In the intricate world of healthcare, few tasks carry the weight and consequence of medical coding. What may appear to an outsider as a simple alphanumeric label is, in reality, the lifeblood of the modern medical system. It is the language of reimbursement, the data for public health initiatives, and the foundation for clinical research. Nowhere is this precision more critical than in coding complex, multi-system conditions like neurogenic bladder. A neurogenic bladder is not a disease in itself; it is a symptom, a manifestation of a deeper neurological disruption. Therefore, accurately capturing its essence in an ICD-10 code requires more than just finding the right number—it demands a deep understanding of the underlying neurology, the specific type of bladder dysfunction, and the causal relationship between the two. This article serves as a definitive guide, moving beyond basic code lookup to explore the art and science of coding for neurogenic bladder. We will dissect the ICD-10-CM index, unravel complex clinical scenarios, and illuminate the profound impact that accurate coding has on patient care, ensuring that every character in the code tells a complete and accurate story.
ICD-10 Codes for Neurogenic Bladder
2. Understanding the Neurogenic Bladder: A Primer on Pathophysiology and Presentation
The Neurology of Normal Bladder Function
To comprehend the dysfunction, one must first understand the elegant physiology of normal bladder control. The lower urinary tract—comprising the bladder (detrusor muscle) and the urethral sphincters—is governed by a sophisticated neural network often called the “spinobulbospinal reflex pathway.” This involves a delicate balance between the autonomic nervous system (involuntary) and the somatic nervous system (voluntary).
-
Storage Phase (Sympathetic Dominance): As the bladder fills with urine, stretch receptors in the bladder wall send signals via pelvic nerves to the sacral spinal cord. These signals are relayed to the brainstem (the pontine storage center), which inhibits the parasympathetic nerves and excites the sympathetic nerves (via the hypogastric nerve). This causes the detrusor muscle to relax (accommodating more urine) and the internal urethral sphincter to contract, maintaining continence.
-
Voiding Phase (Parasympathetic Dominance): When socially appropriate, the brain (the prefrontal cortex) sends a “permission” signal to the pontine micturition center. This center then inhibits the sympathetic and somatic nerves and excites the parasympathetic nerves (via the pelvic nerve). This results in a coordinated contraction of the detrusor muscle and relaxation of the urethral sphincters, allowing for complete and efficient emptying.
This complex ballet between the brain, spinal cord, and peripheral nerves is what allows for voluntary, controlled urination. A neurogenic bladder occurs when this communication network is damaged.
What is Neurogenic Bladder? Defining the Dysfunction
Neurogenic bladder is a general term for any bladder dysfunction caused by an interruption in the normal nervous system control of urination. This interruption can occur at any level: the brain (as in a stroke or Parkinson’s disease), the spinal cord (as in a spinal cord injury or multiple sclerosis), or the peripheral nerves (as in diabetic neuropathy). The resulting bladder behavior is entirely dependent on the location and nature of the neurological lesion. The consequences are far-reaching, including urinary incontinence, urinary retention, recurrent urinary tract infections (UTIs), kidney stones, and, in severe cases, permanent kidney damage (renal failure).
Key Types: Overactive vs. Underactive Bladder
While there are several classification systems, the fundamental distinction lies between an overactive (spastic/hyperreflexic) bladder and an underactive (flaccid/hypotonic/areflexic) bladder.
-
Overactive Neurogenic Bladder: This results from a lesion above the sacral spinal cord (suprapontine or suprasacral), which disrupts the brain’s inhibitory control. The bladder becomes overactive and contracts involuntarily, often with small capacity and high pressure. The patient experiences symptoms of urgency, frequency, and incontinence. This is typical of conditions like stroke, Parkinson’s disease, and spinal cord injuries above the sacral level.
-
Underactive Neurogenic Bladder: This results from a lesion at or below the sacral spinal cord or involving the peripheral nerves. The connection between the bladder and the spinal cord is severed, leading to a loss of sensation and contractility. The bladder becomes flaccid, over-distended, and unable to empty properly (urinary retention). This is seen in conditions like diabetic autonomic neuropathy, cauda equina syndrome, and lower spinal cord injuries.
