Navigating the world of medical coding can feel like learning a new language. For healthcare professionals, medical coders, and even patients reviewing old records, understanding historical coding systems is crucial. The ICD-9 code for stroke represents a critical piece of medical history, used for decades to classify, track, and bill for cerebrovascular events. While the healthcare industry has transitioned to ICD-10, knowledge of ICD-9 remains vital for interpreting past medical records, handling legacy billing issues, and conducting longitudinal research.
This guide serves as your definitive reference. We’ll break down the specific codes, explain their structure, and provide the context you need to work with or understand these important diagnostic labels. Our goal is to transform complex coding information into clear, actionable knowledge.
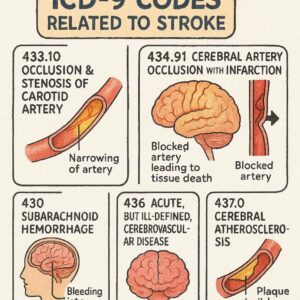
ICD-9 Codes for Stroke
Understanding ICD-9: The System Behind the Code
Before we dive into the specific codes for stroke, let’s establish what ICD-9 is and why it still matters today.
The International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) was the standard diagnostic coding system used in the United States from 1979 until October 1, 2015. Its primary purposes were to:
-
Translate medical diagnoses into standardized alphanumeric codes.
-
Support statistical tracking of disease prevalence and mortality.
-
Facilitate medical billing and reimbursement from insurance providers.
-
Enable epidemiological research and public health planning.
Think of ICD-9 as a vast, organized library where every known disease and health condition had a unique “call number.” A stroke, depending on its type and location, had several possible call numbers within the “chapter” for diseases of the circulatory system.
Key Note: As of October 1, 2015, the U.S. healthcare system officially transitioned to ICD-10-CM, which offers far greater specificity and detail. However, ICD-9 codes are still relevant for anyone dealing with medical records, insurance claims, or research data from before that date.
The Structure of an ICD-9 Code
An ICD-9 code is typically 3 to 5 digits long. The structure is hierarchical:
-
First three digits (Category): Represent the general disease category (e.g., 434 for occlusion of cerebral arteries).
-
Fourth digit (Subcategory): Adds detail about the etiology or anatomic site.
-
Fifth digit (Sub-classification): Provides even more specificity, such as location within the brain.
This structure allowed for basic specificity but was often criticized for being insufficiently detailed compared to modern medical needs, which was a key driver for the move to ICD-10.
Primary ICD-9 Codes for Stroke (Cerebrovascular Accident)
In ICD-9, strokes are classified under the broader category of “Diseases of the Circulatory System” (codes 390-459). There is no single, monolithic “stroke code.” Instead, the correct code depends entirely on the type of stroke that occurred. The two main categories are ischemic stroke and hemorrhagic stroke.
Ischemic Stroke (Blockage)
An ischemic stroke, accounting for about 87% of all cases, occurs when a blood clot blocks an artery supplying blood to the brain. The primary ICD-9 codes for ischemic stroke fall under the category “Occlusion and Stenosis of Pre-cerebral and Cerebral Arteries” (433-434).
Common ICD-9 Codes for Ischemic Stroke:
| ICD-9 Code | Code Description | Clinical Notes & Specificity |
|---|---|---|
| 433.xx | Occlusion and stenosis of pre-cerebral arteries | “Pre-cerebral” refers to arteries leading to the brain (e.g., carotid, vertebral). Requires a 5th digit. |
| 433.01 | Occlusion and stenosis of basilar artery with cerebral infarction | |
| 433.11 | Occlusion and stenosis of carotid artery with cerebral infarction | |
| 433.21 | Occlusion and stenosis of vertebral artery with cerebral infarction | |
| 433.31 | Occlusion and stenosis of multiple and bilateral pre-cerebral arteries with infarction | |
| 433.81 | Occlusion and stenosis of other specified pre-cerebral artery with infarction | |
| 433.91 | Occlusion and stenosis of unspecified pre-cerebral artery with infarction | |
| 434.xx | Occlusion of cerebral arteries | Refers to arteries within the brain itself. Requires a 5th digit. |
| 434.01 | Cerebral thrombosis with cerebral infarction | A clot forms locally in a cerebral artery. |
| 434.11 | Cerebral embolism with cerebral infarction | A clot travels from elsewhere (e.g., heart) to the brain. |
| 434.91 | Cerebral artery occlusion, unspecified with infarction | Used when the type of blockage (thrombosis vs. embolism) is not specified. |
Important Coding Distinction: The 5th digit of “1” in the codes above (e.g., 434.11) is critical. It indicates that the occlusion resulted in cerebral infarction (i.e., tissue death or stroke). A 5th digit of “0” would indicate occlusion without infarction, which is a different clinical scenario.
