In the intricate plumbing system of the human body—the urinary tract—the ureters serve as vital, slender pipes, tirelessly transporting urine from the kidneys to the bladder. These muscular tubes, though robust, are vulnerable to obstruction. A kidney stone, a sinister stricture, a compressing tumor, or surgical trauma can dam this essential flow, leading to a hydraulic crisis known as hydronephrosis. The backup of urine creates dangerous pressure, threatening the functional integrity of the kidney itself, causing severe pain, infection, and potential loss of renal function.
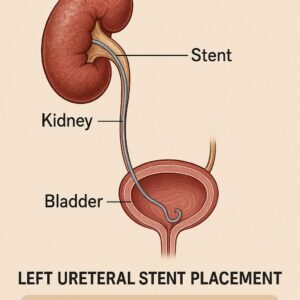
Enter the ureteral stent: a flexible, hollow, and seemingly simple tube that becomes a silent sentinel of renal salvation. Typically made of silicone or polyurethane, this device is engineered to act as an internal bypass. When placed, it spans the distance from the renal pelvis in the kidney down to the bladder, creating a passive conduit for urine to flow around an obstruction or to protect a surgical anastomosis. The stent’s coiled ends—a “pig-tail” in the kidney and another in the bladder—anchor it in position, preventing migration. For patients, it is often a paradoxical presence: a source of relief from the catastrophic threat of renal failure, yet often accompanied by bothersome symptoms like urinary frequency, urgency, and flank pain during voiding, a phenomenon known as “stent syndrome.”
The decision to place a stent, particularly in the left ureter, is never trivial. It is a calculated intervention to preserve renal function, manage pain, facilitate healing, or prepare for further treatment. The procedure itself is a testament to modern minimally invasive urology, but its administrative and financial translation—the act of capturing its complexity in a series of alphanumeric characters—is where the equally critical world of ICD-10-PCS coding begins.
Left Ureteral Stent Placement and Its ICD-10-PCS Code
2. Navigating the Lexicon of Care: The Critical Role of ICD-10-PCS Coding
If medicine is the language of healing, then medical coding is its essential grammar and syntax for the healthcare ecosystem. The International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) is not merely an administrative afterthought; it is a multifunctional linchpin in modern healthcare. Unlike its diagnosis-focused counterpart (ICD-10-CM), ICD-10-PCS is used exclusively in inpatient hospital settings in the United States to describe the procedures performed. Its primary roles are multifaceted:
-
Financial Reimbursement: It forms the basis for DRG (Diagnosis-Related Group) assignment, which determines the fixed payment a hospital receives from Medicare and other insurers for an inpatient stay. An inaccurate code can lead to underpayment or costly denials.
-
Epidemiological Tracking & Research: Aggregated procedure data allows public health officials and researchers to track the prevalence of surgical interventions, study outcomes, and allocate resources.
-
Quality Metrics and Benchmarking: Hospitals use this data to compare their surgical volumes and outcomes against national benchmarks, driving quality improvement initiatives.
-
Operational Planning: Understanding procedure volumes helps hospitals manage inventory (like stents themselves), schedule operating room time, and staff appropriately.
ICD-10-PCS is built on a logical, multi-axial structure. Each code is composed of seven alphanumeric characters, with each character representing a specific aspect of the procedure. This structure demands precision. There is no room for interpretation or approximation. The code for placing a stent in the left ureter is fundamentally different from placing one in the right ureter, or from removing it, or from placing a different device altogether. This granularity, while complex, is what makes the system powerful and unambiguous. For the coder, the surgeon’s operative note is the sacred text from which these seven characters must be meticulously derived.
3. Deconstructing the Code: A Deep Dive into 0TH94KZ and Its Neighbors
Let us dissect the specific code for Left Ureteral Stent Placement: 0TH94KZ.
This string of characters is not random; it is a precise, structured narrative of the procedure.
-
Character 1 (Section): 0 – This identifies the section of the procedure. “0” corresponds to the Medical and Surgical section, which encompasses the vast majority of invasive procedures.
-
Character 2 (Body System): T – This denotes the Urinary System. This character immediately narrows the field from all possible surgical procedures to those involving the kidneys, ureters, bladder, and urethra.
-
Character 3 (Root Operation): H – This is the core of the code. “H” stands for Insertion. In PCS terminology, “Insertion” is defined as “putting in a non-biologic device that remains in the body after the procedure” (e.g., a pacemaker, a catheter, or, in this case, a stent). It is critically distinct from “Replacement” (changing a device) or “Removal” (taking a device out).