3. The ICD-10-CM Coding Framework: An Overview of Structure and Logic
The International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) is a highly detailed system with over 70,000 codes. Its logic is based on etiology (cause), anatomy (location), and severity. For neurogenic bladder, codes are found in two primary chapters.
The N30-N39 Block: Diseases of the Urinary System
This chapter contains codes for the bladder dysfunction itself, which are considered manifestation codes. The most relevant block is N31: Neuromuscular dysfunction of bladder. These codes describe how the bladder is malfunctioning but not why.
The G00-G99 Block: Diseases of the Nervous System
This chapter contains codes for the underlying neurological conditions that cause the neurogenic bladder. These are the etiology codes. Examples include G35 (Multiple sclerosis), G20 (Park’s disease), and codes from the S14, S24, S34 series for spinal cord injuries.
The Importance of the 7th Character
For many codes, particularly those related to injuries (like spinal cord injuries) and their sequelae, a 7th character is required to indicate the encounter status. This is critical for accurate coding:
-
A: Initial encounter (active treatment)
-
D: Subsequent encounter (routine healing, aftercare)
-
S: Sequela (complications or conditions arising as a direct result of the initial injury)
4. Deconstructing the Primary Code: N31.9 – Neuromuscular Dysfunction of Bladder, Unspecified
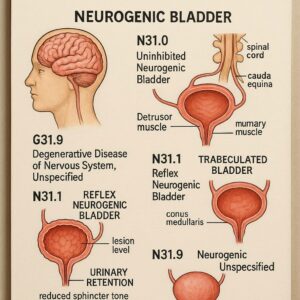
N31.9 is the most general code for neurogenic bladder. It should be used only when the medical documentation does not specify the type of neuromuscular dysfunction (e.g., the clinician simply documents “neurogenic bladder” without further qualification like “reflex” or “flaccid”).
-
When to Use It: As a placeholder when specific documentation is lacking.
-
Limitations: Using unspecified codes can lead to claim denials or down-coded reimbursements, as payers view them as incomplete. They also provide less value for data tracking. The goal of the coder and clinician should always be to provide enough detail to avoid this code whenever possible.
5. A Deep Dive into the Specific Neuromuscular Dysfunction Codes (N31.0 – N31.8)
This is where clinical documentation becomes paramount. The specific codes under N31 provide a much clearer picture of the patient’s condition.
N31.0: Uninhibited Neurogenic Bladder, Not Elsewhere Classified
This describes a condition where there is a loss of inhibitory control from the brain, leading to urgency and frequency. It is often associated with suprapontine lesions like early-stage dementia or small cerebrovascular events, but it is not classified under more specific neurological conditions. It is a less severe form of overactivity.
N31.1: Reflex Neurogenic Bladder
This is the classic overactive bladder resulting from a complete spinal cord lesion above the sacral level (e.g., a cervical or thoracic injury). The brain’s control is completely severed. The bladder empties automatically via a spinal reflex arc when it fills to a certain capacity, but this emptying is not coordinated with the sphincter (a condition known as detrusor-sphincter dyssynergia), leading to high pressure and incomplete emptying. This code is highly specific to complete suprasacral spinal cord injuries.
N31.2: Flaccid Neurogenic Bladder
This is the classic underactive bladder. It occurs with lesions that affect the sacral spinal cord, cauda equina, or peripheral nerves. The bladder is areflexic (has no reflex activity), leading to over-distention, urinary retention, and overflow incontinence. This is common in conditions like diabetic neuropathy, cauda equina syndrome, and spina bifida.
N31.8: Other Neuromuscular Dysfunction of the Bladder
This is a catch-all code for types of dysfunction not specified elsewhere. It might be used for mixed presentations or specific disorders like the non-neurogenic neurogenic bladder (Hinman syndrome), though this is rare.
6. The Crucial Role of the Etiology: Coding the Underlying Neurological Condition
Coding only the bladder dysfunction (N31.-) is telling only half the story. ICD-10-CM coding conventions and official guidelines often require that the underlying cause be coded first. This is known as the “code first” instruction. The etiology code provides the why.
