A gastrointestinal bleed (GIB) is not merely a diagnostic entry in a patient’s chart; it is a dramatic, often life-threatening event that sets in motion a rapid cascade of clinical interventions. In the bustling emergency department, the endoscopy suite, or the inpatient ward, the focus is rightly on stabilization, diagnosis, and treatment. Yet, once the immediate crisis has passed, a parallel process begins—one that translates the clinical narrative into the precise, structured language of medical codes. This process, centered on the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), is far from a simple administrative task. For a condition as complex and varied as a GI bleed, accurate coding is a critical linchpin connecting patient care to outcomes analysis, reimbursement integrity, and the very data that drives public health understanding.
The ICD-10 code for a GI bleed is more than a number; it is a story condensed into a series of alphanumeric characters. Does the code K92.2 (Gastrointestinal hemorrhage, unspecified) tell the same story as K25.4 (Gastric ulcer with hemorrhage) or I85.01 (Esophageal varices with bleeding)? To a clinician, a researcher, or a payer, the difference is profound. The unspecified code paints a picture of uncertainty, a mystery yet to be solved. The specific codes, however, provide a clear diagnosis, implying a known etiology, a specific treatment pathway, and a distinct prognosis. This guide is designed to be an exhaustive resource for medical coders, students, and healthcare professionals who seek to master the nuanced art of coding gastrointestinal hemorrhages. We will move beyond the basic code lookup and delve deep into the clinical context, the structure of the ICD-10-CM system, the intricacies of official guidelines, and the practical application of this knowledge through real-world case studies. Our goal is to equip you with the expertise to consistently choose the most specific and accurate code, ensuring that the story told by the data is as clear and truthful as the story written in the medical record.
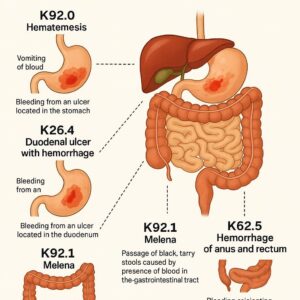
ICD-10 Codes for Gastrointestinal Bleed
2. Understanding the Landscape of GI Bleeds: A Clinical Primer for Coders
To code a GI bleed accurately, one must first understand what it is. A GI bleed refers to any form of bleeding that occurs within the gastrointestinal tract, which stretches from the mouth to the anus. The clinical presentation, diagnostic approach, and ultimate code assignment are heavily influenced by the bleed’s location, acuity, and volume.
Anatomy of the GI Tract: From Esophagus to Rectum
The GI tract is conventionally divided into two main sections:
-
Upper GI Tract: This includes the esophagus, stomach, and the first part of the small intestine (duodenum). A bleed originating from a source proximal to the ligament of Treitz is classified as an upper GI bleed.
-
Lower GI Tract: This encompasses the remainder of the small intestine (jejunum and ileum), the large intestine (colon), rectum, and anus. Bleeding from a source distal to the ligament of Treitz is a lower GI bleed.
This anatomical distinction is crucial because the symptoms and diagnostic tests differ significantly.
The Clinical Spectrum: Acute vs. Chronic, Overt vs. Occult
GI bleeds are also categorized by their timing and visibility:
-
Acute GI Bleed: A sudden, often severe hemorrhage that constitutes a medical emergency. Symptoms appear rapidly and can include hematemesis (vomiting blood), melena (black, tarry stools), or hematochezia (bright red blood per rectum).
-
Chronic GI Bleed: A slow, gradual loss of blood that may go unnoticed for some time. It often presents as iron deficiency anemia (fatigue, weakness) rather than visible bleeding.
-
Overt GI Bleed: Bleeding that is visible to the patient or clinician, such as vomiting blood or passing bloody stools.
-
Occult GI Bleed: Bleeding that is not visible. It is typically detected through laboratory tests like a fecal occult blood test (FOBT) or a fecal immunochemical test (FIT).
Common Causes and Risk Factors
A wide array of conditions can cause GI bleeding. Common causes for upper GI bleeds include peptic ulcers (gastric or duodenal), esophageal varices (dilated veins in patients with liver disease), gastritis, and Mallory-Weiss tears (tears in the esophagus from violent vomiting). Lower GI bleeds are frequently caused by diverticulosis, angiodysplasia (abnormal blood vessels), hemorrhoids, anal fissures, colitis (inflammatory or ischemic), and colorectal cancer. Understanding these causes is the first step toward selecting the correct ICD-10 code, as the coding system is designed to capture this specific etiology whenever it is known.