Hemorrhagic Stroke (Bleeding)
A hemorrhagic stroke occurs when a weakened blood vessel ruptures and bleeds into or around the brain. This type is less common but often more deadly. Its codes are found in a different section: “Intracranial Hemorrhage” (430-432).
Common ICD-9 Codes for Hemorrhagic Stroke:
| ICD-9 Code | Code Description | Clinical Notes & Specificity |
|---|---|---|
| 430 | Subarachnoid hemorrhage | Bleeding into the space between the brain and the tissue that covers it (the arachnoid membrane). Often from a ruptured aneurysm. |
| 431 | Intracerebral hemorrhage | Bleeding directly into the brain parenchyma itself. Often related to chronic hypertension or vascular malformations. |
| 432.xx | Other and unspecified intracranial hemorrhage | This category includes other types of bleeding. Requires a 4th digit. |
| 432.0 | Nontraumatic extradural hemorrhage | |
| 432.1 | Subdural hemorrhage | |
| 432.9 | Unspecified intracranial hemorrhage |
Essential Related and Sequelae Codes
A patient’s stroke diagnosis often involves more than just the acute event. ICD-9 provided codes for related conditions and long-term effects.
Transient Ischemic Attack (TIA) – The “Warning Stroke”
A TIA is a temporary blockage with stroke-like symptoms that resolve fully, typically within 24 hours. It’s a major warning sign for a future stroke.
-
ICD-9 Code: 435.9 – Unspecified transient cerebral ischemia. Often used for TIA.
Late Effects and Sequelae of Stroke
These codes are used for encounters where the acute stroke is no longer being treated, but the patient is dealing with its long-term consequences (sequelae). This is a crucial concept for accurate coding after the initial event.
-
ICD-9 Code: 438 – Late effects of cerebrovascular disease.
-
This code is never used alone. It must be paired with additional codes from the 438 series to specify the nature of the late effect (e.g., hemiplegia, speech deficits, cognitive issues).
-
Example:
438.21– Late effect of CVA affecting dominant side with hemiplegia.
-
Cerebrovascular Disease without Acute Event
For conditions that increase stroke risk but are not an acute stroke themselves.
-
ICD-9 Code: 437.9 – Unspecified cerebrovascular disease. Used for generalized cerebrovascular atherosclerosis or history of cerebrovascular disease not otherwise specified.
ICD-9 vs. ICD-10: A Critical Comparative Analysis
The transition from ICD-9 to ICD-10-CM represented a monumental shift in specificity. Understanding the differences is key to translating old records into the modern context.