Common Etiologies of Neurogenic Bladder and Their Corresponding ICD-10 Codes
| Underlying Condition | ICD-10 Code(s) | Notes and 7th Character Importance |
|---|---|---|
| Spinal Cord Injury (SCI) | S14.1-, S24.1-, S34.1-_ (Cervical, Thoracic, Lumbosacral) | The 7th character (A, D, S) is mandatory. A for acute treatment, S for long-term sequela like neurogenic bladder. |
| Multiple Sclerosis (MS) | G35 | The code for MS itself. Neurogenic bladder is a common manifestation. |
| Parkinson’s Disease | G20 | The code for Parkinson’s disease. |
| Diabetes with Neurological Complications | E11.41 (Type 2 DM with diabetic mononeuropathy) or E11.42 (Type 2 DM with diabetic polyneuropathy) | Use the appropriate code from E08-E13 with the .4x extension. Autonomic neuropathy affects the bladder. |
| Stroke (CVA) Sequelae | I69.- (e.g., I69.30 for sequelae of cerebral infarction) | The 7th character is required to indicate the sequela. Neurogenic bladder is a sequela. |
| Spina Bifida | Q05.- (e.g., Q05.9 for spina bifida, unspecified) | Neurogenic bladder is almost always present. |
| Cauda Equina Syndrome | G83.4 | This code specifically represents cauda equina syndrome. |
Sequencing: Which Code Goes First?
The general rule is to sequence the underlying etiology code first, followed by the manifestation code (N31.-). For example:
-
A patient with neurogenic bladder due to MS would be coded as G35, N31.9 (or a more specific N31 code if documented).
-
A patient with neurogenic bladder as a sequela of a spinal cord injury would be coded as S34.11AS, N31.2 (if documented as flaccid).
7. Coding Scenarios: Practical Application and Clinical Stories
Let’s apply this knowledge to real-world patient encounters.
Scenario 1: The New Spinal Cord Injury Patient
-
Clinical Picture: A 35-year-old male is admitted to the hospital after a motorcycle accident resulting in a T6 complete spinal cord injury. He is in spinal shock initially, but later develops a reflex neurogenic bladder with detrusor-sphincter dyssynergia.
-
Documentation: “Patient with complete T6 ASIA A spinal cord injury, now exhibiting signs of reflex neurogenic bladder. Will initiate intermittent catheterization program.”
-
Correct Coding:
-
S24.11XA: Injury of thoracic spinal cord, initial encounter. (Etiology, sequenced first).
-
N31.1: Reflex neurogenic bladder. (Manifestation, sequenced second).
-
Scenario 2: The Long-Term Multiple Sclerosis Patient with UTI
-
Clinical Picture: A 50-year-old female with a 15-year history of relapsing-remitting MS presents to her urologist for a follow-up. She has a known neurogenic bladder (documented as uninhibited) and now has a symptomatic UTI.
-
Documentation: “Patient with MS presents for routine management of neurogenic uninhibited bladder. Currently asymptomatic for UTI, but urinalysis shows bacteriuria. No treatment needed at this time.”
-
Correct Coding:
-
G35: Multiple sclerosis. (Etiology, first).
-
N31.0: Uninhibited neurogenic bladder. (Manifestation, second).
-
N39.0: Urinary tract infection, site not specified. (This is added because the UTI, even if asymptomatic, is documented and relevant to the encounter).
-
Scenario 3: The Diabetic Patient with Bladder Retention
-
Clinical Picture: A 68-year-old male with poorly controlled type 2 diabetes presents with complaints of difficulty urinating and a feeling of incomplete emptying. Urodynamic studies confirm a flaccid, underactive bladder consistent with diabetic autonomic neuropathy.
-
Documentation: “Patient with diabetic cystopathy due to long-standing autonomic neuropathy. Findings consistent with a flaccid neurogenic bladder.”
-
Correct Coding:
-
E11.42: Type 2 diabetes mellitus with diabetic polyneuropathy. (Etiology, first).
-
N31.2: Flaccid neurogenic bladder. (Manifestation, second).
-
8. Common Coding Pitfalls and How to Avoid Them
-
Pitfall: Coding Only the Manifestation.
-
Avoidance: Always ask, “What is the underlying cause?” Scour the record for a neurological diagnosis. If it’s present, it must be coded.
-
-
Pitfall: Misinterpreting “Unspecified.”