3. Navigating the ICD-10-CM Chapter on Diseases of the Digestive System (K00-K95)
The logical starting point for coding a GI bleed is Chapter 11 of the ICD-10-CM manual: Diseases of the Digestive System (K00-K95). Within this chapter, you will find the most commonly used codes for GI hemorrhage when a more specific site has not been identified.
The Structure of Chapter 11
Chapter 11 is organized anatomically, covering diseases of the oral cavity, esophagus, stomach, intestines, appendix, rectum, liver, gallbladder, and pancreas. The codes for generalized or unspecified GI bleeding are found toward the end of the chapter, under the category K92 – Other diseases of digestive system.
The Importance of Code Specificity
A fundamental principle of ICD-10-CM is to code to the highest level of specificity. The system is designed to capture detailed information about a patient’s condition. Using an unspecified code should be a last resort, used only when the medical record documentation does not support a more precise code. This is especially true for GI bleeds, where the difference between an unspecified code and a site-specific code can have significant implications for reimbursement (via DRG assignment) and quality reporting.
4. Decoding the Primary Categories: K92.2 vs. K92.1
When a provider’s documentation is limited to terms like “GI bleed,” “GIB,” or “hematemesis” without a confirmed source, you will turn to the K92 category.
K92.2: Gastrointestinal Hemorrhage, Unspecified
This is the catch-all code for a GI bleed of unknown origin. It is used when the documentation does not specify whether the bleed is upper or lower and does not point to a specific cause like an ulcer or varices. Terms that typically lead to K92.2 include:
-
Gastrointestinal hemorrhage NOS (Not Otherwise Specified)
-
Intestinal hemorrhage NOS
-
Hematemesis (vomiting blood) without a specified cause (e.g., not linked to varices)
-
Hematochezia (bright red blood per rectum) without a specified cause (e.g., not linked to diverticulosis or hemorrhoids)
Crucial Point: If the provider documents “hematemesis” and the workup confirms esophageal varices, you must code the more specific I85.01 (Esophageal varices with bleeding), not K92.2. K92.2 is a code of necessity, not choice.
K92.1: Melena
Melena is a specific clinical sign, not a diagnosis. It refers to black, tarry, foul-smelling stools resulting from the digestion of blood, which typically indicates an upper GI bleed (though a slow bleed in the small intestine can also cause it). Code K92.1 is assigned when the provider documents melena as a confirmed symptom, but the underlying source has not been definitively identified. If the source is known (e.g., “melena due to a bleeding duodenal ulcer”), you would code the underlying condition with hemorrhage (K26.4 for a duodenal ulcer with hemorrhage) as the principal diagnosis. K92.1 would not be used in this case.
A Comparative Table: K92.2 vs. K92.1
| Feature | K92.2 – Gastrointestinal Hemorrhage, Unspecified | K92.1 – Melena |
|---|---|---|
| Definition | A general term for bleeding anywhere in the GI tract without a specified site or cause. | A specific symptom describing digested blood in the stool, indicating a likely upper GI source. |
| Common Documentation | “GI bleed,” “GIB,” “hematemesis,” “intestinal bleeding,” “hematochezia” (without known cause). | “Melena,” “black tarry stools.” |
| Clinical Implication | Represents a diagnostic uncertainty. The source of the bleed is unknown. | Represents a specific clinical finding. While the exact source may be unknown, it localizes the bleed to the upper GI tract in most cases. |
| When to Use | When the medical record lacks specificity regarding the site or etiology of the bleed. | When melena is documented as a presenting sign, and no more specific bleeding source is identified. |
| Example | A patient presents to the ER vomiting blood. The initial diagnosis is “acute GI hemorrhage” before endoscopy. | A patient complains of black stools for one week. The provider documents “melena” pending further workup. |
5. The Pursuit of Specificity: Coding by Site of Origin
The true power of ICD-10-CM is realized when the site and cause of the bleed are documented. In these cases, you must abandon the unspecified K92 codes and use the specific code for the underlying condition.
