal Procedures
| Root Operation | PCS Code | Definition | Common Nasal Procedure Example |
|---|---|---|---|
| Alteration | 0W5F-0ZZ / 0W5G-0ZZ | Modifying the anatomical structure for aesthetic purposes | Cosmetic Rhinoplasty (narrowing nasal bones, refining tip) |
| Repair | 0C9J- – – | Restoring a body part to its normal anatomical structure/function | Functional Septoplasty (straightening a deviated septum) |
| Resection | 0C9J- – – | Cutting out or off all of a body part | Submucous Resection (SMR) of the septum |
| Excision | 0CBT- – – / 0CBS- – – | Cutting out only a portion of a body part | Partial Turbinectomy (removing part of the inferior turbinate) |
| Destruction | 0CBT- – – / 0CBS- – – | Physical eradication of a body part | Coblator ablation of turbinate tissue |
| Dilation | 0C9N- – – | Expanding an orifice | Balloon Sinuplasty (dilation of a sinus ostium) |
Building the ICD-10-PCS Code for Septoplasty (0C9J—)
| Character 1 | Character 2 | Character 3 | Character 4 | Character 5 | Character 6 | Character 7 |
|---|---|---|---|---|---|---|
| Section | Body System | Root Operation | Body Part | Approach | Device | Qualifier |
| 0 Medical and Surgical | 9 Ear, Nose, Sinus | C Repair | J Nasal Septum | 0 Open 3 Percutaneous 7 Via Natural/Artificial Opening 8 Via Natural/Artificial Opening Endoscopic |
Z No Device | Z No Qualifier 7 Autologous Tissue Substitute 8 Nonautologous Tissue Substitute |
9. Navigating Coding Challenges and Pitfalls
-
Insufficient Documentation: The op report must clearly state the approach (open vs. endoscopic), the specific structures worked on (septum, turbinates, bones), and whether grafts were used. If it’s unclear, a physician query is essential.
-
Misinterpreting the Root Operation: Do not default to “Resection” just because cartilage was removed. If the overall goal was to straighten and repair, “Repair” is the correct choice.
-
Bilateral Procedures: In PCS, if there are separate body part values for left and right (like turbinates or nasal bones), you must code each side separately.
-
Assuming “Endoscopic”: Do not assume an approach. If the surgeon does not explicitly mention the use of an endoscope for the septoplasty, you cannot code an endoscopic approach (8).
10. The Importance of Documentation and Physician Queries
The accuracy of your PCS code is directly dependent on the clarity of the operative report. Encourage surgeons to be specific. A well-documented report should include:
-
Indication: The functional problem (e.g., “nasal obstruction due to deviated septum”).
-
Incision: The exact type and location (e.g., “left hemitransfixion incision,” “transcolumellar incision”).
-
Technique: “Mucoperichondrial flaps elevated,” “deviated segment excised/scored/repositioned,” “bony spur resected.”
-
Visualization: Explicitly state “using a 0-degree nasal endoscope” if performed endoscopically.
-
Grafts: “A 2×1 cm piece of septal cartilage was harvested and carved into a spreader graft.”
-
Additional Procedures: Clearly describe any work on turbinates, nasal bones, or sinuses.
If any of these elements are missing or ambiguous, a formal query to the physician is the only compliant path to obtaining clarification and ensuring an accurate code.
11. Conclusion: Synthesizing Knowledge for Precision Coding
Accurate ICD-10-PCS coding for septoplasty hinges on a deep understanding of nasal anatomy and surgical intent. The coder must meticulously analyze the operative report to select the correct root operation—most often Repair for functional goals. The specific approach, use of grafts, and any concurrent procedures like turbinate resections must be captured with distinct characters or separate codes, building a complete and compliant picture of the patient’s surgical encounter.
12. Frequently Asked Questions (FAQs)
Q1: What is the most common ICD-10-PCS code for a standard functional septoplasty?
A1: The most common code is 0C9J7ZZ (Repair of Nasal Septum, Via Natural or Artificial Opening). This assumes a functional goal (Repair), an internal incision (Approach 7), and no graft.
Q2: How do I code a septoplasty if the surgeon uses the patient’s own septal cartilage as a graft?
A2: You would use the same root operation (Repair) and body part (Nasal Septum), but the qualifier would change to 7 for Autologous Tissue Substitute. The code would be 0C9J0Z7 if done via an open approach or 0C9J8Z7 if done endoscopically.
Q3: Is it ever correct to use the root operation “Resection” for a septoplasty?
A3: Yes, but it is less common. If the operative report describes a classic Submucous Resection (SMR) where large portions of the septum are removed without any reconstructive effort (e.g., scoring, repositioning, grafting), then Resection may be appropriate. In modern practice, Repair is almost always the better fit.
Q4: How many codes do I need for a septoplasty with bilateral inferior turbinate reductions?
A4: You will need a minimum of three codes: one for the septoplasty (e.g., 0C9J7ZZ), one for the left turbinate reduction (e.g., 0CBT7ZZ for Excision), and one for the right turbinate reduction (0CBS7ZZ).
Q5: What is the fundamental PCS difference between a septoplasty and a rhinoplasty?
A5: The root operation. A functional septoplasty is coded to Repair. A cosmetic rhinoplasty is coded to Alteration. A septorhinoplasty requires both a Repair code for the septum and an Alteration code for the external nasal structures.
Date: November 19, 2025
Author: Medical Coding Specialist
Disclaimer: This article is intended for educational purposes and to illustrate the principles of ICD-10-PCS coding. It is not a substitute for the official ICD-10-PCS guidelines, code books, or professional coding advice. Medical coders must use the current year’s official resources and consult with their compliance departments for final coding decisions. The procedural descriptions are generalized; actual techniques can vary by surgeon and patient circumstance.





