In the high-stakes realm of neurosurgery, where millimeters matter and timing is paramount, the clarity of clinical documentation finds its parallel in the precision of medical coding. A subdural hemorrhage (SDH), a potentially life-threatening collection of blood on the brain’s surface, demands swift surgical intervention. But the story doesn’t end in the operating room. Every incision, every approach, every device used must be meticulously translated into a universal alphanumeric language: the ICD-10-PCS (Procedure Coding System). This translation is not mere administrative paperwork; it is the linchpin connecting patient care to data analytics, quality reporting, and hospital reimbursement. An inaccurately coded procedure can obscure clinical realities, skew national health statistics, and jeopardize financial stability. This comprehensive guide, crafted exclusively for the discerning professional, ventures beyond simplistic code lookup. It delves into the anatomical, procedural, and coding intricacies of surgical interventions for subdural hemorrhage, empowering coders, clinicians, and students to navigate this complex landscape with confidence and expertise. Prepare for a detailed journey through the layers of the meninges, the philosophy of root operations, and the art of building the perfect 7-character code.
ICD-10-PCS for Subdural Hemorrhage
2. Anatomy and Pathology: Understanding the Subdural Space and Hemorrhage
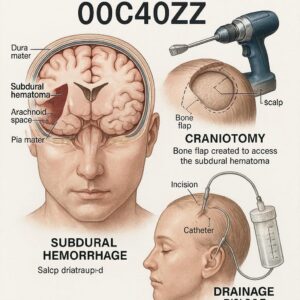
To code a procedure accurately, one must first understand the anatomy and the disease process. The meninges are the three protective membranes surrounding the brain and spinal cord: the dura mater (outermost, tough layer), the arachnoid mater (middle, web-like layer), and the pia mater (innermost, delicate layer). The subdural space is a potential space between the dura mater and the arachnoid mater. It is not a natural cavity but can be pathologically expanded by the accumulation of blood.
A subdural hemorrhage occurs when bridging veins—which traverse this potential space from the brain’s surface to the dural sinuses—tear, often due to traumatic acceleration-deceleration forces. This is classically seen in falls or assaults, especially in the elderly and in chronic alcoholics, where brain atrophy may have already stretched these veins. SDHs are categorized by their chronicity:
-
Acute SDH: Presents within 72 hours of injury. Blood is fresh, hyperdense on CT scan, and often requires urgent evacuation.
-
Subacute SDH: Presents between 3 days and 3 weeks. A mixture of clotted and liquefying blood.
-
Chronic SDH: Develops over weeks to months. The blood has liquefied into a serosanguineous fluid, often encapsulated by neomembranes. It may result from a minor, forgotten trauma.
The pathology dictates the surgery. An acute SDH is often a solid clot requiring removal, while a chronic SDH may be irrigated and drained. This fundamental clinical distinction directly informs the choice of the most critical component of an ICD-10-PCS code: the Root Operation.
3. The ICD-10-PCS Framework: A Primer on the 7-Character System
ICD-10-PCS is a completely different system from ICD-10-CM (diagnosis coding). It is built on a logical, multi-axial structure where each character has a specific meaning, independent of the others. Every code is seven characters long, and each character represents a specific aspect of the procedure.
The 7 Characters of an ICD-10-PCS Code:
-
Section: The broadest category (e.g., Medical and Surgical, Obstetrics).
-
Body System: The general physiological system (e.g., Central Nervous System).
-
Root Operation: The objective of the procedure—what the physician did.
-
Body Part: The specific site where the procedure was performed.
-
Approach: The technique used to reach the site (e.g., open, percutaneous).
-
Device: Any device that remains after the procedure.
-
Qualifier: An additional attribute for further specificity.
For subdural hemorrhage procedures, we operate almost exclusively within the Medical and Surgical Section (0) and the Central Nervous System Body System (0). Our coding quest revolves around accurately defining characters 3 through 7.