Comparative Table: Stroke Coding in ICD-9 vs. ICD-10
| Feature | ICD-9-CM | ICD-10-CM |
|---|---|---|
| Code Format | 3-5 digits, mostly numeric | 3-7 characters, alphanumeric |
| Number of Codes for Stroke | Approximately 30 core codes | Over 450 codes (dramatically increased specificity) |
| Specificity | Limited. Often could not specify artery side (left/right) or laterality. | Highly Detailed. Always specifies laterality (left, right, bilateral). |
| Ischemic Stroke Example | 434.11 – Cerebral embolism with cerebral infarction |
I63.411 – Cerebral infarction due to embolism of right middle cerebral artery |
| Hemorrhagic Stroke Example | 431 – Intracerebral hemorrhage |
I61.3 – Nontraumatic intracerebral hemorrhage in brain stem |
| Sequela Coding | Single code 438 with subcodes |
Specific 7th character “S” for sequela added to the acute stroke code |
| Clinical Detail | Focused on type of event. | Incorporates etiology, location, and laterality directly into the code. |
The Fundamental Difference: ICD-10 tells a complete clinical story in the code itself. While ICD-9 code 434.11 tells you “embolic stroke,” ICD-10 code I63.411 tells you “embolic stroke, in the right middle cerebral artery.” This shift improves tracking, research, and care planning.
Practical Application: How to Use ICD-9 Stroke Codes
Even in the ICD-10 era, you may need to work with ICD-9 codes. Here’s a practical guide.
For Medical Coders & Billers (Handling Legacy Claims)
-
Identify the Stroke Type: Carefully review the physician’s documentation (neurology consult, discharge summary, imaging reports) to determine if the stroke was ischemic or hemorrhagic.
-
Determine Specificity: For ischemic strokes, was it a thrombosis or embolism? For hemorrhagic, was it intracerebral or subarachnoid?
-
Select the Correct Code: Use the code tables above as a guide. Crucially, verify with an official ICD-9 coding manual from the relevant year, as guidelines and updates occurred annually.
-
Code for Sequela When Applicable: If the encounter is for rehab or managing paralysis from a stroke that occurred months or years ago, code
438.xwith the appropriate subcode, not the acute stroke code.
For Patients & Families (Understanding Medical Records)
If you’re reading an old medical record and see an ICD-9 code:
-
Don’t Panic: The code is a standardized label, not a prognosis.
-
Use this Guide as a Decoder: Match the code on the record to the descriptions above to understand the general type of stroke documented.
-
Seek Clarification: Always discuss your medical history and records with your current healthcare provider. They can interpret the old codes in the context of your overall health.
For Researchers (Analyzing Historical Data)
-
Use Code Ranges: When querying databases for stroke patients pre-2015, you must include all relevant codes: the 433.x1 series, 434.x1 series, 430, 431, and 432.x.
-
Understand the Limitations: Recognize that ICD-9 data lacks laterality and precise anatomic detail. Your analysis should account for this lack of granularity compared to modern datasets.
-
Clean Your Data: Be aware of the distinction between acute event codes and sequela codes (
438) to avoid misclassifying follow-up visits as new strokes.
Common Pitfalls and Important Notes
Working with ICD-9 stroke codes requires attention to detail to avoid errors.
Critical Checklist for Accurate ICD-9 Stroke Coding:
-
Always use a 5th digit for 433 and 434 codes. “1” for infarction is standard for a diagnosed stroke.
-
Do not code a suspected or ruled-out diagnosis. Code only confirmed conditions.
-
Differentiate between acute stroke and sequela. Using an acute code for a rehab visit is a common billing error.
-
Consult the Tabular List. The official ICD-9 manual includes “Includes,” “Excludes,” and “Use additional code” notes that are essential for correct application.
-
Documentation is King. The code must always be supported by clear, specific language in the patient’s medical record.
Professional Insight: “The biggest mistake I see in historical chart reviews is the misinterpretation of code
438as an active stroke. In coding, context is everything. That code doesn’t mean the patient is having a stroke; it means they are dealing with the after-effects of one. This distinction changes the entire clinical and billing picture.” – Veteran Medical Coder
The Transition Forward: From ICD-9 to ICD-10-CM
On October 1, 2015, the U.S. mandated the use of ICD-10-CM for all diagnosis coding. This was not a simple update but a complete overhaul. For stroke, the change meant:
-
Increased Administrative Burden: Coders needed extensive training to learn the new, more complex system.
-
Improved Data Quality: The ability to track strokes by specific artery and side has enhanced public health research and resource allocation.