-
Character 4 (Body Part): 9 – This character specifies the exact site. “9” corresponds to the Ureter, Left. This is where laterality is decisively captured. The code for the right ureter would use a different character (8 for Ureter, Right).
-
Character 5 (Approach): 4 – The approach describes the technique used to reach the body part. “4” signifies Via Natural or Artificial Opening. For most ureteral stent placements, this refers to a cystoscopic approach—the surgeon passes instruments through the urethra (a natural opening) and into the bladder, then accesses the ureteral orifice.
-
Character 6 (Device): K – This character identifies the device that is being inserted and will remain. “K” is defined as an Intraluminal Device, Urinary. A ureteral stent is the quintessential example of this device category.
-
Character 7 (Qualifier): Z – This character provides additional detail when needed. “Z” is a No Qualifier placeholder, indicating that no further specification is applicable for this particular combination.
Therefore, 0TH94KZ literally translates to: “Medical and Surgical procedure on the Urinary System, involving the Insertion of an Intraluminal Device into the Left Ureter, performed Via a Natural or Artificial Opening Endoscopic approach.”
Contrasting Key Codes: A Comparative Table
| ICD-10-PCS Code | Code Meaning | Clinical Scenario | Key Differentiator |
|---|---|---|---|
| 0TH94KZ | Insertion of intraluminal device into left ureter, via natural opening | Standard cystoscopic placement of a left ureteral stent. | The primary code for standard left stent placement. |
| 0TH97KZ | Insertion of intraluminal device into left ureter, via percutaneous | Antegrade stent placement; access is through the kidney skin. | Approach (Char 5): Percutaneous (7) vs. Via Opening (4). |
| 0TH98KZ | Insertion of intraluminal device into right ureter, via natural opening | Standard cystoscopic placement of a right ureteral stent. | Body Part (Char 4): Right Ureter (8) vs. Left Ureter (9). |
| 0TP94KZ | Removal of intraluminal device from left ureter, via natural opening | Cystoscopic removal of a left ureteral stent. | Root Op (Char 3): Removal (P) vs. Insertion (H). |
| 0TH93KZ | Insertion of intraluminal device into left ureter, via open approach | Stent placed during an open abdominal or pelvic surgery. | Approach (Char 5): Open (3) vs. Via Opening (4). |
| 0TH94MZ | Insertion of infusion device into left ureter, via natural opening | Placement of a left ureteral catheter for continuous irrigation. | Device (Char 6): Infusion Device (M) vs. Intraluminal Device (K). |
*Table 1: ICD-10-PCS Code Differentiation for Ureteral Procedures. This table highlights how a single character change reflects a fundamentally different procedure.*
4. The Clinical Journey: From Indication to Insertion
The pathway to code 0TH94KZ begins long before the patient enters the operating room. It starts with a clinical story.
Common Indications for Left Ureteral Stent Placement:
-
Obstructive Nephrolithiasis: A stone lodged in the left ureter, causing hydronephrosis.
-
Malignant Obstruction: Extrinsic compression from cancers like cervical, colorectal, or prostate cancer affecting the left ureter.
-
Benign Strictures: Narrowing from prior surgery, radiation therapy, or inflammatory conditions.
-
Prophylactic/Perioperative Stenting: To protect the ureter during complex pelvic or abdominal surgeries (e.g., hysterectomy, colectomy) or to facilitate healing after ureteral reconstruction.
-
Urinary Leak: To divert urine and promote healing of a ureteral injury or anastomosis.
-
Instrumentation Access: To dilate a ureteral stricture over time (a “stent-string”).
The patient’s journey typically involves a crescendo of symptoms—colicky flank pain, nausea, hematuria—leading to imaging. A CT scan is the gold standard, revealing the dilated left renal pelvis and ureter proximal to the point of obstruction. Once the decision to stent is made, the procedure is scheduled, and the meticulous process of documentation and coding preparation begins.
5. The Anatomy of a Procedure: A Step-by-Step Technical Exploration
Understanding the technical steps is crucial for both clinicians and coders to ensure accuracy. A standard cystoscopic left ureteral stent placement unfolds as follows:
-
Anesthesia: The procedure is performed under general, spinal, or even local anesthesia with sedation.
-
Positioning & Preparation: The patient is placed in the dorsal lithotomy position. The genitalia are cleansed and draped.