4. Deconstructing the Root Operation: “Drainage” vs. “Extirpation” vs. “Resection”
This is the heart of SDH coding. Misidentifying the root operation is the most significant error a coder can make. The official definitions from the ICD-10-PCS Reference Manual are paramount:
-
Drainage (Root Operation 0): “Taking or letting out fluids and/or gases from a body part.” The key concept is fluid. This is the most common root operation for chronic SDH, where the hematoma has liquefied. The surgeon makes a hole (burr hole or small craniotomy) and irrigates and drains the fluid collection. No solid material is actively “cut out.”
-
Extirpation (Root Operation B): “Taking or cutting out solid matter from a body part.” The key concept is solid matter. This is typically used for acute or subacute SDH, where a solid or semi-solid clot is present. The surgeon removes the clot from the subdural space. The clot is not a body part itself; it is solid matter within a body part (the intracranial space or meninges).
-
Resection (Root Operation T): “Cutting out or off, without replacement, all of a body part.” This is RARELY applicable for SDH. It would only be used if a surgeon removed a portion of the dura mater itself (e.g., for a dural biopsy or because it was necrotic). It is not used for removal of the hematoma.
Clinical Documentation Clue: The operative report’s verb is crucial. If the surgeon describes “evacuating a liquid chronic hematoma,” “irrigating until clear fluid returns,” or “placing a drain for drainage,” think Drainage (0). If the report describes “removing an organized clot,” “evacuating a solid acute hematoma,” or “extirpating the hematoma,” think Extirpation (B).
5. The Body Part Conundrum: Meninges, Intracranial, or Focal?
Character 4 specifies the Body Part. For SDH procedures, the main choices are in the Central Nervous System table:
-
Meninges: This refers to the dura, arachnoid, and pia mater as a combined structure. It is used when the procedure is focused on the meningeal layers themselves (e.g., a dural repair, a biopsy).
-
Intracranial Space: This is a cavity or potential space within the head. The subdural space is an intracranial space. This is the most appropriate and commonly used body part for SDH drainage or extirpation, as the hematoma occupies that space.
-
More specific sites (e.g., Frontal, Temporal, Parietal): These are used for procedures on the brain tissue itself, not the space around it. They would be inappropriate for a routine SDH evacuation.
Coding Consensus: For standard evacuation of a subdural hematoma, “Intracranial Space” is the preferred and most anatomically precise body part value.
6. The Surgical Approach: From Open Craniotomy to Percutaneous Endoscopy
Character 5 defines the Approach—how the surgeon accessed the operative site.
-
Open (0): The classic surgical approach. The surgeon makes a scalp incision, removes a bone flap (craniotomy) to expose a large area of the dura, opens the dura, and performs the procedure under direct vision. Used for large, acute SDHs or complex cases.
-
Percutaneous (3): Access is via a needle-puncture or small stab wound. For SDH, this is the burr hole approach. A small hole is drilled through the skull, the dura is opened, and the hematoma is drained or irrigated. Common for chronic SDHs.
-
Percutaneous Endoscopic (4): A burr hole is made, but a small endoscope (camera) is introduced to visualize the space, assist in breaking up loculations, and ensure adequate evacuation. Increasingly common.
-
External (X): Used only for procedures performed on the surface of the body. Not applicable for SDH evacuation.
7. Device Character: The Critical Role of Drainage Catheters and Monitoring
Character 6 identifies any device that remains after the procedure. For SDH, this is almost always about drainage.
-
No Device (Z): No device is left in place. The hematoma is evacuated, and the wound is closed.
-
Drainage Device (0): A subdural drain (like a Jackson-Pratt or similar soft catheter) is left in the subdural or epidural space postoperatively to drain residual fluid or blood. This is a very common practice, especially for chronic SDH, to prevent re-accumulation.
-
Monitoring Device (Pressure), Intracranial (1): An intracranial pressure (ICP) monitor or bolt is placed. This may be done in conjunction with an SDH evacuation if the patient has severe brain swelling or is at high risk for elevated ICP.
Critical Note: If a drain is placed, code Drainage Device (0). This is a key differentiator that impacts coding accuracy.