Esophageal Hemorrhage (I85.-)
It is critical to note that codes for esophageal varices are not located in Chapter 11 (K00-K95). They are found in Chapter 9: Diseases of the Circulatory System (I00-I99), under the category I85 – Esophageal varices.
-
I85.01 – Esophageal varices with bleeding: This code is used when varices are confirmed as the source of active bleeding.
-
I85.11 – Secondary esophageal varices with bleeding: Used for varices due to a specified underlying condition like portal hypertension.
-
I85.00 / I85.10 – Esophageal varices without bleeding: Used for a history of varices or if varices are present but not bleeding during the encounter.
-
K22.8 – Other specified diseases of esophagus: This category includes non-variceal bleeds, such as those from esophagitis. For example, K20.0 is for reflux esophagitis with bleeding.
Gastric and Duodenal Ulcers (K25-K28)
Peptic ulcer disease is a leading cause of upper GI bleeds. The codes require fourth and fifth characters to specify the stage of the ulcer (acute, chronic, etc.) and whether complications like hemorrhage or perforation are present.
-
K25.- Gastric ulcer: The fifth character indicates the presentation.
-
K25.0 – Acute with hemorrhage
-
K25.4 – Chronic or unspecified with hemorrhage
-
-
K26.- Duodenal ulcer:
-
K26.0 – Acute with hemorrhage
-
K26.4 – Chronic or unspecified with hemorrhage
-
-
K27.- Peptic ulcer, site unspecified: Used only if the provider cannot determine if it’s gastric or duodenal.
-
K28.- Gastrojejunal ulcer: For ulcers at the anastomosis site after certain surgeries.
Coding Tip: If the documentation states “bleeding ulcer,” you must query whether it is gastric or duodenal to avoid using the less specific K27.- codes.
Angiodysplasia of GI Tract (K55.21)
Angiodysplasia is a common cause of lower GI bleeding, especially in older adults. It involves fragile, abnormal blood vessels in the colon. The specific code is K55.21 – Angiodysplasia of colon with hemorrhage. If angiodysplasia is present without bleeding, use K55.20.
Diverticular Disease (K57. )
Diverticulosis (the presence of pouches in the colon wall) can lead to bleeding. The codes for diverticular disease are complex and are based on location (small intestine or large intestine) and the presence of complications (bleeding, perforation, abscess).
-
K57.41 – Diverticulosis of large intestine with bleeding
-
K57.51 – Diverticulosis of both small and large intestine with bleeding
Hemorrhoids (I84. )
Like esophageal varices, hemorrhoid codes are located in Chapter 9 (Diseases of the Circulatory System). They are classified by type and severity.
-
I84.1 – Internal thrombosed hemorrhoids
-
I84.3 – External thrombosed hemorrhoids
-
I84.5 – Residual hemorrhoidal skin tags
-
Important: You must add a 7th character to these codes to indicate the encounter (A, D, S). For example, I84.1-XXXA for an initial encounter.
6. The Critical Role of Documentation: Bridging the Gap between Clinician and Coder
The accuracy of medical coding is entirely dependent on the quality of clinical documentation. Coders are instructed to code based on what is documented, not on what they might suspect or infer.
Key Phrases that Drive Code Selection
-
“Suspected” or “Rule Out”: You cannot code a diagnosis that is documented as “suspected” or “rule out.” You code the signs and symptoms (e.g., hematemesis, melena, anemia) until a definitive diagnosis is established.
-
“Due to”: This is the gold standard for coders. Phrases like “melena due to a bleeding duodenal ulcer” directly link the symptom to the cause, mandating the use of code K26.4.
-
Post-procedural Bleeding: If a bleed occurs after a procedure like a colonoscopy with polypectomy, you must use a code from the T81 series, specifically T81.710A – Complication of following ectopic and molar pregnancy is incorrect; the correct code would be T81.710A – Hemorrhage complicating a procedure for the initial encounter, along with the code for the specific site if known.
Querying for Clarity: When and How to Ask for More Information
When documentation is ambiguous, contradictory, or incomplete, a coder should initiate a physician query. A query is a formal, non-leading communication seeking clarification. For example:
-
Scenario: The discharge summary states “GI bleed,” but the endoscopy report describes “a bleeding ulcer in the duodenal bulb.”
-
Query: “Dear Dr. Smith, The endoscopy report identifies a bleeding duodenal ulcer. May we clarify the principal diagnosis for this admission as ‘Duodenal ulcer with hemorrhage’ for accurate coding?”