-
Cystoscopy: A rigid or flexible cystoscope is introduced via the urethra into the bladder. The bladder mucosa and, critically, the left ureteral orifice are visualized.
-
Guidewire Cannulation: Under direct vision, a floppy-tipped guidewire is advanced through the cystoscope’s working channel and carefully threaded into the left ureteral orifice, navigating past the obstruction under fluoroscopic (live X-ray) guidance until its tip coils in the renal pelvis.
-
Stent Selection & Placement: A stent of appropriate length and diameter is chosen. It is threaded over the guidewire. Using a pusher catheter, the stent is advanced until the proximal (renal) coil is confirmed fluoroscopically to be in the renal pelvis. The guidewire is then slowly withdrawn, allowing the distal (bladder) coil to form inside the bladder.
-
Confirmation: Final fluoroscopic images confirm correct positioning of both coils, with the stent’s mid-portion traversing the entire length of the left ureter.
-
Cystoscope Removal: The cystoscope is removed. A Foley catheter may or may not be left temporarily.
For the coder, the operative report must clearly document: the procedure performed (insertion), the specific device (ureteral stent/intraluminal device), the exact body part (left ureter), and the surgical approach (cystoscopic/via natural opening). Any deviation, such as the use of a ureteral balloon to dilate a stricture before stent placement, may require an additional procedure code.
6. Beyond the Primary Code: The Essential Ecosystem of Supporting Codes
No procedure exists in a coding vacuum. 0TH94KZ is the centerpiece, but a complete and accurate bill requires a constellation of supporting codes that paint the full clinical picture.
-
Diagnosis Codes (ICD-10-CM): These justify the medical necessity of the stent placement. Examples include:
-
N13.1 – Hydronephrosis with ureteral stricture, not elsewhere classified
-
N20.1 – Calculus of ureter, left
-
N13.6 – Pyonephrosis (if infected)
-
A code for the underlying malignancy (e.g., C67.5 – Malignant neoplasm of bladder neck) if causing obstruction.
-
-
Additional Procedure Codes: The same operative note may describe other billable interventions:
-
Cystoscopy (0TJB8ZZ): Always performed as part of the access, but may be separately coded depending on payer guidelines and the primary reason for the procedure.
-
Ureteral Dilation (0T7D8ZZ): If a balloon dilator was used to treat a stricture.
-
Biopsy (0T9D8ZX): If a tissue sample was taken from the ureter or bladder.
-
-
Anesthesia & Supply Codes: CPT/HCPCS codes from the hospital’s chargemaster are used for the specific stent model used, the guidewires, and other disposable equipment.
This ecosystem underscores the need for seamless communication between the urology team, who must provide detailed documentation, and the health information management (HIM) coding professionals, who must interpret that documentation with expert knowledge of ICD-10-PCS guidelines.
7. The High-Stakes Impact: How Precision Coding Drives Healthcare Outcomes
The consequences of inaccurate coding extend far beyond a clerical error. They have tangible, high-stakes impacts:
-
Financial Integrity: Undercoding (using a less specific code) can result in significant revenue loss for the hospital. Overcoding (misrepresenting the complexity) can trigger audits, hefty penalties, and allegations of fraud.
-
Distorted Clinical Data: If stent placements are miscoded, the data used for public health research, device safety monitoring, and epidemiological studies becomes unreliable. This can obscure trends in kidney stone disease or complications related to stents.
-
Impaired Quality Assessment: Hospitals rely on accurate procedure data to calculate infection rates, complication rates, and readmission rates related to specific interventions like stent placement. Inaccurate codes corrupt these quality metrics.
-
Patient-Care Repercussions: While indirect, incorrect coding can affect future care. An incomplete procedural history in a patient’s electronic health record, due to coding errors, could lead to repeated procedures or inappropriate treatment plans.
Therefore, the act of correctly assigning 0TH94KZ is a professional responsibility that upholds the financial, scientific, and ethical pillars of healthcare delivery.
8. Case Studies in Clarity: Applying Knowledge to Real-World Scenarios
Case Study 1: The Standard Stone
*A 45-year-old male presents with severe left flank pain. CT shows a 7mm obstructing stone in the left mid-ureter with hydronephrosis. He undergoes cystoscopy with laser lithotripsy and placement of a left ureteral stent.*
-
Primary Procedure Code: 0TH94KZ (Insertion of stent into left ureter).
-
Secondary Procedure Code: 0TH68ZZ (Destruction of stone in left ureter, via natural opening).
-
Primary Diagnosis: N20.1 (Calculus of left ureter).