8. The Qualifier: A Deeper Look into Substance and Purpose
Character 7, the Qualifier, provides final specificity. For the Central Nervous System body system, the most relevant qualifier for SDH is:
-
Diagnostic (X): The procedure is performed primarily to obtain a sample or visualize for diagnostic purposes.
-
No Qualifier (Z): A therapeutic procedure.
-
Other Qualifier (Y): Used for specific scenarios like stereotactic guidance (which is more often captured in the Approach character for other body systems).
For SDH evacuation, unless it’s explicitly a diagnostic burr hole (rare), the qualifier is typically No Qualifier (Z).
9. Step-by-Step Coding Scenarios: From Acute to Chronic, Simple to Complex
Let’s apply our knowledge to real-world examples.
Scenario 1: Chronic Subdural Hematoma, Burr Hole Drainage with Drain Placement.
-
Op Report: “Under general anesthesia, a right frontal burr hole was created. The dura was coagulated and opened. Dark, liquid chronic subdural hematoma was drained under pressure. The cavity was irrigated with warm saline until clear. A subdural drain was placed and brought out through a separate stab incision. The wound was closed.”
-
Code Build:
-
Section: 0 (Medical and Surgical)
-
Body System: 0 (Central Nervous System)
-
Root Operation: 9 (Drainage) – Liquid was let out.
-
Body Part: 0 (Intracranial Space) – The subdural space is an intracranial space.
-
Approach: 3 (Percutaneous) – Burr hole technique.
-
Device: 0 (Drainage Device) – A subdural drain was left in place.
-
Qualifier: Z (No Qualifier) – Therapeutic procedure.
-
-
Final ICD-10-PCS Code: 00903ZX
Scenario 2: Acute Subdural Hematoma, Craniotomy for Evacuation of Solid Clot, No Drain.
-
Op Report: “A large left frontotemporoparietal craniotomy was performed. The dura was tense and blue. Upon opening the dura, a large solid acute subdural clot was encountered. The clot was meticulously extirpated using suction and irrigation. The brain relaxed. The dura was closed primarily. The bone flap was replaced.”
-
Code Build:
-
Root Operation: B (Extirpation) – Solid matter (clot) was taken out.
-
Body Part: 0 (Intracranial Space)
-
Approach: 0 (Open) – Full craniotomy.
-
Device: Z (No Device) – No drain mentioned.
-
Qualifier: Z (No Qualifier)
-
-
Final ICD-10-PCS Code: 00B00ZZ
Scenario 3: Complex Case – Acute SDH Evacuation with ICP Monitor Placement.
-
Op Report: “…evacuated the acute subdural hematoma via craniotomy. Given the significant cerebral edema, an intracranial pressure monitoring bolt was placed in the right frontal region.”
-
Coding Logic: This requires two codes.
-
Code 1: Evacuation of SDH. 00B00ZZ (Extirpation of intracranial space via open approach).
-
Code 2: Placement of ICP monitor. This is a different root operation. The root operation is Insertion (H) – putting in a monitoring device. The body part is Intracranial Space (0), Approach is Open (0), Device is Monitoring Device, Pressure, Intracranial (1), Qualifier is Z. 00H002Z.
-
10. The Pitfalls and Challenges: Common Errors in SDH Coding
-
Confusing Drainage with Extirpation: The #1 error. Relying on the lay term “evacuation” without reading the pathology report or op note description of the hematoma’s consistency.
-
Misidentifying the Body Part: Using “Brain” or “Cerebral Meninges” instead of the more accurate “Intracranial Space.”
-
Overlooking the Device: Failing to code for a drain (Device character 0) is a common oversight that can impact DRG assignment.
-
Incorrect Approach for Burr Hole: Coding a burr hole as “Open” instead of “Percutaneous.”
-
Not Coding All Procedures: Missing the separate code for an ICP monitor or a dural repair.