This process is essential for ensuring coding accuracy and compliance.
7. Complex Coding Scenarios and Comorbidities
Patients with GI bleeds often have multiple conditions that need to be coded.
Coding Anemia in the Context of GI Bleed (D50.0, D62)
Acute blood loss from a GI bleed causes anemia. The Official Coding Guidelines state that when a patient is admitted for acute blood loss anemia due to a GI bleed, the cause of the anemia (the GI bleed) is sequenced as the principal diagnosis. The acute blood loss anemia is coded as a secondary diagnosis.
-
D62 – Acute posthemorrhagic anemia is the appropriate code for anemia due to an acute GI bleed.
-
D50.0 – Iron deficiency anemia secondary to blood loss (chronic) is used if the bleed has been slow and chronic.
The Impact of Anticoagulants and Antiplatelets
If a GI bleed is caused or exacerbated by a medication like warfarin (Coumadin) or aspirin, additional codes are required.
-
First, code the GI bleed (e.g., K92.2, K25.0).
-
Then, code the adverse effect of the drug using a code from the T45.5- series (Anticoagulant antagonists, vitamin K, etc.) or T39.01- series (Salicylates poisoning).
-
Finally, you may need to code the reason the patient is on the medication (e.g., I48.91 for atrial fibrillation).
Sepsis and Shock Resulting from GI Hemorrhage
A massive GI bleed can lead to hypovolemic shock. In this case, the GI bleed is the underlying cause. The principal diagnosis would be the specific GI bleed (e.g., K25.0), followed by a code for hypovolemic shock (R57.1).
8. The 7th Character Extension: The Episode of Care (A, D, S)
For certain codes, including many related to injuries and complications of care, a 7th character is required to indicate the episode of care.
-
A – Initial Encounter: Used for active treatment for the condition (e.g., the patient is admitted for the bleed).
-
D – Subsequent Encounter: Used for routine care after the active phase of treatment is over (e.g., a follow-up office visit to check healing).
-
S – Sequela: Used for complications or conditions that arise as a direct result of the initial condition (e.g., stricture formation after healing of an ulcer-related bleed).
Most of the K92 codes do not require a 7th character. However, codes for hemorrhoids (I84.-) and post-procedural bleeding (T81.71-) do require them.
9. Case Studies: Applying Knowledge to Real-World Scenarios
Case Study 1: The Elderly Patient with Melena and Hemoglobin Drop
-
Presentation: An 80-year-old woman presents to the ER with weakness and black, tarry stools for two days. Her hemoglobin is 7.0 g/dL (down from a baseline of 12.0). The ER physician documents “melena and acute anemia likely due to GI bleed.”
-
Initial Codes: K92.1 (Melena), D62 (Acute posthemorrhagic anemia).
-
Hospital Course: An esophagogastroduodenoscopy (EGD) reveals a 1.5 cm gastric ulcer with a visible vessel that is cauterized. The final diagnosis is “Bleeding gastric ulcer.”
-
Final Codes: K25.4 (Chronic or unspecified gastric ulcer with hemorrhage) as the principal diagnosis. D62 is retained as a secondary diagnosis. K92.1 is not used because a more specific cause has been identified.
Case Study 2: The Patient with Cirrhosis and Hematemesis
-
Presentation: A 55-year-old man with a history of alcoholic cirrhosis is brought in after vomiting a large amount of blood. The ER note states “Hematemesis, likely from esophageal varices.”
-
Initial Codes: While varices are suspected, you cannot code them until confirmed. You would use R11.10 (Vomiting of blood, unspecified) and K74.60 (Unspecified cirrhosis of liver).
-
Hospital Course: An emergency EGD confirms large, bleeding esophageal varices, which are banded.
-
Final Codes: I85.11 (Secondary esophageal varices with bleeding) as the principal diagnosis. K70.31 (Alcoholic cirrhosis of liver with ascites) would be used if documented, providing more specificity than K74.60.
Case Study 3: Post-Polypectomy Bleed Following a Colonoscopy
-
Presentation: A patient is readmitted 3 days after an outpatient colonoscopy during which a large polyp was removed. They report passing bright red blood per rectum.
-
Documentation: The admitting diagnosis is “post-polypectomy hemorrhage.”