-
Avoidance: Use N31.9 as a last resort. If the documentation uses terms like “spastic,” “flaccid,” “reflex,” “uninhibited,” or describes urodynamic findings, a more specific code from the N31.0-N31.8 series is likely appropriate.
-
-
Pitfall: Incorrect Sequencing.
-
Avoidance: Remember the “code first” rule. The underlying condition is the primary reason for the manifestation. The etiology code should generally be sequenced first.
-
-
Pitfall: Ignoring Laterality and the 7th Character.
-
Avoidance: For spinal cord injuries and stroke sequelae, the 7th character is not optional. Using ‘S’ for sequela is crucial for accurately representing a chronic condition like neurogenic bladder that resulted from an old injury.
-
9. The Link Between Accurate Coding and Patient Outcomes: Beyond Reimbursement
Precise coding does more than just ensure payment. It creates a rich, accurate data ecosystem that directly benefits patients.
-
Data Analytics: Aggregated, specific codes allow hospitals and health systems to identify populations of patients with neurogenic bladder, analyze their outcomes, and improve care pathways.
-
Medical Necessity: Detailed codes justify the need for specialized and often expensive interventions like urodynamic studies, botulinum toxin injections, or sacral neuromodulation, ensuring patients get the treatments they need.
-
Clinical Research: Researchers rely on accurate coding to identify potential participants for clinical trials aimed at developing new treatments for neurogenic bladder and its underlying causes.
10. FAQs: Frequently Asked Questions on Neurogenic Bladder Coding
Q1: What is the most accurate ICD-10 code for neurogenic bladder?
There is no single “most accurate” code. The most precise code assignment is a combination of the specific N31.- code (e.g., N31.1 for reflex) that matches the clinical documentation, followed by the code for the underlying neurological condition (e.g., G35 for MS).
Q2: When should I use code N31.9?
Use N31.9 only when the provider’s documentation is non-specific and simply states “neurogenic bladder” without any description of its type (e.g., flaccid, spastic, uninhibited). It is always better to query the provider for more specific documentation.
Q3: How do I code a urinary tract infection (UTI) in a patient with a neurogenic bladder?
You would code both conditions. First, code the underlying neurological condition (e.g., G35), then the neurogenic bladder (e.g., N31.0), and then the UTI (N39.0). The neurogenic bladder is a risk factor for UTI, and coding it provides crucial context.
Q4: For a patient with a history of spinal cord injury who is being seen specifically for management of their neurogenic bladder, what 7th character should I use for the spinal cord injury code?
You should use the 7th character ‘S’ for sequela. The encounter is for the long-term management of a condition (neurogenic bladder) that is a direct result (sequela) of the old spinal cord injury.
11. Conclusion: The Art and Science of Precision Coding
Accurate ICD-10 coding for neurogenic bladder is a critical skill that bridges clinical care and healthcare administration. It requires a diligent review of clinical documentation to identify both the specific type of bladder dysfunction and its underlying neurological cause. By moving beyond unspecified codes and meticulously applying the principles of etiology and manifestation coding, healthcare professionals ensure proper reimbursement, contribute to valuable health data, and ultimately, support the delivery of high-quality, patient-centered care for individuals living with this challenging condition.
12. Additional Resources
-
Official Source: The CDC’s ICD-10-CM Official Guidelines for Coding and Reporting: https://www.cdc.gov/nchs/icd/icd-10-cm.htm
-
Professional Organization: The American Academy of Professional Coders (AAPC): https://www.aapc.com/ (Offers resources, training, and certifications).
-
Clinical Reference: The American Urological Association (AUA): https://www.auanet.org/ (Provides clinical guidelines on the diagnosis and treatment of neurogenic bladder).
-
Patient Support: The National Association for Continence (NAFC): https://www.nafc.org/ (A valuable resource for patient education and support).
Date: September 23, 2025
Author: Medical Content Specialist
Disclaimer: This article is for informational purposes only and is intended for healthcare professionals and medical coders. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult the most current, official ICD-10-CM coding guidelines, payer-specific policies, and the patient’s complete medical record before assigning codes. The author and publisher are not responsible for any errors or omissions or for any outcomes related to the use of this information.