11. Linking Coding to DRGs and Reimbursement
Accurate ICD-10-PCS coding directly determines the Medicare Severity-Diagnosis Related Group (MS-DRG). For SDH, key DRGs include:
-
DRG 023: Craniotomy for Trauma with MCC (Major Complication/Comorbidity)
-
DRG 024: Craniotomy for Trauma with CC (Complication/Comorbidity)
-
DRG 025: Craniotomy for Trauma without CC/MCC
-
DRG 033: Other Disorders of Nervous System with MCC/CC (often captures burr hole procedures)
The distinction between an “Open” approach (craniotomy, DRGs 023-025) and a “Percutaneous” approach (burr hole, often DRG 033) has a substantial financial impact for the hospital. Accurate coding of the device and any complications is also critical for correct DRG assignment and reimbursement.
12. The Future of Procedural Coding: A Glimpse Beyond ICD-10-PCS
ICD-10-PCS, while robust, is not the final evolution. The medical coding community is actively preparing for the eventual transition to ICD-11-PCS and other data standards. The focus is shifting towards greater granularity for new technologies (e.g., specific robotic approach values) and better alignment with electronic health records and clinical terminologies like SNOMED CT. The fundamental skills of analyzing an operative report, understanding anatomy, and applying precise definitions will remain the coder’s most valuable assets in any future system.
13. Conclusion
Mastering ICD-10-PCS coding for subdural hemorrhage requires a synthesis of anatomical knowledge, surgical understanding, and meticulous attention to the definitions within the coding system. It moves far beyond simple lookup, demanding a careful analysis of the operative report to correctly identify the root operation, approach, and any devices used. Precision in this process ensures data integrity, supports quality patient care analytics, and facilitates appropriate reimbursement, solidifying the medical coder’s role as an essential member of the healthcare team.
14. Frequently Asked Questions (FAQs)
Q1: The surgeon documented “evacuation of a subdural hematoma.” Is that Drainage or Extirpation?
A: You cannot determine from that phrase alone. You must read the operative report’s description of the hematoma (e.g., “liquid chronic hematoma” vs. “organized solid clot”) and the details of the procedure (e.g., “irrigated” vs. “removed the clot”) to decide between Drainage and Extirpation.
Q2: What if the surgeon performs both a craniotomy for an acute SDH and places a drain?
A: If the drain is placed in the subdural space at the end of the extirpation procedure, you only need one code. The Device character (6th character) would be 0 (Drainage Device). The code would be 00B00Z0.
Q3: How do I code a bilateral subdural hematoma evacuation?
A: ICD-10-PCS has laterality. The Intracranial Space body part has values for 0- Intracranial Space, right, 1- Intracranial Space, left, and M- Intracranial Space, bilateral. If a single procedure addresses both sides (e.g., bilateral burr holes), use the bilateral body part value. If two distinct procedures are performed (e.g., a left craniotomy and a separate right burr hole), you would assign two codes.
Q4: Is there a code for “twist drill craniostomy” or “mini-craniotomy”?
A: These are both considered Percutaneous (3) approaches, as they involve a small hole or opening rather than a full bone flap removal. The specific terminology the surgeon uses is less important than the conceptual approach.
Q5: Where can I find official updates and guidance on ICD-10-PCS?
A: The definitive sources are the AHA’s *Coding Clinic for ICD-10-CM/PCS* (quarterly publication) and the official guidelines published by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS).
15. Additional Resources
-
Centers for Medicare & Medicaid Services (CMS) ICD-10-PCS Files: https://www.cms.gov/medicare/coding/icd10 (Provides the official code tables, guidelines, and updates).
-
American Hospital Association (AHA) Coding Clinic: The only authoritative source for official ICD-10-PCS coding advice. Subscription-based.
-
American Health Information Management Association (AHIMA): Offers educational resources, webinars, and certifications for coding professionals.
-
National Center for Health Statistics (NCHS): https://www.cdc.gov/nchs/icd/icd-10-pcs.htm (Provides background and maintenance process for ICD-10-PCS).
Date: December 10, 2025
Author: Medical Coding & Neurosurgical Documentation Specialists
Disclaimer: This article is for educational and informational purposes only. It is not a substitute for official coding guidance from the American Hospital Association’s Central Office (AHA COC) or the Centers for Medicare & Medicaid Services (CMS). Always consult the current year’s official ICD-10-PCS code books, guidelines, and updates for definitive coding decisions.