-
Coding: This is a complication of a procedure. The correct code is T81.710A – Hemorrhage complicating a procedure, initial encounter. You would also code the specific site if known from a subsequent procedure (e.g., K62.5 for hemorrhage of anus and rectum). The reason for the original colonoscopy (e.g., screening, Z12.11) may also be coded.
10. Common Pitfalls and Audit Risks in GI Bleed Coding
-
Defaulting to K92.2: The most common error is using K92.2 when the record contains information supporting a more specific code. Always check the entire record, especially procedure and pathology reports.
-
Missequencing Diagnoses: Incorrectly coding acute blood loss anemia (D62) as the principal diagnosis when the admission was for the active GI bleed.
-
Ignoring Causality: Failing to link a drug (like anticoagulants) to the bleed, which requires an additional external cause code.
-
Overlooking the 7th Character: Forgetting to add the appropriate 7th character (A, D, S) on codes that require it, such as those for hemorrhoids or complications of care.
11. Conclusion: The Art and Science of Accurate GI Bleed Coding
Mastering ICD-10 coding for gastrointestinal hemorrhage requires a blend of meticulous attention to detail, a solid understanding of clinical medicine, and strict adherence to official guidelines. The journey from a nonspecific term like “GI bleed” to a precise code such as K55.21 (Angiodysplasia with hemorrhage) is the essence of quality data capture. By prioritizing specificity, engaging in clear communication with providers through queries, and continuously updating your knowledge, you transform from a simple code look-up specialist into a vital contributor to the healthcare data ecosystem. Accurate coding ensures fair reimbursement, supports quality patient care through accurate data, and fuels the research that leads to better treatments for all.
12. Frequently Asked Questions (FAQs)
Q1: What is the default ICD-10 code for a GI bleed?
A: There is no true “default.” The most general code is K92.2 – Gastrointestinal hemorrhage, unspecified. However, this should only be used when the medical record provides no information to support a more specific code for the site or cause of the bleed.
Q2: When should I use K92.1 (Melena) instead of K92.2?
A: Use K92.1 when the provider specifically documents “melena” as a confirmed symptom and no more specific source of the bleeding (like an ulcer) has been identified. If the cause is known, you code the cause (e.g., K26.4) and do not use K92.1.
Q3: How do I code a GI bleed that is caused by a medication like aspirin or warfarin?
A: You would use a combination of codes:
-
The code for the specific GI bleed (e.g., K92.2).
-
A code from the T36-T50 series to identify the drug, with a fifth or sixth character of ‘5’ to indicate an adverse effect (e.g., T45.515A for adverse effect of warfarin, initial encounter).
-
A code for the underlying condition requiring the medication (e.g., I48.91 for atrial fibrillation).
Q4: A patient is admitted for a bleeding duodenal ulcer and has a very low hemoglobin. What is the principal diagnosis?
A: The principal diagnosis is the reason for the admission. In this case, the patient was admitted for the actively bleeding ulcer. Therefore, K26.0 (or K26.4) for the duodenal ulcer with hemorrhage is the principal diagnosis. The resulting anemia, D62 – Acute posthemorrhagic anemia, is coded as a secondary diagnosis.
13. Additional Resources
For the most accurate and up-to-date information, always rely on these primary sources:
-
The ICD-10-CM Official Guidelines for Coding and Reporting: Published annually by the Centers for Disease Control and Prevention (CDC) and the Centers for Medicare & Medicaid Services (CMS). This is the ultimate authority on coding rules.
-
The Current ICD-10-CM Code Set: Available through the CDC’s website and various commercial coding software.
-
American Health Information Management Association (AHIMA): Offers a wealth of resources, including practice briefs, journals, and continuing education on coding topics.
-
American Academy of Professional Coders (AAPC): Provides certification, training, and local chapter meetings for networking and education.
Date: September 23, 2025
Author: Medical Coding Specialist
Disclaimer: *This article is intended for informational and educational purposes only. It is not a substitute for professional medical coding advice, consultation, or the application of official coding guidelines. Medical coders must always refer to the most current versions of the ICD-10-CM code set, the Official Guidelines for Coding and Reporting, and consult with clinical documentation integrity specialists and physicians for accurate code assignment. The author and publisher are not responsible for any errors, omissions, or consequences resulting from the use of this information.*