-
Clinical Documentation Improvement (CDI): Physicians had to document with much greater specificity (e.g., “acute ischemic stroke due to embolism of the left MCA”) to support the appropriate ICD-10 code.
While ICD-9 is now a historical system, its logic forms the foundation of our current understanding of disease classification. Mastering its principles, especially for major conditions like stroke, remains a valuable skill for navigating the full spectrum of medical information.
Conclusion
Understanding the ICD-9 codes for stroke is essential for accurately interpreting decades of medical records, billing data, and epidemiological research. While the system has been replaced by the more detailed ICD-10, its codes—from the 434 series for ischemic infarcts to the 430-432 range for hemorrhages—provide the foundational language for historical cerebrovascular disease classification. By grasping the distinctions between acute event coding and sequela designations like code 438, professionals can ensure accurate historical analysis and seamless transitions between old and new medical data frameworks, maintaining continuity in patient care and research integrity across coding generations.
Frequently Asked Questions (FAQ)
Q1: What is the most common ICD-9 code for a stroke?
A: There isn’t one single “most common” code, as it depends on stroke type. However, 434.11 (Cerebral embolism with cerebral infarction) and 434.91 (Unspecified cerebral artery occlusion with infarction) were frequently used for ischemic strokes. 431 (Intracerebral hemorrhage) was common for hemorrhagic strokes.
Q2: I see code 438.xx on my old record. Does that mean I had a stroke?
A: Yes, but it provides important nuance. Code 438 indicates “Late Effects of Cerebrovascular Disease.” This means you had a stroke (CVA) in the past, and this particular medical encounter was for treating or managing the lasting consequences of that stroke, such as paralysis (hemiplegia) or speech difficulties, not for a new acute stroke.
Q3: Why did the code system change from ICD-9 to ICD-10?
A: ICD-9 was outdated, with limited space for new codes and insufficient clinical detail. ICD-10 was adopted to allow for greater specificity (e.g., which side of the body was affected), better tracking of public health trends, more accurate billing, and alignment with modern medical practices and technology.
Q4: Can a doctor still use an ICD-9 code today?
A: No. For all diagnosis coding on medical claims submitted in the United States for services provided on or after October 1, 2015, the use of ICD-10-CM codes is mandatory. Using an ICD-9 code would result in claim rejection.
Q5: How do I find the modern ICD-10 equivalent of an old ICD-9 stroke code?
A: There are official “crosswalks” or general equivalence mappings (GEMs) provided by the Centers for Medicare & Medicaid Services (CMS). However, because one ICD-9 code often maps to many ICD-10 codes, the correct translation depends on the specific clinical details in the medical record. It’s best performed by a qualified medical coder using the patient’s documentation.
Additional Resources
For those seeking to deepen their understanding or verify official information, we recommend consulting these authoritative sources:
-
Centers for Disease Control and Prevention (CDC) – ICD-9 & ICD-10 Pages: Provides background, official guidelines, and tools related to disease classification.
-
National Center for Health Statistics (NCHS): The U.S. government agency responsible for maintaining the ICD-10-CM system.
-
American Health Information Management Association (AHIMA): The premier professional organization for medical coders, offering educational resources and updates on coding standards.
-
American Heart Association/American Stroke Association: For comprehensive clinical information on stroke types, symptoms, and treatment, which informs proper coding.
-
Official ICD-9-CM and ICD-10-CM Code Books: While outdated for active use, historical ICD-9 manuals can be found through medical publishers and libraries for reference purposes.
Disclaimer: This article is intended for informational and educational purposes only. It is not a substitute for professional medical coding advice, clinical guidance, or official coding resources. Medical coding is a complex and regulated field. For accurate coding of any medical condition, healthcare providers and coders must consult the most current, official ICD-10-CM code sets and guidelines published by the Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS), as well as complete and specific clinical documentation. The author and publisher disclaim any liability for errors or omissions or for any outcomes related to the use of this information.
Date: January 03, 2025
Author: The Web Health Writer Team