-
Secondary Diagnosis: N13.1 (Hydronephrosis).
Case Study 2: The Malignant Obstruction
*A 68-year-old female with a history of cervical carcinoma presents with anuria and renal failure. Imaging reveals bilateral hydronephrosis due to pelvic tumor recurrence. She undergoes bilateral ureteral stent placements.*
-
Left Ureter Procedure Code: 0TH94KZ.
-
Right Ureter Procedure Code: 0TH98KZ.
-
Primary Diagnosis: C79.82 (Secondary malignant neoplasm of genital organs).
-
Secondary Diagnoses: N13.1 (Hydronephrosis), N17.9 (Acute kidney failure).
Case Study 3: The Complex Stricture
A patient with a history of left ureteral injury from prior surgery presents with a tight stricture. The urologist performs a cystoscopy, dilates the left ureteral stricture with a balloon, and then places a stent.
-
Primary Procedure Code: 0TH94KZ (Stent insertion).
-
Secondary Procedure Code: 0T7D8ZZ (Dilation of left ureter).
-
Diagnosis: N13.1 (Hydronephrosis with ureteral stricture).
9. The Future Horizon: Trends in Urology and Procedural Coding
The field is evolving, and coding must adapt. Trends include:
-
Biodegradable Stents: Devices that dissolve over time, eliminating the need for a second procedure for removal. PCS will need new device characters or qualifiers to capture this technology.
-
Drug-Eluting Stents: Stents coated with medications to reduce infection or encrustation. This may require a new device value or significant documentation to capture the enhanced function.
-
Enhanced Robotics & Navigation: Increasingly precise placement techniques may eventually be reflected in more granular approach or device qualifiers.
-
Artificial Intelligence in Coding: AI-assisted coding tools are emerging, but they will never replace the need for skilled human coders who understand clinical context. The coder’s role will evolve towards auditing and complex case analysis.
10. Conclusion: The Confluence of Clinical Skill and Coding Precision
The journey of the left ureteral stent—from a life-saving clinical intervention to its precise representation as ICD-10-PCS code 0TH94KZ—epitomizes the dual engines of modern healthcare. It requires the technical mastery of the urologist navigating anatomy and pathology, and the analytical precision of the coder navigating a complex lexicon. Together, they ensure that patient care is not only delivered expertly at the bedside but is also communicated accurately to the wider systems that fund, study, and improve medicine for all. In this confluence lies the true art and science of healthcare delivery.
11. Frequently Asked Questions (FAQs)
Q1: What is the difference between CPT codes and ICD-10-PCS codes for this procedure?
A: CPT (Current Procedural Terminology) codes are used primarily by physicians to bill for their professional services in both outpatient and inpatient settings (e.g., 52332 – Cystourethroscopy with insertion of indwelling ureteral stent). ICD-10-PCS is used only by hospitals to bill for the facility resources used during an inpatient admission. They are two parallel but interconnected systems.
Q2: Why is the approach character so important? What if the approach isn’t clearly documented?
A: The approach (Character 5) directly impacts the DRG and reimbursement, as an “Open” approach is more resource-intensive than an endoscopic one. If the approach isn’t documented, the coder must query the physician. It is unacceptable to guess; the default is not to code the procedure.
Q3: How do you code a stent exchange?
A: A stent exchange is technically a Removal of the old device (0TP94KZ) followed by an Insertion of a new device (0TH94KZ). Both codes should be assigned if performed during the same operative session.
Q4: Is fluoroscopy guidance included in the code 0TH94KZ?
A: No. Fluoroscopic guidance is considered an integral part of the procedure for stent placement and is not separately coded in ICD-10-PCS. Separate radiation physics codes might be billed by the hospital’s radiology department.
Q5: What is the most common coding error related to ureteral stent placement?
A: Misidentifying laterality (Left vs. Right) or the root operation (Insertion vs. Removal). Relying on a discharge summary instead of the detailed operative report is a common source of these errors.
Date: December 11, 2025
Author: This article was composed by a team with expertise in clinical urology and health information management. It is intended for educational and informational purposes only.
Disclaimer: The information contained in this article is for educational purposes and does not constitute medical advice or official coding guidance. While every effort has been made to ensure accuracy, codes and guidelines are subject to change. Always consult the most current, official ICD-10-PCS code set, guidelines, and the physician’s documentation before assigning codes. The author and publisher assume no responsibility for errors or omissions or for any outcomes related to the application of this information.





